 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
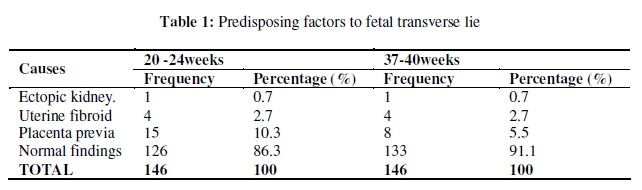
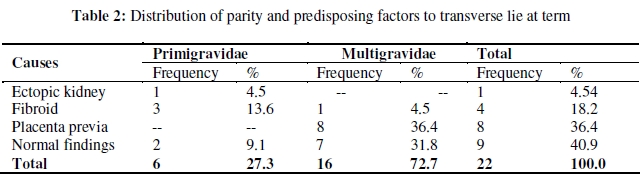
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 129-133 ORIGINAL RESEARCH ARTICLE Longitudinal Evaluation of Foetal Transverse Lie using Ultrasonography Evaluation ultrasonique de la presentation traversale au terme Olalekan I Oyinloye1* and Alexander A Okoyomo2 1Department of Radiology, University of Ilorin Teaching Hospital, Ilorin; 2Department of Obstetrics and Gynaecology, Federal Medical Centre, Lokoja, Nigeria. *For correspondence: Email: Oyinbuk2001@yahoo.com ABSTRACT The purpose of this study was to assess the risk of persistence of transverse lie detected earlier in pregnancy and associated predisposing factors using follow-up ultrasound (US). A longitudinal study was carried out from January 2004 to august 2004 at Federal Medical centre, Lokoja, Nigeria. All singleton pregnancies, with ultrasound diagnosis of transverse lie, between 24-28 weeks were followed to term. At 24-28 weeks, 183 fetuses presented with transverse lie. Thirty seven were lost to follow-up; out of the remaining 146 babies, 22 persisted to term. Overall persistence rate was 15.1%. No identifiable predisposing factors were seen in 91.1%, placenta previa in 5.5%, lower segment fibroids in 2.7%, and ectopic kidney in 0.7%. In conclusion, transverse lie detected early in pregnancy is transient, and majority would convert to a longitudinal lie at term. Potential predisposing factors highlighted above increases the risk of persistent transverse lie at term, with placenta previa and lower segment fibroids being the major predisposing factors (Afr J Reprod Health 2010; 14[1]:129-133). RĖSUMĖ Cette étude avait pour but d’évaluer le risque de la persistance de la présentation transversale détectée plus tôt pendant la grossesse et les facteurs prédisposants associés à l’aide de l’ultrason de contrôle. Une étude longitudinale a été menée entre janvier 2004 et août 2004 à Federal Medical Centre, Lokoja, Nigeria. Toutes les grossesses simples ayant un diagnostic ultrasonique d’une présentation transversale d’entre 24 et 28 semaines ont été suivies jusqu’au terme. A la fin de 24 – 28 semaines, 183 fœtus se sont présentes de manière transversale. Trente-sept ont été perdus de vue. Sur les 146 bébés, 22 ont survécu jusqu’au terme. Le taux de la persistance globale était de 15,1%. Nous n’avons pas noté des facteurs prédisposants identifiables chez 91,1%, le placenta chez 5,5%, les fibromes du segment inférieur chez 2,7% et le rein ectopique chez 0,7%. En conclusion, quand la présentation transversale est détectée tôt pendant la grossesse, elle est transitoire et la majorité seraient converties à une présentation au terme. Les facteurs prédisposants potentiels sur lesquels on a attiré l’attention ci-dessus, augmentent le risque de la présentation transversale persistante au terme, ayant comme facteurs predisposants majeurs le previa du placenta et les fibromes du segment inférieur (Afr J Reprod Health 2010; 14[1]:129-133). KEYWORDS: Persistent fetal transverse lie, Ultrasound scan diagnosis, Predisposing factors. Introduction Foetal transverse lie persisting to term has been associated with serious complications like uterine rupture and cord prolapse during labour, hence a cause of concern for pregnant women and their carers 1,2 . Therefore, when transverse lie is detected during routine ultrasonography, follow up of such pregnancy to term is necessary to determine persistence of such lie, and associated predisposing factors. This will enable the mode of delivery to be determined, and forestall complications to both the infant and mother. Ultrasonography has been established as a clearly superior means of determining noncephalic presentation during pregnancy than routine manual palpation3. Therefore, a definitive US based data, on the risk of persistent abnormal lie at term would provide a useful statistical tool in advising women on the chances of abnormal presentation, and prepare them for the potential requirement of caesarean section (CS) 4. The incidence of transverse lie, detected in early pregnancy persisting to term gestation has been reported to vary between 6 and 22%. As term approaches, the likelihood of persistence of transverse lie increases4,5. This study aims to provide an ultrasound based data on the risk of persistent transverse lie and associated predisposing factors in our environment, using follow-up ultrasound of transverse lie detected earlier in pregnancy. Materials and Methods This longitudinal study was carried out from august 2003 to august 2004 at Federal medical centre, Lokoja, Nigeria. The study was approved by the ethical committee of the hospital. All women with singleton pregnancies referred to the ultrasound unit of the hospital for routine ultrasonography, with foetal transverse lie discovered between 20-24 weeks of gestation were incorporated in the study. The foetus was said to be in transverse lie when its longitudinal axis is perpendicular to the maternal spine. Diagnosis of placenta previa was made on US when the placenta partially or completely covers the internal os. The foetuses were followed up and had repeat US at 30-34 weeks and a final US evaluation at 37-40 weeks of gestation. A siemens SL machine 3.5 MHz linear array probe machine was used. The pregnant women lay in the supine position and the entire abdomen scanned. The full-bladder technique was used to aid detection of placenta previa, or lower segment masses which could predispose to transverse lie. All other relevant data were also collected from patient case files, including maternal age, last menstrual period (LMP) and previous obstetric history. Data analysis to derive frequency and percentages were done using Statistical Package for Social Sciences (SPSS) version 11. Results A total of 183 patients were found to be in transverse lie at 20-24 weeks gestational age. Thirty seven patients were lost to follow-up and therefore excluded from the study. The remaining 146 patients, consisting of 125 multigravidae (85.6%) and 21 primigravidae (14.4%) were followed to term. The mean age of the pregnant women was 28.3 ± 5.8 in this study. The mean parity was 3.2 ± 1.7, with a mode of 4. At 30-34 weeks of gestation, a total of 103 (70.5%) foetuses had converted to longitudinal lie with 43 (29.5%) remaining in transverse lie. At 37-40 weeks, a total number of 124 foetuses had converted to longitudinal lie (84.9%), with 22 (15.1%) remaining in transverse lie. Causes of transverse lie seen on ultrasound are represented in Table 1. At 20-24 wks, no predisposing findings to transverse lie was seen in 126 patients (86.3%), while placenta previa was the most frequent predisposing factor observed in 15 patients (10.3%). At 37-40 weeks, no predisposing findings to transverse lie were observed in 133 (91.1%) patients, however, the frequency of placenta previa had reduced to 8 (5.5%) patients. Ectopic kidney, constituted 1 (0.7%) and uterine fibroid 4 (2.7%) at both 20 to 24 wks and 37-40 weeks. At 37-40 weeks of gestation, out of the 22 patients remaining in transverse lie, 8 (36.4%), all multigravidae, had placenta previa, 4 lower segment fibroids, out of which 3 were primigravidae and 1 multigravidae. Ectopic kidney was seein 1 patient a primigravidae. No prediposing findings were seen in 9 women, with 7 being multigravidae and 2 primigravidae (Table 2). Discussion Associated factors like placenta previa, lower uterine segment masses, multiparity, congenitial uterine anomalies and ectopic kidneys can potentially increase the risk of persistent transverse lie1,6,7. Since transverse lie is associated with serious complication like uterine rupture and cord prolapse from premature rupture of membrane, during labour8. A study in Korle-bu Ghana, proffered that early antenatal detection and follow-up of predisposing factors like placenta previa with the aid of US could substantially reduce aforementioned complications, and elective deliveries could be undertaken8. In this study out of 146 patients discovered at 20-24 weeks, 103 (70.5%) patients had converted to longitudinal lie at 30–34 weeks and 124 patients (84.9%) at 37–40 weeks, with 22 (15%) remaining in transverse lie. This finding is similar to what was observed in earlier studies, which showed significant decline in the incidence of abnormal lie detected in the early trimester towards term.4,5 Fried et al in a study in which foetuses discovered to be in transverse lie by ultrasonography at 20 weeks were followed up, found the overall persistent rate of transverse lie to be 6%5. Similarly, Alice et al discovered that an abnormal presentation detected in the early trimester caries an overall 22.2% chance of persisting to term 4. Various predisposing factors have been known to contribute to the incidence of persistent transverse lie at term. In this study, placenta previa was the commonest predisposing etiology to transverse lie persisting to term. Its frequency was found to decrease from a total number of 15 discovered at 20 – 24 weeks to about half (eight) at 37-40 weeks. This is believed to also account for a reduction in the incidence of persistent transverse lie at term. The incidence of placenta previa detected during early pregnancy has been found to decrease as term approaches, this as largely been attributed to upward migration of the placenta as the uterus increases with advancement of pregnancy. Adeyomoye et al in a study of the accuracy of diagnosis of placenta previa by ultrasound in Lagos, discovered that conversion of placenta previa to a normal location occurred in 71.5% of patients by 35-39wks9. Other simillar studies have reported a conversion rate of between 63-90% 10-12. However, despite conversion of about half of placenta previa diagnosed earlier in pregnancy, to a normal location at term, it was still the commonest predisposing finding to transverse lie at term, occurring in 8 out of the 22 patients(36.6%). Fried et al also found placenta previa to be the commonest predisposing factor occurring in 35.7% of cases of transverse lie persisting to term5. In the light of this, it is necessary to have a follow up US in the 3rd trimester close to delivery as possible since the lower uterine segment is not usually formed till the late third trimester. Uterine fibroid constituted 18.2% of the predisposing etiology to transverse lie at term. Uterine fibroid is the commonest benign tumour of the female, when the size is large can cause mal-position and obstructed labour14 . It is also important to note that all 4 patients with huge, lower uterine fibroids discovered at 20-24 weeks remained in persistent transverse lie till term in this study. Ectopic kidney as a predisposing factor to transverse lie was seen in 1 patient earlier in pregnancy (20-24weeks), and the lie also persisted to term. Ectopic kidney, though not a very common occurrence generally, is also known to be a possible cause of persistent transverse lie6. Majority of the patient had no predisposing factor to transverse lie seen on ultrasound through out the duration of the study. At 20-24 wks, 146 foetuses were in transverse lie and 126 (86.3%) of the women had no obvious predisposing factors to transverse lie. At 37-40wks 124 foetuses converted to longitudinal lie and 22 (15.1%) fetuses remained in transverse lie with no predisposing factor to seen in 133 (91.1%) women. The reason for this increase is again attributable to the above mentioned statement, indicating that some of the cases diagnosed as placenta previa by 20-24weeks had apparently migrated to a more fundal location by 37-40weeks, hence falling under the categories of those with no obvious predisposing factors seen on ultrasound. Majority of patients at term with persistent transverse lie were mainly multiparae 16 (72.7%) while 6(27.3%)) were primigravidae. This observation is not surprising as the commonest predisposing factor to transverse lie has been attributed to a lax abdomen from multiparity, it is suggested that the pendulous abdomen from mutiparity allows the uterus to fall forwards deflecting the long axis of the foetus from the axis of the birth canal into a transverse lie6. Conversely when persistent transverse lie occurs at term in primigravidae, there is usually an underlying predisposing factor, which may be apparent or not. In this study, out of the 6 primigravidae with persistent transverse lie till term, majority, 4(66.6%), had predisposing factors demonstrable on US as the possible etiology of transverse lie. In the absence of any obvious predisposing factors to transverse lie in primigravidae seen at ultrasonography, and in whom the cause cannot be explained by a lax abdomen, causes not apparent during antenatal assessement like cephalopelvic disporpotion and congenitial uterine abnormally should be considered7. Hence it is suggested that delivery in primigravidae with persistent transverse lie should be by CS, even in the absence of obvious predisposing factors, while in the multigravidae external cephalic version (ECV) could be considered as an alternative to CS7. Conclusion The overall risk of persistent transverse lie, detected in this study was 15%, indicating transverse lie detected earlier during pregnancy to be transient in majority of cases. Placenta previa is the commonest predisposing etiology to transverse lie in this study, however, the incidence also reduced towards term, presumably due to upward migration of the placenta to a fundal position with advancement in pregnancy. The transverse lie detected earlier in pregnancy, with associated lower segment masses like uterine fibroid, almost have a 100% chance of persisting to term. In primigravidae with transverse lie at term, there is a high probability of an underlying predisposing factor, hence mode of delivery should be by CS and alternative means like ECV should not be encouraged. These above observations would likely provide a useful tool in advising women and their carers on the chances of persistent transverse lie at term in our environment, and preparing them for the potential requirement of CS. References
The following images related to this document are available:Photo images[rh10011t1.jpg] [rh10011t2.jpg] |
| |||||||||

{kind=link}
{kind=link}