 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
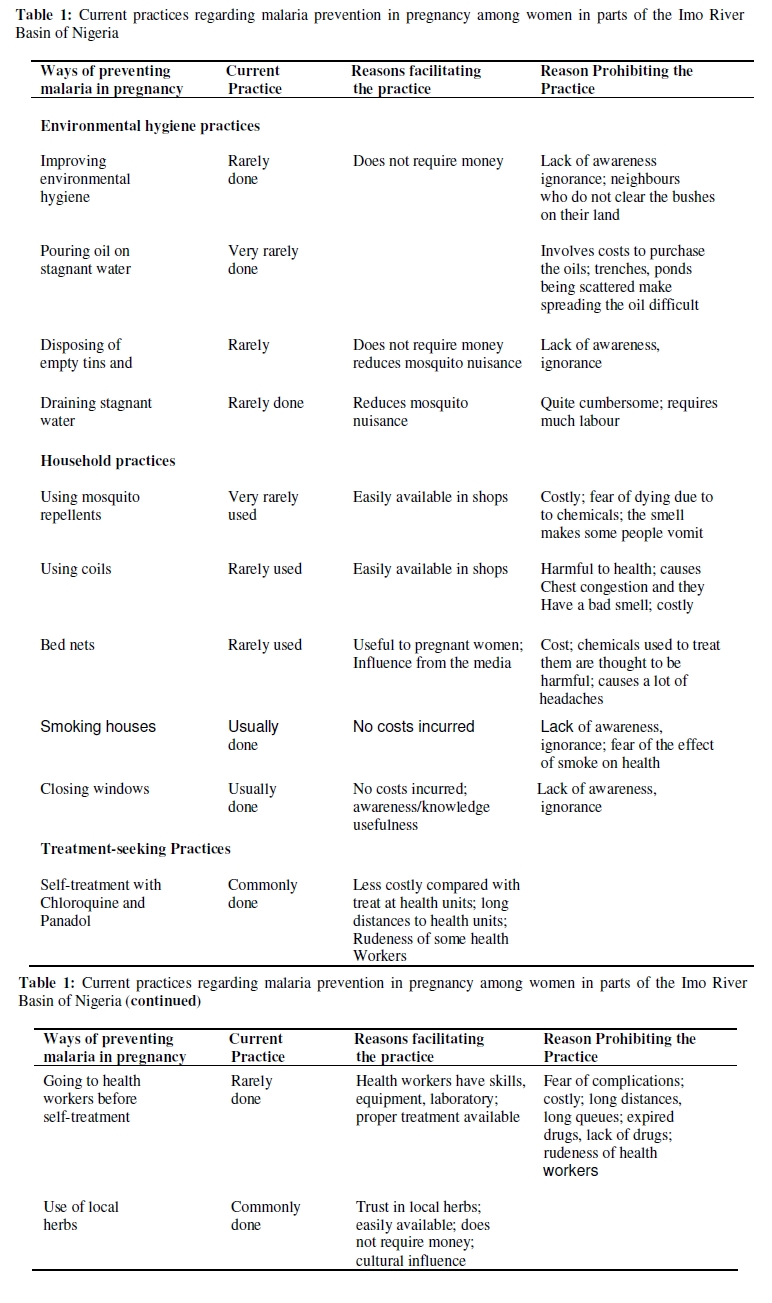
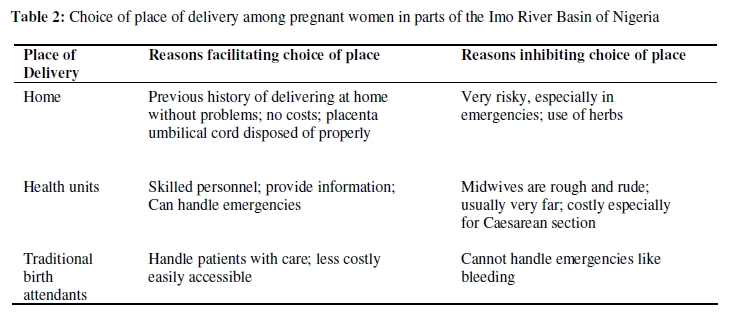
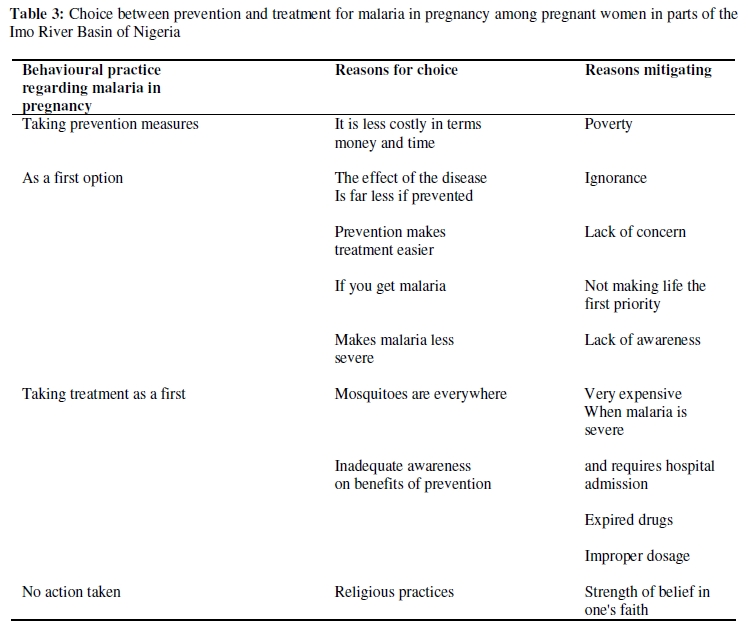
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 117-128 ORIGINAL RESEARCH ARTICLE Perceptions on the Use of Insecticide Treated Nets in Parts of the Imo River Basin, Nigeria: Implications for Preventing Malaria in Pregnancy Perceptions sur l’emploi des moustiquaires imprégnés d’insecticide dans la région du bassin du fleuve Imo, Nigeria: Implications pour la prévention de la malaria pendant la grossesse Chukwuocha UM1*, Dozie INS2, Onwuliri COE3, Ukaga CN4, Nwoke BEB4, Nwankwo BO1, Nwoke EA1, Nwaokoro JC1, Nwoga KS1, Udujih OG1, Iwuala CC1, Ohaji ET1, Morakinyo OM1 and Adindu BC1 1Department of Public Health Technology, Federal University of Technology, Owerri, Imo state Nigeria; 2Department of Microbiology, Imo state University, Owerri, Imo State, Nigeria; 3Department of Biotechnology, Federal University of Technology, Owerri Imo State Nigeria; 4Department of Animal and Environmental Biology, Imo State, University, Owerri, Imo State Nigeria. *For correspondence: Email: chukwuochauchem@yahoo.com ABSTRACT This study aimed at assessing perceptions on use of ITNs in parts of the Imo River Basin, Nigeria and its implications in preventing malaria in pregnancy. Data was collected using focus group discussions, key informant interviews and structured questionnaires. Results showed high awareness on the benefits of ITNs. Factors affecting use of ITNs included its high cost, perceptions of chemicals used to treat them as having dangerous effects on pregnancy, low utilization of antenatal care, husband’s lack of interest in malaria prevention and perceptions that adolescent girls are at low risk of getting malaria. The implications of these findings include demystifying the negative perceptions on the chemicals used for net treatment and subsidizing the cost of ITNs to increase access. These findings provide important lessons for malaria programmes that aim at increasing access to ITNs by pregnant women in developing countries (Afr J Reprod Health 2010; 14[1]:117-128). RĖSUMĖ Cette étude avait pour but d’évaluer les perceptions sur l’emploi des MIIs dans des régions du bassin du fleuve Imo, Nigeria et ses implications dans la prévention de la malaria dans la grossesse. Les données ont été collectées à l’aide des discussions à groupe cible, des interviews auprès des informateurs et des questionnaires structurés. Les résultats ont montré une conscience élevée des avantages des MIIs. Parmi les facteurs qui affectent l’emploi des MIIs sont le coût élevé, la perception des produits chimiques utilisés pour les traiter comme ayant des effets dangereux sur la grossesse, la faible utilisation des soins prénatals, le manque d’intérêt chez le mari dans la prévention de la malaria et des perceptions selon lesquelles les filles adolescentes courent un faible risque d’attraper la malaria. Les implications des ces résultats comprennent la démystification des perceptions négatives sur les produits chimiques qu’on a utilisés pour le traitement du moustiquaire et la subvention du coût des MIIs pour augmenter l’accès. Ces résultats donnent des leçons importantes pour des programmes de la malaria qui visent l’augmentation d’accès aux MIIs par les femmes enceintes dans les pays en voie de développement (Afr J Reprod Health 2010; 14[1]:117-128). KEYWORDS: Malaria, Insecticide Treated Nets, Mothers, Pregnancy, Prevention, Perceptions Introduction In most countries of sub-Sahara Africa, malaria is highly endemic and due to repeated exposure to malaria infection, people develop a certain degree of immunity to it during the first decade of life1, 2 . Despite this immunity, pregnant women, especially primigavidae, have a higher susceptibility to Plasmodium falciparum infection, manifested by a higher prevalence and intensity of parasitaemia 2, 3 . The serious consequences of malaria in pregnancy are attributed to the sequestration of malaria parasites in the placenta, leading to impeded trans-placental nutrient transport. This, combined with malaria induced anemia, compromises foetal growth and result in low birth weight (LBW) and a subsequent increase in infant and childhood mortality4 -6, 3. As much as 50% of low birth weight (LBW) among primigravidae has been attributed to malaria in some malaria endemic areas1. A number of studies have found that insecticide treated nets (ITNs) provide varying degrees of protection against malaria morbidity, anemia and LBW 7. In a trial of untreated bednets in the Gambia, nets were found to reduce the number of infective bites but not enough to reduce morbidity from malaria 8. Following this study, however, it was shown that irrespective of ethnic group, area, habitat and distance from the River Gambia, malaria prevalence decreased with use of ITNs 9, 10. The main reason for this was that mosquitoes were not only kept away from the sleeping people, but would die when they came in contact with the insecticide. In subsequent studies, it was demonstrated further that use of ITNs in pregnancy reduces malaria parasitaemia, anemia and premature deliveries, increases mean birth weight and subsequently reduces neonatal and infant mortality11, 12. ITNs have a mean protective efficacy against malaria episodes of approximately 50% in highly endemic areas of Africa 13 and have also been found to reduce overall mortality among children by 63% in villages using impregnated nets 14 . A recent review has similarly shown that ITNs are highly effective in reducing morbidity and mortality from malaria 15 . Bed nets given to pregnant women have been found to be protective to women and their children against malaria in both high and low malaria transmission areas of Kenya 16, now WHO recommends that in malaria endemic areas, all pregnant women should receive malaria chemoprophylaxis and sleep under ITNs 17. Further to this recommendation, in the year 2000 African countries initiated the Roll Back Malaria strategy to control malaria in the Continent. This recommended increased access to chemoprophylaxis and use of ITNs by pregnant women and children 18 . Following the above recommendations, Nigeria’s policy on prevention of malaria in pregnancy recommends two doses of chloroquine as intermittent preventive treatment (IPT) in the second and third trimester of pregnancy for women of all parities. The policy also advocates that pregnant women should use ITNs. A recent review on community acceptance of bed nets has shown that various factors influence the use of bed nets, including cultural, behavioural and demographic factors, ethnicity, accessibility, gender relations and seasonality of malaria 7. Several authors have concluded that although ITNs are effective, local perceptions, acceptance of and use of ITNs as well as use of other mosquito methods are invaluable in malaria control programmes 10, 19, 20. It is also known that even if ITNs are purchased and used correctly, they must be recognized and accepted. Further to this, the local acceptance of the insecticide may be influenced by its toxicity, the local terms used to translate the chemical and the meaning attached to these terms 20 . Current use of malaria preventive measures during pregnancy in Nigeria is low, and calls for serious consideration. Perceptions on the use of ITNs and other malaria preventives have been conceptualized based on the Health Belief Model developed by Becker 21 . In this model, two main factors influence the likelihood that a person will adopt a recommended preventive action. First, a person must feel susceptible and threatened by the disease, with perceived serious consequences. Secondly the person must belief that the benefits of practicing prevention outweigh the perceived barriers to the preventive action. Therefore, four constructs can be derived from this model: perceived susceptibility, perceived severity, perceived benefits and perceived barriers. The selection of this model to analyze the treatmentseeking pattern for malaria in pregnancy is based on its previous use to predict a number of healthrelated behaviours like engaging in exercise 22 ; Child vaccination 23 and compliance with recommended medical regimens 24 . In addition, the model construct have been found to have a high correlation with health-related behaviours 25 . Materials and Methods Study Area The study was conducted in three local government areas viz, Ahiazu Mbaise, Aboh Mbaise and Ezinihitte Mbaise Local Government Areas (LGAs) within the Imo River Basin of Imo State Nigeria. The LGAs lie between latitude 5010l and 5051l north and longitude 6035land 7028l east with a population density of 161 people/per km2. The area has a high fertility rate of 6.2 births per woman. Farming is the main occupation of the local inhabitants mainly at the subsistence level. The climate and topography together with human activities in the area seriously encourage malaria transmission. Data Collection Data were collected using qualitative methods including focus group discussions (FGD) and key informant interviews (KII). The following thematic areas were explored: perceptions on susceptibility and seriousness of malaria in pregnancy; perception on use of malaria preventive interventions. Study participants from different target population groups were selected from each of the LGAs taking into consideration their age, education, socioeconomic and marital status. This approach enabled data collection from a range of people in order to get the broad picture necessary for a review of the policy for malaria prevention in pregnancy. FGDs were held separately with pregnant women aged 20-49 years adolescent girls (both those out of school and those in school) aged 10-19 years and men aged 20-50 years. A total of 10 FGDs were conducted, with a total of 90 participants: 15 adolescents aged 10-19 years, 36 young women aged 20 -29 years and 39 men aged 20-50 years. Sixty-three participants had attained some primary education while 27 had secondary education and above. Sixty-eight were married and engaged in peasant agriculture and petty trade. In addition to the FGDs, 40 KIIs were conducted targeting opinion leaders, local government officials, elderly midwives, retired women leaders, drug shop owners, traditional birth attendants, pregnant and non pregnant women. Results Perceptions on Susceptibility and Seriousness of Malaria in Pregnancy Malaria in this area is known locally as “Ida” or “Akum” (fever with body weakness) and is perceived as the leading cause of ill health among children and pregnant women. The main reasons given by participants as to why pregnant women and children are vulnerable to malaria was that their bodies are weak, a reference to low immunity against disease. In this area, adolescents, primigravidae and men were not perceived to be at risk of malaria. The study explored health-seeking behaviour among adolescents as an important group to target for malaria prevention. All participants in the 10 FGDs and all the key informants interviewed considered adolescents and primigravidae as people at no special risk from malaria. Over three-quarters of participants in all the FGDs including those with adolescents themselves, perceived pregnant adolescents as a group least likely to use health services like antenatal care: and it was also reported that nonpregnant adolescents were the group least likely to use existing health services. This is because the main response to pregnancy among adolescents is to try to have an abortion, by whatever means. Generally, adolescents do not want their parents to know that they are pregnant. They also fear being dismissed from school when it becomes known that they are pregnant. Their fear drives them underground and limits their access to treatment and preventive services. The expressions below illustrated this fear: “Pregnancy in adolescent brings conflict between parents and the girl, parents mistreat girls who get pregnant, and the girl may feel bad and resort to abortion. I may consult my parents to give me help and if they chase me to go to the man responsible for the pregnancy, who may be poor, I may decide to go and Consult. I know how to abort; I know some herbs which can cause abortion. To abort I can go to a drug shop and buy some pills” (18-year old adolescent in Ahiazu Mbaise LGA). “When you do not attend antenatal care at health units and you go to deliver at health units, midwives cannot deliver you” (20year-old pregnant woman at Eziudo Ezinihitte Mbaise LGA). Our analysis indicates that pregnant adolescents realize the importance of seeking preventive care for malaria compared with nonpregnant adolescent. However, although there are several constraints that limit access to services, like stigma against adolescent pregnancy and the negative attitude of health workers. In further discussions with adolescents, it was revealed that the common source of information for adolescents is their peers. Through information sharing, adolescents were aware of the dangers of getting pregnant, and they also know that young people are not yet prepared to carry the stress of pregnancy. However, they did not know the danger malaria poses to pregnant adolescent and how to prevent it. Perceived Benefits and Barriers Related to Use of ITNs In all the FGDs and the KIIs conducted, participants and key informants knew that mosquito nets were a useful preventive measure against malaria, and that pregnant women and children were supposed to sleep under nets since they are the most vulnerable groups. However, the availability and use of the nets in this area was found to be very low. Over three quarters of participants in all the FGDs and KIIs reported that very few people in the area use mosquito nets for example: “For us here we do not use mosquito nets…I also do not have one” (17-year-old adolescent Amumara in Ezinihitte Mbaise LGA). Furthermore, the following statement illustrates the perceptions on the availability of mosquito nets in this community: “For me I have lived in this area for long, I have never known any one using a mosquito net” (24-year-old woman at Amuzu in Aboh Mbaise LGA). The factors associated with how use of ITNs were explored by asking participants and key informants what constraints exist to the prevention of malaria with ITNs. In all the 10 FGDs and the KIIs conducted, it was emphasized that the cost of ITNs followed by their nonavailability were constraints to their use. Similarly, over half of participant in all the 10 FGDs thought that the chemicals used to treat the nets were very harmful to adults, children and pregnant women. This fear was confirmed by key informants who said this was a widely held perception in the community. People in this community had heard from the radio that bed nets are treated with chemicals which kill mosquitoes. In all the FGDs conducted, the name and type of the chemical was not known, neither did it have any local terminology. The difference between treated and non-treated net was also not known. People believed that all nets were treated with a chemical. Over half of the participants in all FGDs seemed to believe that ITNs are treated with chemicals which affect pregnant women, especially their breathing, and that if the chemicals can kill mosquitoes instantly, they can also kill people. We explored whether this perception was held mainly by non-users, although users also believed it in addition to reporting the feeling of excessive heat and suffocation at night due to use of ITNs. The quote below summarizes the fear of chemicals used to treat nets: “We fear we may die because these chemicals are poisonous” (35-year-old woman at Nguru in Aboh Mbaise LGA). Another constraint mentioned by over threequarters of women participants in all FGDs was uncaring husbands. Men were expected to care for their spouses in all aspects, including helping them to seek treatment and prevention for malaria, such as paying for ITNs. In this regard, the expressions below show men’s perceptions on their vulnerability to malaria and how this may influence their attitude towards malaria treatment and prevention. “We leave them (nets) to women and children because as we told you, men are resistant, we have strong blood” (35-year-old man at Ogbe in Ahiazu Mbaise LGA) “Malaria nets are not a priority to people in this area, people (mainly the men) would rather use the money to buy net to drink” (32-year-old non-pregnant woman Lude in Ahiazu Mbaise LGA). Despite the above expression from a male participant, over three quarters of women in all FGDs complained that men did not care about the health of their wives and their children. Men were reported not to prioritize the issue of health, as the latter quote above shows. Women thought that men use their money on items like alcohol and forget about buying nutritious foods and providing health care to their families. Women participants at Ezinihitte Mbaise LGA said that they fear to buy mosquito nets because their husband would question them about the source of the money. This is because women in this community are not expected to have money, the husbands feel obliged to know its source. More than half of women participants in all the FGDs expressed fear that if a woman bought a net, the husband would suspect that she got the money from another man. In addition to the fear of the chemicals used to treat ITNs and the cost of purchasing them, the few respondents who used ITNs complained of too much heat and discomfort experienced while sleeping under the nets. “For me I use it but I feel like suffocating. It brings a lot of heat” (35-year-old woman at Itu in Ezinihitte LGA). “Some pregnant women say that mosquito nets cause a lot of heat and discomfort, yet they want to relax at night but the nets limit them”. (17-year-old adolescent at Aboh LGA) From the study findings, it was reported that very many households in the study area use mosquito repellents although mainly targeted at mosquito nuisance and not malaria. The study explored perceptions related to their use, especially by pregnant women. The common household mosquito repellents were known by their trade (brand) names as Raid, Shelltox and Mobil. In all FGDs conducted, participant said that these repellents have a bad smell that makes pregnant women vomit. This belief was expressed by women who had been pregnant before and had experienced the bad smell. Over two-thirds of the female participants in all FGDs expressed fear that the chemicals in the mosquito repellents could be harmful to pregnant women, health and foetus. If she breathed them the foetus in the womb would die. On further exploration, it was found that this fear was not based on evidence of severe outcomes due to use of mosquito repellents. It was also noted that burning of mosquito coils causes difficulty in breathing. The experience was expressed by eight respondent in two of the 10 FGDs conducted. However, a majority of key informants (over two-thirds) did not express this fear, indicating a difference in awareness among respondents regarding this preventive measure. Sources of Information on Prevention of Malaria in Pregnancy The common source of information on malaria prevention in pregnancy is the radio, followed by health workers, newspapers, pastors, meeting in local communities and peers, especially among adolescents. Television was mentioned by a few participants (less than a quarter) as a source of information in eight of the 10 FGDs. Over three-quarters of participants in all FGDs mentioned that they trusted information from health workers because health workers are knowledgeable and can reach the people and provide face to face explanations. However, radio messages are also trusted because for many years the radio has been a source of official and authoritative information in Nigeria with a wide coverage. Almost all participants (about nine out of 10) in all the FGDs and all the key informants had heard several messages on malaria treatment and preventions. The messages covered the benefits of sleeping under ITNs, and improving environmental hygiene to prevent breeding of mosquitoes. A few participants (less than a third in all FGDs conducted) had heard that fansidar can be used as a preventive measure during pregnancy, and these were people who had previously used it. Perception on Other Malaria Prevention Measures In all FGDs and KIIs conducted, participants and key informants knew that there were various ways of preventing malaria. Like clearing bushes around homes, keeping good environmental hygiene, disposing of empty tins and broken pots, draining away stagnant water, pouring oils on water ponds, digging deep pit latrines, closing windows and doors early in the evening, and eating a proper diet to make the body stronger. Despite having this knowledge, the malaria prevention practices in this community were reported to be poor (Table 1). For example, it was mentioned that most people do not close windows and doors early in the evening, they do not frequently clear bushes around their homes and they make no effort to remove broken pots and stagnant water. The reasons given by most of the participants (about seven out of 10) in the FGDs for not practicing preventive measures were laziness for environmental measures and economic constraints in the case of ITNs and mosquito repellents that have to be purchased. For example: “We do not put a lot of emphasis on what we are told to do due to laziness” (39-year-old non-pregnant woman Udo in Ezinihitte LGA). Among other reasons given by participants for poor practices regarding malaria prevention and treatment were ignorance, lack of awareness and the high cost of accessing services at health facilities. In all the FGDs, more than threequarters of participants said that they could not afford to buy ITNs or the cost of assessing services at health facilities. This was confirmed by all the key informants. But it was also noted by a few participants (about three out of 10) in three of the FGDs that some people simply do not bother to take care of their health: “Some people here do not give life a priority; people, especially men, prefer to use the money for drinking alcohol than buying mosquito nets” (32-year-old female respondent Itu in Ezinihitte LGA). It was noted that poor malaria prevention practices by some people have a negative influence on others. Three male participants at one FGD at Afor Enyiogugu market noted that they have neighbours who do not clear bushes or they plant maize gardens which are breeding places for mosquitoes. It was also thought that the government was supposed to protect the people from malaria by providing drugs in dispensaries and clean water, such as from boreholes which are not breeding places for mosquitoes. From the discussions in all FGDs, it was apparent that attendance of antenatal care in this area is poor, and this results in limited access to information on malaria prevention in pregnancy, such as the benefits of IPT and ITNs. In all the FGDs, participants said that the majority of women (approximately eight of every 10) go to health units at least once in order to get a maternity card. So if they have problems of the time of delivering, they can present the card as evidence that they attended antenatal care. It was further noted in most of the FGDs (eight out of 10) that many pregnant women (over half) deliver at home with help from traditional birth attendants (TBAs) while few deliver at health facilities (Table 2). Over three quarters of the participants in all FGDs (both male and female) gave the following reasons for pregnant women not delivering at health units: normally women deliver at home without problems, there is strong belief in the effectiveness of TBAs, and TBAs are accessible and understand women’s problems. The majority of key informants (over threequarters) noted that the poor quality of care at health units, the costs involved in seeking antenatal and delivery care, and ignorance of women were the main factors that prevent women from delivering at health facilities. The expression below summarizes the reason why women prefer delivering with the help of TBAs. “We prefer to deliver at home or with TBAs because they know how delivering a child pains, so they care for you: but in hospitals, they abuse you” (From the FGDs) Other reasons why pregnant women do not use antenatal care services at health units included: lack of money to cover transport and the cost of drugs; fearing that the health workers abuse them either because of their attire, their beliefs in using herbs or their going to seek care at health facilities when it is late; lack of knowledge on the importance of good health during pregnancy; and fear of injection pain. Some participants (about three 10) in four FGDs reported that they had all their deliveries at home with no problem, and therefore they did not see the need for attending antenatal care and delivering at health facilities. In the study area, all participants in the 10 FGDs and all the key informants were aware that it is more important to use preventive measure against malaria than wait to fall sick and be incapacitated by the disease or face the burden of seeking treatment. The main determinant factor for this choice was the perceived low cost incurred in practicing preventive measures. Table 3 shows the enabling and disabling factors in relation to use of preventive measures. The reasons given for not taking treatment as a first option include fear of expired drugs and inappropriate doses prescribed by drug vendors. Discussion The results of this study show that people in the study area are aware of the dangers of malaria and the various ways it can be prevented. They also know that malaria mostly affects pregnant women and children and that ITNs are beneficial in reducing the burden of malaria. However, there is low use of ITNs and other malaria preventive interventions in this area. This was partly attributed to the high cost of ITNs and negative perceptions on the chemicals used to treat them, especially among non-users, and to poor utilization of health services, particularly antenatal care and delivery care, leading to missed opportunities. Both pregnant and non-pregnant adolescents were perceived not to be at risk of malaria, and were found least to benefit from malaria prevention interventions due to the stigma surrounding adolescent pregnancy. Similarly men were perceived to be at less risk of malaria and were found uncaring in malaria prevention. Our findings further show that there is a perception that men do not care for the health of their spouses and do not prioritize health issues. This is an area in which further investigation is recommended. Some studies have documented perceptions regarding use of ITNs in malaria prevention. A study carried out in Western Uganda, found that mosquitoes were perceived as a cause of malaria but at the same time use of bed nets was low (26%). People who did not use bed nets cited discomfort due to heat and humidity; and the high cost of ITNs as reasons for non–use 26. In Kenya, community reactions were assessed before the introduction of permethrin-treated bednets. Although malaria was found to be an important disease, ITNs were believed to be only partially beneficial because of the perception that malaria had multiple causes and further to this, fear was expressed that the chemicals used to treat ITNs were associated with the use of family planning27 . After a randomized controlled trial of ITNs mothers in intervention villages were more knowledgeable on benefits of ITNs, resulting in good care of nets and re-treatment with insecticide 28 . The results of this study are not only consistent with the above findings but have highlighted that people perceive chemicals used in treating nets to be associated with poor pregnancy outcomes and to have an effect on children. In order to increase access to ITNs, this perception will have to be demystified through education on how the chemical used to treat nets works. Furthermore, negative perceptions on chemical mainly among non-users was also found. It would be of interest to find out about community discussion groups where users of malaria prevention interventions narrate their experiences and assess how this motivates the non-users. The findings of this study further show that the cost of ITNs and mosquito repellants is an important barrier for their use. This is also consistent with previous studies which have shown that the cost of ITN impregnation, regular re-impregnation and the availability of ITNs are determinant factors for use of ITNs in malaria prevention 13, 29. However a study in the Gambia found that use of ITNs was correlated with ethnic group, age and polygamy, but not with education, income, occupation or ownership of items which indicate high social status 19 . This highlights the importance for malaria prevention of other factors like perceptions and beliefs on ITNs. An important factor contributing to poor quality care at health facilities has been identified in this study. This is poor communication skills among nurses and individuals and the way they handle pregnant women who come to deliver at health facilities. It is possible that the low antenatal care attendance observed in this study is associated with the perceived poor quality of care at health facilities. One could argue that malaria preventive interventions currently delivered through health facilities are not accessible in the study area and therefore there is no motivation to use them. An important finding is that most people in this area trust information given to them by health workers. There is an important opportunity for health promotion programmes to use this channel by providing refresher courses to health workers to update both their knowledge and their skills in communication and counseling on prevention of malaria in pregnancy. Similarly this study has documented that a large proportion of women are attended to at delivery by traditional birth attendants (TBAs). This highlights an opportunity for identifying ways of involving TBAs and other community resource persons in increasing coverage of ITNs and other malaria prevention tools like intermittent preventive treatment (IPT). Results of the present study have indicated that people fear there are expired drugs in the market and that drug vendors will give them improper dosages, especially for treatment. Further the perceptions on expired drugs, drug resistance and how these perceptions influence the use of chloroquine for IPT among pregnant women. Knowledge on perceptions of malaria in adolescents is a neglected area, yet adolescent pregnancies are always found especially in the rural communities. This study has documented widespread perception that adolescents are not vulnerable to malaria. This might be partly explained by the stigma surrounding adolescent pregnancy. Similar findings were found in a part of Nigeria where premarital pregnancy was resented, associated with shame and most parents hid their daughters. Thus the adolescents were more likely to resort to self medication rather then using services at health facilities 30 . The implication of these findings include the need to increase awareness about the dangers of malaria among adolescent primigravidence by focusing attention on adolescents themselves, their peers, parents, health workers and community resource persons. Ways of reaching adolescents earlier need to be identified. Although most people in the study area knew ways of preventing malaria, the findings documented that this knowledge is not used in daily practice. The reason for this seems to be that people, including pregnant women, are not really concerned. Several explanations can be given for this behaviour. It is known that in highly endemic areas, people get used to sickness and with time, they adopt to the disease. It is therefore possible that malaria is not seen as life threatening and deaths due to malaria may not be attributed to malaria itself but to other causes. It is also possible that people get used to poverty, sickness and death due to malaria and other diseases that they no longer care about their fate. There is need for more research to investigate why people who perceive a disease as a common cause of ill health do not take adequate preventive measures. This study has shown that negative perceptions on ITNs are held by most people who have not used them and do not have first-hand experience. It would be interesting to try an intervention where users of ITNs narrate their experiences to non-users and test how this may influence the use of ITNs in the community. Similarly, it would be of interest to find out what questions people ask when they are purchasing ITNs. This will enable policy makers to design a better package for ITN distribution. Several factors that influence the use of ITNs and other malaria prevention interventions were identified in this study. These include the high perception on the seriousness of malaria and its effect on pregnant women and children, the high perceived benefit of ITNs in protecting children and pregnant women against malaria and the high awareness of the prevention of malaria as a better and cheaper option compared with treatment. Inhibitory factors include fear of the chemical that is used to treat nets, high cost of ITNs and the high cost of assessing health services, uncaring husbands, unavailability of ITNs in communities and low quality of health services. The implications of these findings include the need to develop a health promotion package based on these factors, especially demystifying the negative perceptions on the chemicals used in treating nets (ITNs) in order to increase access to this intervention. The perceived high costs of ITNs should provide lessons to programmes that aim at increasing access to ITNs for pregnant women in malaria endemic countries. Adolescents as a group need to be specially targeted. Health workers and parents need to be involved in the health-seeking behaviour of adolescents. There is also need to target men regarding health seeking behaviour of pregnant women, especially in use of ITNs and IPT. References
The following images related to this document are available:Photo images[rh10010t3.jpg] [rh10010t1.jpg] [rh10010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}