 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
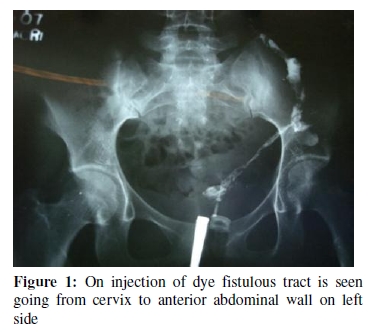
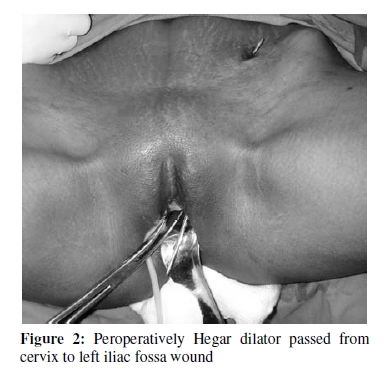
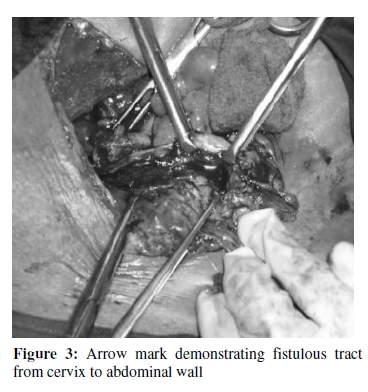
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 135-137 CASE REPORT An Unusual Case of Cervico-cutaneous Fistula Un cas etrange de la fistule cervicocutanee Seetesh Ghose, Dilip K Maurya, Mamatha Gowda and Parveen Begum Department of Obstetrics and Gynecology, Mahatma Gandhi Medical College and Research Institute, Pilliarkuppam, Pondicherry-607402, India For correspondence: Email: sonasee16@yahoo.co.uk Tel: 914132274633 Mobile: 919443244630 Office: 914132615449, ext no 124 Fax: 914132615457 ABSTRACT A lady presented with 6 months of amenorrhea and cyclical menstruation through an opening in the abdominal wall for the same duration, following septic abortion. Examination and investigations revealed an extraperitoneal Cervicocutaneous fistula, which was excised in toto. She had an uneventful recovery and resumed normal periods (Afr J Reprod Health 2010; 14[1]:135-137). RĖSUMĖ Une dame a présenté une aménorrhée qui a duré six mois et d’une menstruation cyclique à travers une ouverture dans le paroi abdominale pour la même durée, suite à un avortement septique. L’examen et les études ont révélé une fistule cervicocutanée extrapéritonéale qui a été excisée totalement. Sa récupération fut sans incidents et elle a repris ses règles normales (Afr J Reprod Health 2010; 14[1]:135-137). KEYWORDS: Cervicocutaneous fistula, Uterocutaneous fistula, Genital fistula Introduction Fistula is an abnormal communication between two epithelial surfaces. Vesicovaginal and rectovaginal fistulae are common genital fistulas well known in gynecology whereas uterocutaneous fistulae are very rare. Fistulae involving the uterus are usually result of abortions, postpartum and postoperative complications. We report in this paper the first case to our knowledge of extra peritoneal cervicocutaneous fistula which developed following a septic abortion. Case report A 25 year old lady presented with complains of cyclical monthly bleeding through an opening in the left lower quadrant of abdominal wall for past six months. She had no bleeding per vaginally for the same duration. There was a significant past history of incision and drainage for an abscess in the left iliac fossa 6 months back in a clinic (Jan 2009). General examination was unremarkable. Abdomen was soft with no palpable mass. In the region of left iliac fossa there was 1 cm sinus surrounded by exuberant granulation tissue. Per vaginal examination revealed a healthy cervix and induration in left fornix. Uterus was acutely retroverted and was normal in size. When methylene blue dye was injected into the cervix, there was free flow of dye through the abdominal wound. When contrast medium was injected into the cervix, there was no filling of uterine cavity. The dye was seen flowing from the cervix to the abdominal wall sinus (Figure 1). Sounding of uterus was attempted but failed due to stenosis. Based on above findings a provisional diagnosis of Cervico-cutaneous fistula was made. A work up for tuberculosis including mantoux test and chest X-ray were done and found to be negative. An exploratory laparotomy for excision of fistulous tract was done. Peroperatively a Hegar dilator was passed from cervix to the abdominal wound to delineate the tract during dissection (Figure 2). Abdomen was opened by suprapubic muscle splitting transverse incision. There were no adhesions intraperitoneally. Uterus was acutely retroverted with smooth surface and was of normal size. The fistulous tract in its entirety was extraperitoneal. When the Uterovesical fold of peritoneum was opened, three small bony spicules about 1cm each were found. The fistulous tract was found to be communicating to left lateral aspect of cervix, about 1 cm below the internal os (Figure 3). The tract was excised completely. As the internal os was completely closed the anterior surface of uterus was cut open and the cervical os was dilated from above under direct vision. A drainage tube was kept in uterus and was brought to vagina via isthmus and cervix. Uterus was closed in layers. An extraperitoneal drain was left in situ. Post operative period was uneventful. The vaginal drain was removed on postoperative day 7. Histopathology of fistulous tract was that of granulation tissue with nonspecific chronic inflammation. The three tiny spicules were confirmed to be bone on histopathology. Patient was put on high dose oral contraceptive pills to suppress menstruation for 4 weeks. On follow up abdominal wound scar was healthy. Patient resumed menstruation vaginally after stopping oral contraceptive pills and is having regular periods per vaginally since then. Discussion A number of cases of uterocutaneous fistulae are reported in the literature. Majority of these fistulae followed classical cesarean section. The decrease in the incidence of uterocutaneous fistula may reasonably be attributed to marked decrease in the frequency of that type of operation in modern obstetrics1 . Most uterocutaneous fistulae originate from some type of infective process that disrupts the continuity of tissues involved. Jain et al 2 reported an uterocutaneous fistula following lower segment cesarean section. Gupta et al 3 reported an uterocutaneous fistula which developed following septic abortion induced by laminaria tent insertion in the cervix. Dragoumis et al4 described a case of endometriotic uterocutaneous fistula after cesarean section. Uterocutaneous fistula is a rare condition that may be difficult to manage 5 . Surgical excision of the fistulous tract is the treatment of choice. Most cases end up with hysterectomy however Seyhan et al6 reported a case of uterocutaneous fistula that was successfully treated with gonadotropin-releasing hormone agonist administration. Here we are reporting the first case of cervicocutaneous fistula. In our case perforation was on the cervix probably due to acute retroversion of uterus. As perforation was below uterovesical fold of peritoneum, pus collection was totally extraperitoneal and pus tracked extraperitonealy to point in left iliac fossa. Drainage of pus abdominally resulted in fistula formation. Once a fistula is diagnosed, prompt excision of the fistulous tract in its entirety is required. Providing good drainage of uterus is important if recurrence is to be avoided. References
The following images related to this document are available:Photo images[rh10012f1.jpg] [rh10012f3.jpg] [rh10012f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}