 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
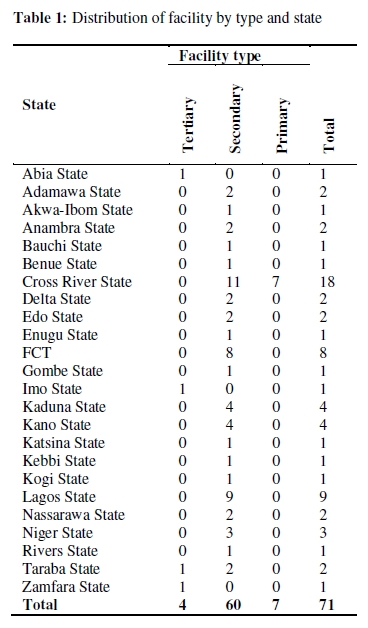
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 109-116 ORIGINAL RESEARCH ARTICLE Integrating Reproductive Health and HIV Indicators into the Nigerian Health System – Building an Evidence Base for Action Integration de la sante de la reproduction et les indices du vih dans le systeme de la sante publique: L’etablissement d’une base d’evidence pour l’action Ogo Chukwujekwu1, Nzapfurundi Otto Chabikuli1,2, Mike Merrigan1, Dorka Awi1 and Christoph Hamelmann1 1Family Health International/Global HIV/AIDS Initiative Nigeria, Plot 1073-A1 GODAB Plaza, J.S. Tarka Street, Area 3, Garki, P.M.B. 44, Abuja, Nigeria; 2Department of Family Medicine, Faculty of Health Sciences, University of Pretoria, HW Snyman Building, 31 Bophelo Road, Riviera, Pretoria For correspondence: Tel: +234-9-4615569 Email: ochabikuli@ghain.org ABSTRACT The lack of integrated M&E system makes it difficult to assess the effectiveness of HIV and family planning (FP) service integration. Since 2007, Nigeria integrated FP and HIV M&E systems. A pre-post survey compared the availability and use of FP-HIV integration M&E tools six months pre-and 12-months post-integration in 71 health facilities supported by the Global HIV/AIDS Initiative Nigeria (GHAIN). Pre-integration, four facilities (6%) had national FP registers, 32 (45%) had monthly aggregated FP data and 33 (46%) reported data up to national level. Post-integration, all (100%) facilities used national FP register with FP-HIV integration indicators, and reported data up to national level. Sixty six facilities (93%) had at least one monthly supervisory visit. Average number of FP clients per facility referred for HIV testing increased from five in the first month to 15 by month 12 postintegration. Leveraging resources of HIV programs improved significantly the monitoring of FP-HIV services integration (Afr J Reprod Health 2010; 14[1]:109-116). RĖSUMĖ Le manque de système de la S & E intègre, le rend difficile à évaluer l’efficacité de l’intégration du service du VIH et de la planification familiale (PF) Depuis 2007, le Nigéria a intégré la PF et le les systèmes de surveillance et d’évaluation (S & E). Une enquête faite avant et après l’intégration a comparé la disponibilité et l’emploi des outils de l’intégration de la S & E et de la PF – VIH six mois avant et 12 mois après l’intégration dans 71 établissements de santé soutenus par Global HIV/AIDS Initiative Nigéria (GHAIN). En ce qui concerne pre-intégration, quatre établissements (6%) avaient des registres de la PF nationale, 32 (45%) avaient des données mensuelles totales de la PF et 33 (46%) ont signalé les données jusqu’au niveau national. Pour ce qui est de la post-intégration, tous les établissements (100%) se sont servis du registre de la PF nationale avec les indices de l’intégration PF – VIH et ont signalé les données jusqu’au niveau national. Soixante-six établissements (93%) avaient au moins une visite de surveillance par mois. Le nombre moyen des clients de la PF dans chaque établissement qui ont été orientes vers des établissements pour le test pour le VIH a augmente de 5 le premier mois jusq’au 15 dans le 12ième mois de la post intégration. Les ressources destinées aux programmes du VIH ont amélioré de manière importante les services de la moniteur et de la PF – VIH intégration (Afr J Reprod Health 2010; 14[1]:109-116). KEYWORDS: Family planning, HIV, integration, monitoring and evaluation Introduction Nigeria has the largest population in Africa. With a fertility rate estimated at 5.5%, and a population growth estimate of 2.6% per year, its population of 140 million will double within 24 years 1. Nigeria has low contraceptive prevalence rate amongst married women of reproductive age and unmet need for contraceptives, estimated at (12.6% for all methods, 8.2% for modern methods), and 17% respectively2 . The HIV prevalence in Nigeria was 4.6% in 20083. Approximately 3 million people live with HIV/AIDS (PLWHA)4. An increase in access to reproductive health (RH) and family planning (FP) services in particular for HIV positive women would prevent an estimated 8,158 unintended HIV positive births annually in countries receiving funds from the President’s Emergency Fund for AIDS Relief (PEPFAR)5. Enormous resources have been channeled into HIV treatment and care in Nigeria in recent years, but HIV prevention efforts, including those promoting sexual and reproductive health, have fallen behind6. A paradigm shift has now occurred globally with international bodies recognizing and calling for the integration of FP and HIV services7. The debate on FP-HIV service integration has gone beyond the merits of integrating the services to focus on the complex practicalities of implementation as well as monitoring and evaluation (M&E) of success8. The integration of FP and HIV services has been shown to be feasible and effective in Nigeria 9. While there has been progress in FP-HIV service integration globally, the M&E of this integration has lagged behind [10]. Three factors however impede M&E of FP-HIV integration: i) the vertical design of the M&E systems of HIV and FP; ii) the lack of FP-HIV integration indicators; and iii) shortage of human resources adequately skilled and motivated to implement the integrated M&E system. Indicators for monitoring HIV programs are well established and guidelines for national agencies have been in existence since 2000, while indicators and guidelines for monitoring national reproductive health programs have been available since 199711,12. Although indicators for integrated FP and sexually transmitted infection (STI) treatment services were published in 200213 , a literature search revealed only one substantive attempt to define potential indicators for RH/FP and HIV service integration efforts 14 . However, these indicators were not linked to guidelines data for collection, and have not yet been field tested. In February 2008, a meeting in Addis Ababa to launch the “Mobilizing for FP-HIV Integration” initiative re-emphasized the need for a common set of indicators to track integrated services 15,16 . The introduction of these indicators must take into consideration the field challenges of the developing countries’ public health sectors. In Nigeria the FP-HIV integration occurs in the context of a weak health information system, characterized by a paucity of data at different levels, multiple data pathways (vertical “silos”), inadequate quality control methods, and a focus on “bean counting” as opposed to using data for decision-making17. In the Nigerian public sector, FP and HIV services in general hospitals and primary health care (PHC) clinics are provided by generalist doctors and nurses. In the past few decades, the Nigerian health system has been negatively affected by the international brain drain 18. The shortage of staff and de-motivation among health care workers at PHC and secondary level is common in Nigeria19,20 . Against this backdrop, clinical work, perceived as core function, is often prioritized to the detriment of administrative and M&E tasks in public health facilities. The disproportionately high funding for HIV programs in Nigeria, a PEPFAR focus country, has secured dedicated resources within health facilities, including staff. In 2008, Nigeria received US$ 447.6 million from PEPFAR alone, making it the third largest recipient of PEPFAR funds in the world. These funding levels carry expectations that HIV programs generate timely, standardized and good quality data. As a result, the HIV component of the health management information system (HMIS) functions better than FP programs, where the availability of national service statistics is hampered by the use of unstructured or customized data collection tools in many facilities, and insufficient resources devoted to ensuring that data are aggregated and received at higher levels. In Nigeria, contributing to the knowledge base on the M&E of FP-HIV integration requires more than deriving indicators -the entire system inclusive of data collection, aggregation and transmission must be addressed. This paper evaluates a two pronged intervention that leverages resources of HIV programs to improve the availability and use of FP-HIV M&E tools in FP clinics by: i) training and jointly supervising staff in FP and HIV clinics; and ii) introducing FP-HIV integration indicators in the Nigerian national FP register. An earlier publication to evaluate the integration of FP and HIV services in 40 GHAIN-supported facilities had an observation period of six months pre-and six months post-integration9. This paper expanded on that dataset to i) cover an observation period of 12 months post-integration, long enough to offer insight on sustenance of service output and supervision and ii) included the measurement of the frequency of supervision per facility. Methods FP-HIV service integration Between March 2007 and April 2009, the Family Health International’s (FHI)/ Global HIV/AIDS Initiative Nigeria (GHAIN) project supported the integration of FP and HIV services in 71 public sector health facilities in 24 states of Nigeria (Table 1). The HIV service points within facilities include the anti-retroviral therapy (ART) clinic, the HIV counseling and testing centre (HCT) and the PMTCT clinics, including antenatal clinics (ANC). One of the facilities provided only HCT and FP services. Seventy facilities had PMTCT and HCT services, 46 of which provided ART services, in addition to PMTCT and HCT. In Nigeria, FP services, like HIV services, are usually delivered in specialized, separate units (service delivery points) within primary, secondary and tertiary facilities. GHAIN has supported an FP-HIV integration strategy centered around a bi-directional referral mechanism to link PLWHA from HIV service points to FP service points within a health facility, and vice versa. The integration efforts focused on training staff in health facility including on M&E system, with no major structural changes. Providers at HIV service points received FP training while their family planning counterparts received training on the reproductive health needs of PLWHA. The last day of the integrated training was devoted to M&E tools. Materials developed to support FP-HIV integration included standard operating procedures (SOP), job aides and quality assurance tools. Providers also received monthly support supervision visits jointly conducted by the relevant state ministry of health and GHAIN staff. During these visits, providers in HIV clinics were encouraged to offer and record routinely family planning counseling to clients at three HIV service points and referral of acceptors to the FP unit for access to commodities. In addition, providers in FP clinics were encouraged to counsel and record routinely FP clients for HIV testing and refer acceptors to HCT centers, or in a few cases, provide testing at the FP unit. FP-HIV M&E integration The nature of the service integration strategy guided revisions to the national FP register, which in turn informed the selection of FP-HIV integration indicators used in Nigeria. The emphasis was on keeping changes to the existing tools to a minimum so as to limit the reporting burden on the already scarce staff capacity. Four columns were added to the FP register to capture completed referrals from any of the three HIV service points (i.e. HCT, PMTCT and ART) to FP clinics within the facility and referrals from FP clinics to the HCT service points (or HIV counseling and testing done at FP clinic where applicable). Minor adjustments were also made to the ANC register in PMTCT service point and HCT register to record the provision of counseling on FP. HCT registers were introduced at FP clinics to record HIV testing conducted there. Adjustments to these tools were made through a technical working group led by the Federal Ministry of Health. These revised registers were introduced together with a standard monthly summary form aggregating the combined FP and FP-HIV datasets. The following FP-HIV integration-specific data elements are now generated on a monthly basis at each facility:
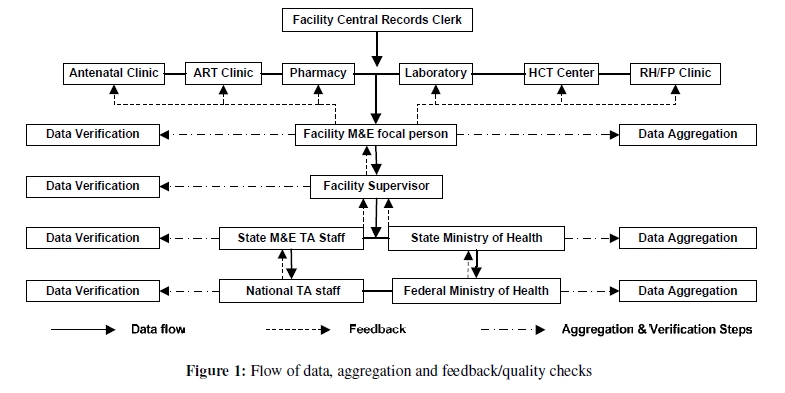
Within the broader mandate of the national HMIS, key structural components of the more advanced HIV M&E system were used to inform the FP-HIV integrated M&E system (Figure 1). Each facility had a trained M&E focal person, often a medical records officer, who was responsible for overseeing the aggregation and onwards reporting of data from each service delivery point. Following FP-HIV service integration, M&E focal persons, together with FP counselors, were trained on this additional dataset. FP-HIV data were collected, summarized and reported to state level alongside data from other HIV service points. The M&E officers in each state added the RH-FP unit in the facility to their schedule of monthly data verification visits. At state level, the verified data was computerized in the Nigerian Ministry of Health’s HMIS database, and data analysis outputs were generated and discussed at monthly M&E meetings. Evaluation design The study was a pre-post, retrospective survey of the availability and use of FP-HIV integration M&E tools, comparing a six months period before FP-HIV integration with a 12 months period following integration of services in all the 71 GHAIN-supported health facilities between March 2007 and April 2009. The following six outcome variables were derived from the aggregated monthly service statistics and reports from routine supervision visits to the sites:
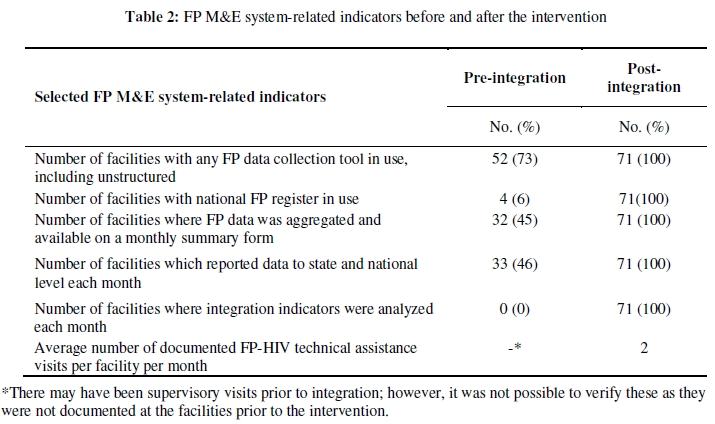
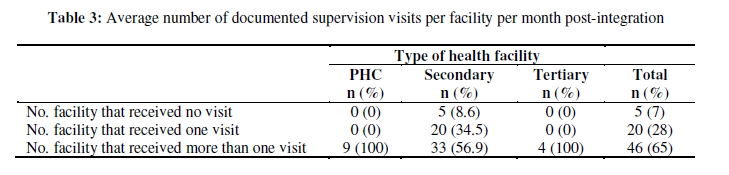
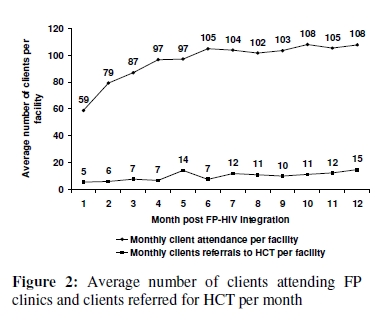
Data for the period before integration were sourced from a review of registers (structured or unstructured) and other M&E tools in use at the facility pre integration. Data on routine service statistics, including supervision, were collected from the District Health Information System (DHIS), the national platform for routine HMIS in Nigeria. Data entry was carried out in Microsoft Excel. All facilities where FP-HIV service integration was operational were included in the analysis. The calculation of frequencies for all outcome measured pre-and post-integration were carried out using Stata 10 (StataCorp). The frequency of monitoring visits per facility was also calculated by facility level. Monthly average numbers of clients referred from the FP clinic to the HIV clinic for testing was calculated and presented graphically. Results All 71 health facilities (four tertiary hospitals, 60 secondary hospitals and seven PHC centers) provided both FP and at least HCT in an integrated manner during the observation period. Fifty two (73%) of the facilities had data collection tools of any kind, including unstructured registers, before integration, while only four (6%) had the national FP register (Table 2). The information from unstructured tools is used mainly for FP commodity stock management and procurement (user charge applies to FP commodities in Nigeria). Prior to FP-HIV integration, only 32 facilities (45%) had aggregated FP data on monthly basis and 33 (46%) reported FP data to the state and national level monthly. None had FP-HIV integration indicators. By the 12th month post integration, a total of 426 health care providers had been trained in the 71 facilities on FP-HIV integration and M&E, an average of six staff per facility. Sixty six facilities (93%) had at least one structured supervisory visit per month from government officials, with technical assistance from GHAIN staff. Forty six facilities (65%) had two or more such visits per month. The average number of monthly supervisory visits was zero for five (7%) secondary hospitals. Twelve months after integration, all 71 facilities had and used the revised FP national register with FP-HIV integration data elements. The percentage of facilities aggregating integration data each month, and reporting it to state/national level, increased from 44% and 46% to 100% respectively. Charts were produced from monthly aggregates from all 71 facilities and were analyzed during meetings with facility M&E focal persons (Table 3). In the post-integration period, FP data, as well as the FP-HIV data elements were incorporated into state and national program management mechanisms and used to inform decision-making. In addition to FP specific data elements such as attendance at FP clinic and uptake of FP methods, all facilities now report on the number of FP clients referred for HIV counseling and testing. There was a steady increase in the average attendance at FP clinics from 59 clients in the first month to 108 in month 12 post integration. However, counseling and referral for HIV testing was low among FP clients. The number of clients counseled and referred to HIV clinics increased three-folds from a mean of five clients per facility per month in the first month of integration to 15 clients in the twelfth month (Figure 2). Thirty-nine facilities provided HCT at the FP clinics. In the post-integration period, a total of 2,372 FP clients were counseled, tested for HIV and received results at the FP clinic. Discussion This study demonstrates how leveraging investments in a large HIV/AIDS program’s M&E system led to improved routine M&E of FP program in Nigeria. Within six months of integration, all facilities in the study had embraced the revised FP register, used them daily, aggregated data monthly and data were analyzed. The alignment with the existing national FP register alone was not sufficient. Ongoing supervision was an important factor needed to ensure that health care providers understand the importance of FP-HIV service integration and the subsequent recording and reporting of these services. This supports the suggestion that HIV programs have the potential to strengthen the HMIS in developing countries21 . One limitation of our study is the absence of control sites, which makes it difficult to assess the possible contribution of external factors to the observed improvement in system indicators. Despite this limitation, several important lessons have been learned in the process of designing an M&E system for FP-HIV integration activities. The selection of indicators needs to be guided by the nature of the service integration model, with additional data requirements kept at a minimum and obtained through revisions to existing national tools where possible. Adopting this principle enabled our M&E integration effort to be acceptable to facility staff: the integration was not a separate, additional burden for health care workers and supervisors. Data quality is a major concern in scaled up HIV programs in developing countries22. There is evidence that data quality improves with better staffing and supervision in HIV programs23,24. While supervision is very beneficial in the context of PHC, its cost is often unaffordable for ministries of health25. Continued advocacy to the relevant levels of government for increased and sustained funding for supervision of health facilities is necessary. Ninety percent of facilities in our study benefited from at least one supervisory visit per month, and all FP clinics received support from the facility M&E focal person from the HIV program. This supervision, in addition to the minimal data requirements, helped ensure that data was properly recorded, aggregated and reported upwards. As a result of improved recording and reporting on FP-HIV data, information on the uptake of HIV testing in FP clinics is now available. Although the referral of FP clients for HCT increased from an average of 5 referrals in the first month to 15 in month 12 post-integration, the numbers are still low compared to the total attendance at FP clinics. It can be argued that the uptake of HIV testing by FP clients may be increased if HCT was offered at the FP clinics (a one-stop shop), rather than referring clients to the HCT service points26. Referral implies additional waiting time for a relatively healthy population. Furthermore, separate HIV clinics are stigmatizing, an additional disincentive to complete referral. In conclusion, this study provides some insight into the utilization of FP commodities and services by clients of HIV services, and vice versa; however, the real benefit of this new evidence generated by the integrated FP-HIV M&E will lie in its systematic incorporation into existing government mechanisms for reviewing health service utilization statistics, and utilization in planning so that resources are channeled where needed most. Support supervision is an effective means of embedding interventions in public health services of developing countries and ensuring compliance with quality standards. The public health sector however does not always have the resources to sustain support supervision. The leveraging of support supervision resources from well funded disease control programs such as HIV and malaria has the potential to expand beyond FP-HIV and strengthen the general HMIS in developing countries. References
The following images related to this document are available:Photo images[rh10009f2.jpg] [rh10009t2.jpg] [rh10009t3.jpg] [rh10009t1.jpg] [rh10009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}