 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
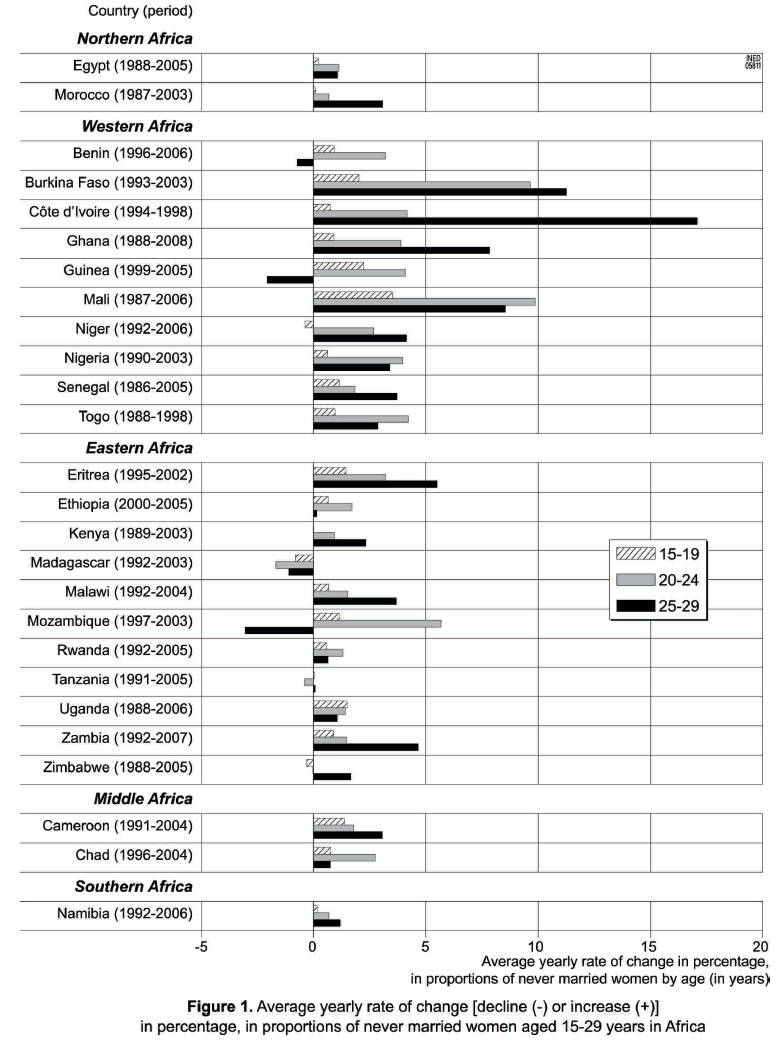
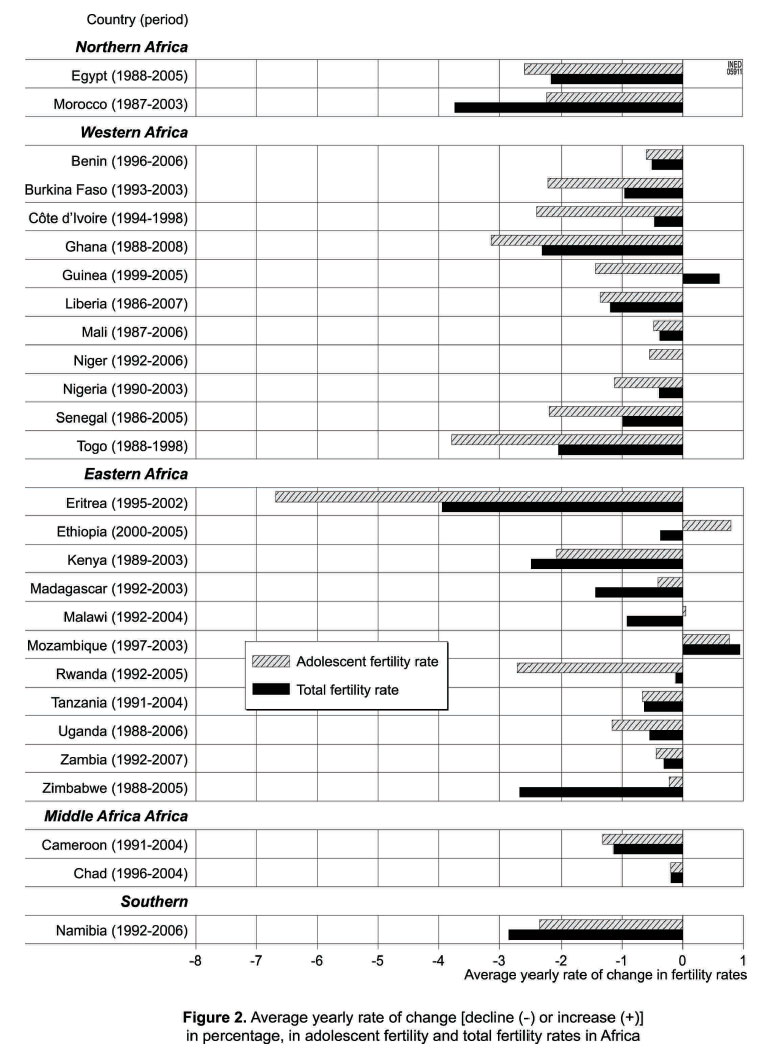
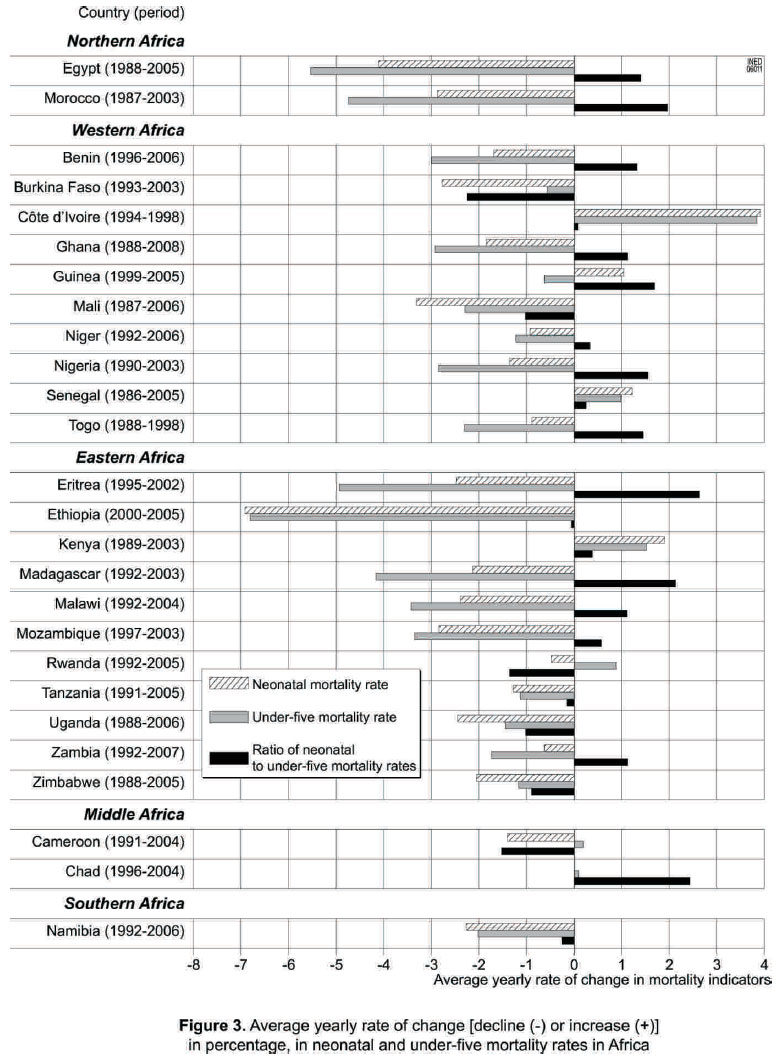
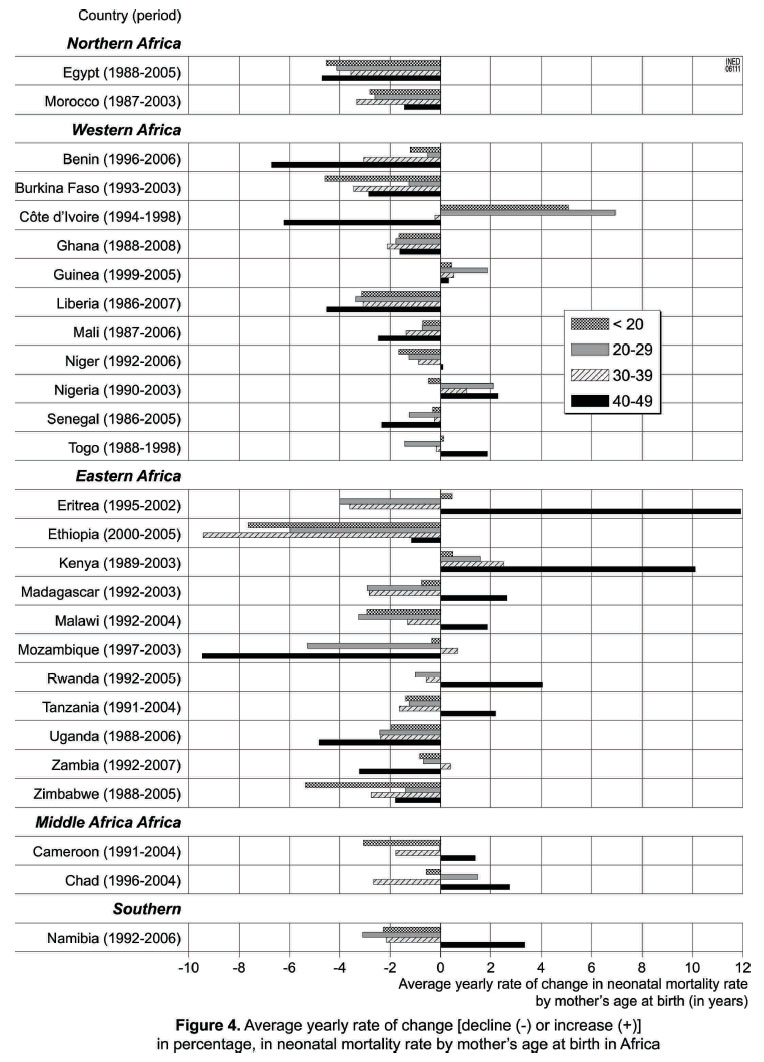
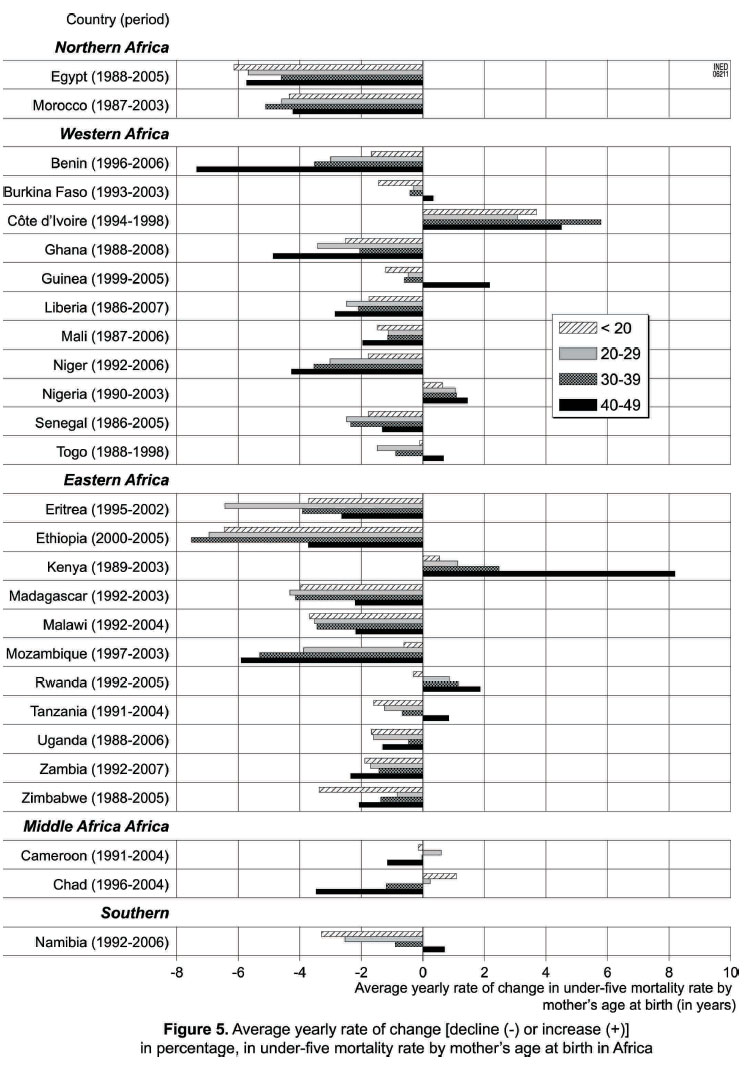
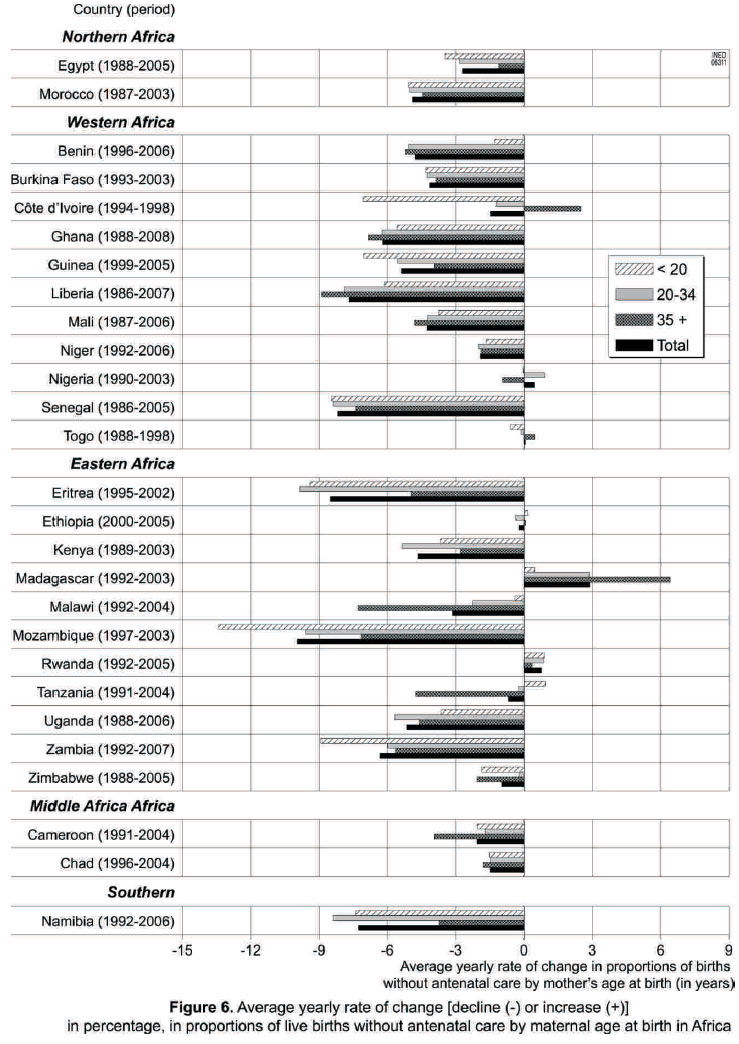
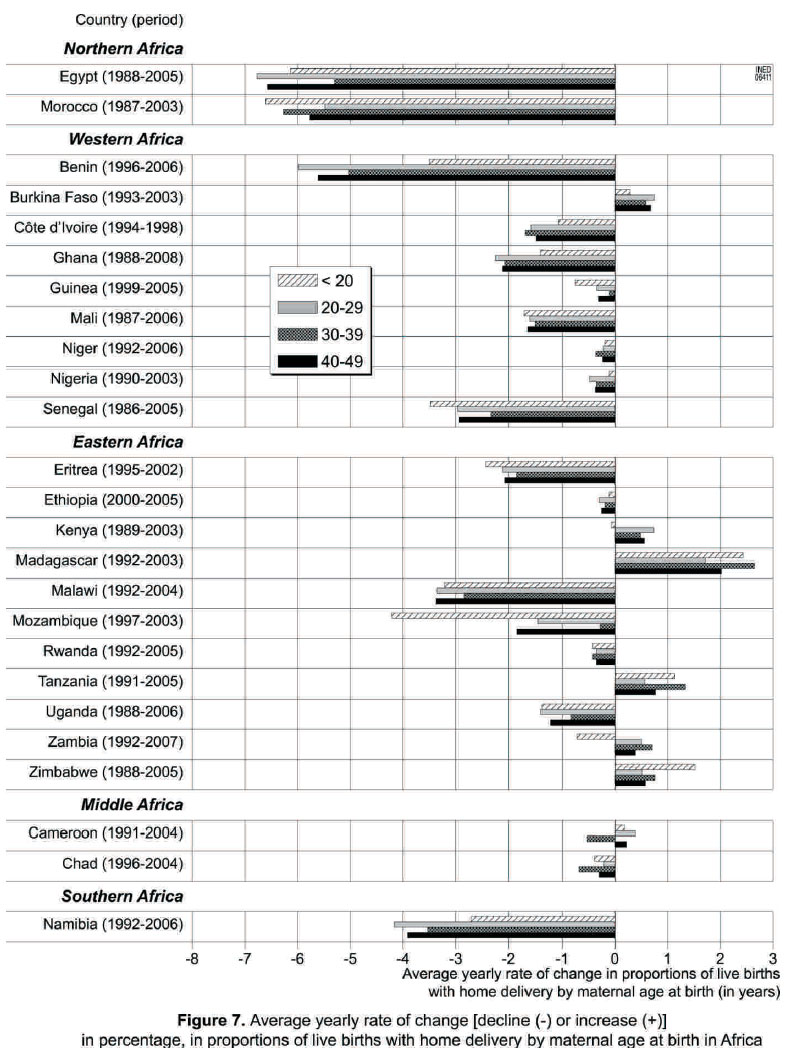
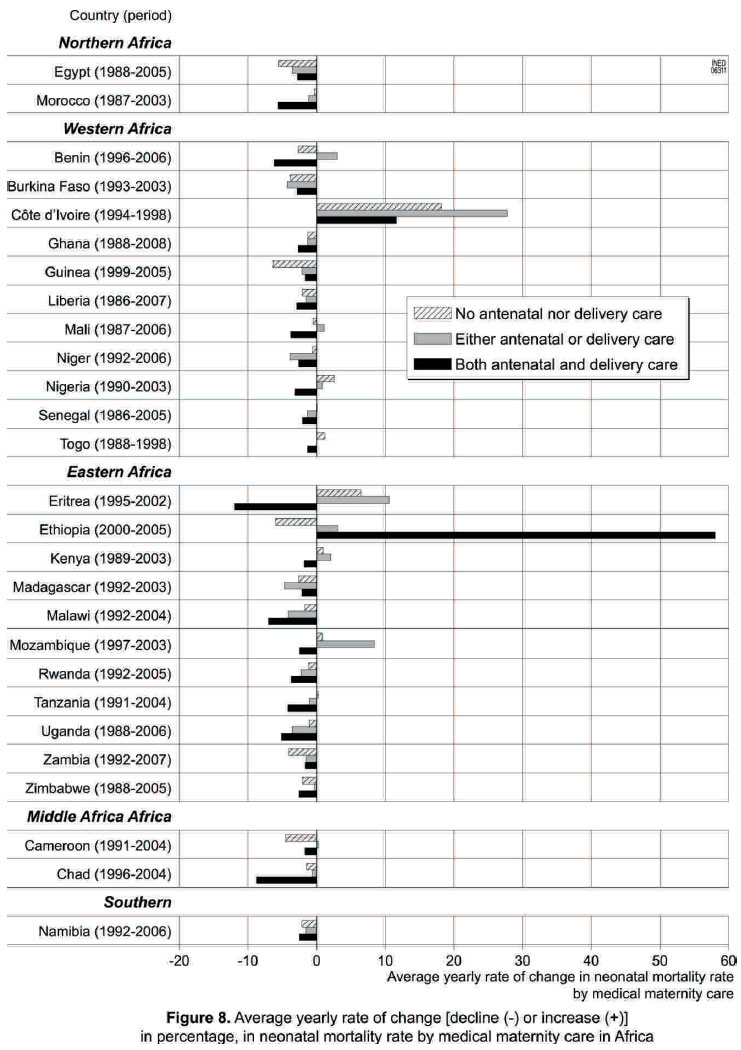
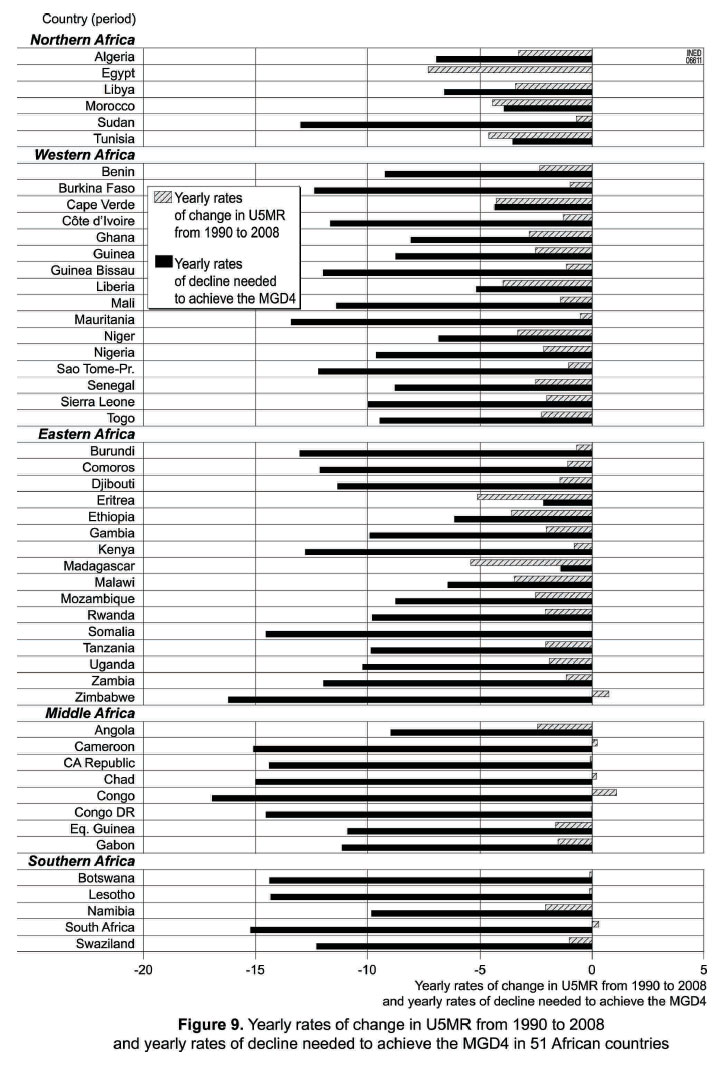
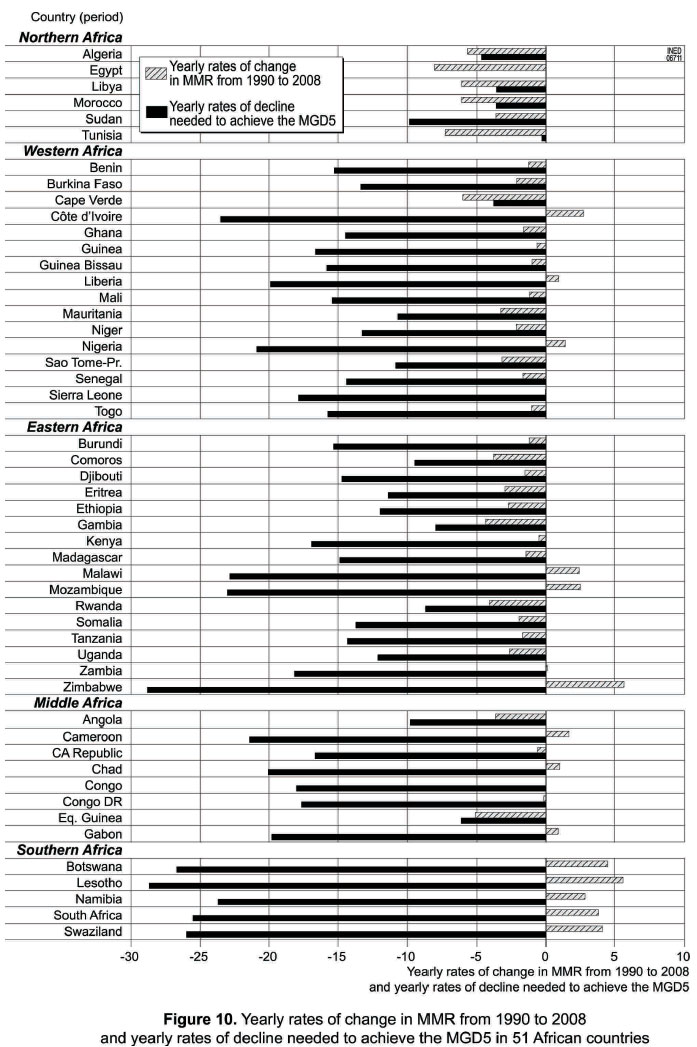
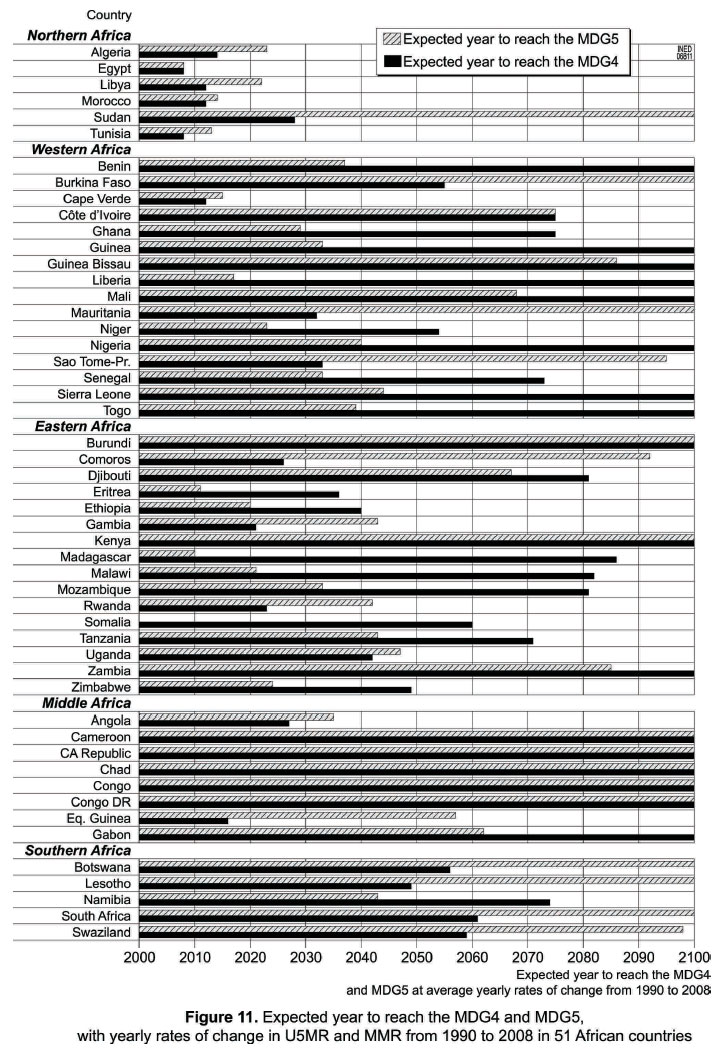
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 9-30 REVIEW ARTICLE The Importance for the MDG4 and MDG5 of Addressing Reproductive Health Issues During the Second Decade of Life: Review and Analysis from Times Series Data of 51 African Countries Barthelemy Kuate Defo Tenure Full Professor of Population Health & Global Health, CHUM Research Center & PRONUSTIC Research Laboratory, University of Montreal, Canada, Member of the United States' National Academy of Sciences' CPOP (since 2005), Chairman of the US National Academy of Sciences' Committee on “The Continuing Epidemiological Transition in Sub-Saharan Africa” Code Number: rh11017 Abstract Addressing adolescent sexual and reproductive health issues are central to efforts for reducing childhood and maternal mortality embedded in MDG4 and MDG5. This paper reviews these issues in Africa and uses statistical methods for measuring changes to analyze recent and comparable time series data from 51 African countries. The contribution of adolescent fertility to total fertility and mortality remains quite high. Delayed marriage is occurring concomitantly with postponement of sexual debut among unmarried adolescents. Six African countries are likely to achieve the MGD4 and five are likely to reach the target for the MDG5; the majority of sub-Saharan African countries will fall short of achieving these goals, not even by 2100 for many at current rates of change in progress indicators. Implementing ground-breaking nationally owned mortality-reduction schemes covering preconceptional and interconceptional periods and well-functioning comprehensive health-care system secured by sustained commitments and financial investments in health and social services are urgently needed, in order to repeal trends of further undoing successes achieved so far or slowing recent progress, thus hastening the pace of child and maternal mortality decline. Résumé S'occuper des questions de santé sexuelle et de la reproduction est au centre des efforts envers la réduction de la mortalité infantile et maternelle gravée dans les OMD-4 et OMD-5. Cette communication passe en revue les problèmes en Afrique et fait une analyse les données des séries du temps comparables tirées de 51 pays africains, à l'aide des méthodes statistiques pour mesurer les modifications. La contribution de la fertilité adolescente à la fertilité et à la mortalité totales demeure élevée. Ils se produisent des mariages retardés de manière concomitante avec la remise à plus tard de début des activités sexuelles chez les adolescents nonmariés. Six pays africains ont la possibilité d'accomplir l'OMD-5 ; selon les indices actuels de modification en progrès, la majorité des pays d'Afrique subsaharienne n'atteindront pas ces objectifs même en l'an 2100 pour beaucoup d'entre eux. Il faut assurer la mise en œuvre des programmes révolutionnaires visant la réduction de la mortalité sur le plan national qui appartiennent à la nation entière ; ceci doit aussi couvrir des périodes de préconception et d'inter conception ; il faut également mettre en place un système de soin sanitaire compréhensif qui fonctionne bien et qui est assuré par les engagements soutenus et les investissement financiers dans les services sanitaires et sociaux pour arrêter les tendances qui ralentissent le progrès récent, accélérant ainsi le rythme du déclin de la mortalité infantile et maternelle. Key words: MDG4, MDG5, Maternal mortality, child mortality, adolescent reproductive health, Africa I. Introduction Most child deaths are preventable or due to treatable conditions,1-3 and maternal deaths are largely avoidable.3-4 The Millennium Declaration in 2000 involved eight Millennium Development Goals (MDGs), two of which are the focus of this study: between 1990 and 2015, reducing by two thirds the under-five mortality rate (MDG4) and reducing by three quarters the maternal mortality ratio (MDG5). The highest rates of under-five mortality are found in Africa, and their reduction by 22 per cent since 1990 appears insufficient to meet the target.3 Most of the under-five deaths could have been avoided through prevention and treatment measures against the four diseases (pneumonia, diarrhea, malaria and AIDS) which accounted for 43 per cent of all deaths in children under five worldwide in 2008, including antibiotics for acute respiratory infections, oral rehydration for diarrhea, immunization, the use of insecticide-treated mosquito nets and appropriate drugs for malaria,1,3 and possibly the virtual elimination of mother-to-child transmission of HIV.5 In fact, the reduction in mortality in Africa from 1950 to 1980 is by most accounts one of the most farreaching changes achieved in the world since the onset of the industrial revolution.2 In developed countries, rates of maternal mortality from infection, pre-eclampsia, cardiovascular disease, intracranial hemorrhage and embolism have fallen to low and stables rates. In contrast, the leading causes of maternal mortality in developing regions and Africa are hemorrhage and hypertension, which together account for half of all deaths in expectant or new mothers; indirect causes such as malaria, HIV/AIDS and heart disease result in 18 per cent of maternal deaths while other direct causes such as obstructed labor, complications of anesthesia or caesarean section and ectopic pregnancy lead to 11 per cent of all deaths during pregnancy or childbirth.3 A recent study estimates about 342 900 maternal deaths worldwide in 2008 with over 50% of them clustered in six developing countries (India, Nigeria, Pakistan, Afghanistan, Ethiopia and the Democratic Republic of Congo).6 In words, maternal mortality represents the greatest divide between the developed and developing world, with an average lifetime risk of maternal death of 1/300. One of the great challenges of global health is the unacceptably high levels of maternal mortality in Africa.4,6 By 2006, it was shown that the timing of maternal deaths is clustered around labour, delivery, and the immediate post-partum period7 and it was argued in some quarters that a health-centre intrapartum care and maternal care strategy would be most likely to bring down rates of maternal mortality.8 That argument around a purely health-systems strengthening approach to reducing maternal mortality was challenged as too rigid or beyond the abilities and environments of many developing countries;9 A study in Senegal substantiates this view.10 By 2007, a re-conceptualization of maternal mortality took place with the notion of a continuum of care, integrating strategies, resources, interventions, and outcomes for maternal, newborn, child, and reproductive health.11 The addition of a new target (5.B) to have universal access to reproductive health --as defined at the ICPD in 1994 -- has given renewed priority to addressing care related to the health outcomes of MDG5 and to redressing the large disparities in coverage of health services between and within countries through necessary interventions in maternal health. The Countdown to 2015 process12 promised higher attention to adolescent reproductive health only in later reports; we argue that the urgency is past due. This research is concerned with the interconnections between sexual and reproductive health issues in adolescence and maternal health, and the health of newborns and children and of the mothers that the girlchildren may become. It highlights the importance of addressing these issues in any preventive, promotionlike, educative, curative, or rehabilitative action that improves maternal and child health. We assess regional and between-country variations in patterns and levels of sexual and reproductive health outcomes, disentangling issues for MDG4 and MDG5 that are sometimes hidden in studies using a single cross-sectional survey and may become apparent in time series data utilized for 51 African countries. II. Epidemiology of sexual and reproductive health with relevance to maternal and child survival Sexual and reproductive health is a prerequisite of MDGs related to gender and health. The most direct link is with MDG5, but progress towards MDG4 and MDG5 is inextricably linked: improving maternal health will lead directly to reductions in deaths among newborns and young children. Sexual and reproductive ill health accounts for an estimated onethird of the global burden of disease and early death in women of reproductive age. Every year, there is an estimated 180–210 million pregnancies, 80 million unwanted pregnancies, 50 million induced abortions, 20 million unsafe abortions, 536 000 maternal deaths including 68 000 deaths from unsafe abortion, 20 million postpartum infections and disabilities and 340 million people infected by sexually transmitted infections (STI). 13 Estimated annual AIDS-related deaths worldwide remain too high, despite their decreases from 2.1 million in 2004 to 1.8 million in 2009.5 The achievement of the MDGs related to health is strongly underpinned by the progress that can be made on sexual and reproductive health.3-5, 14-18 First, apart from ill-health consequences, poor sexual and reproductive health contributes significantly to poverty, inhibiting affected individuals' full participation in socio-economic development. 3,13 Second, ill-health from causes related to sexuality and reproduction remains a major cause of preventable death, disability and suffering among women in Africa.3-4 Third, contraceptive use remains lower and pregnancy risk remains higher for adolescent women than older women.4-5,15-18 Fourth, healthy pregnancy, childbirth, motherhood and life transitions for childbearing women are strongly influenced by care and opportunity structures (e.g., education, health, transportation, technology).4,16-18 Fifth, girls and mothers are the most vulnerable and disadvantaged in most environments in sub-Saharan Africa.4,16-19 Sixth, basic and reproductive prenatal and postnatal healthcare during the pre-reproductive and reproductive years of women can reduce maternal and early childhood morbidity, disability, and mortality.3,17 Seventh, successful programs and interventions have targeted key entry points during a women's entire life cycle and her offspring. For the mother, these entry points are: pre-adolescence, adolescence, before, during, and after pregnancy;4,16-19 for the child, interventions activities are to be carried out from conception to birth and during childhood years.1,4,14-18 The stumbling block of most of these interventions has been their sustainability for those proven successful. Usually, they are undertaken with massive funding from external sources for short durations of demonstration projects. Reduction of maternal and childhood morbidity and mortality from pregnant adolescents will contribute significantly toward achieving MDG4 and MDG5. Between 14 and 15 million women aged 15-19 give birth each year, which accounts for more than 10% of births worldwide with childbirth from adolescent mothers accounting for 15% of the global burden of disease for maternal conditions and 13% of all maternal deaths, while under-15 years old girls and their offspring face highest risks of maternal and neonatal deaths (e.g., for every young woman who dies in childbirth, 30-50 others are left with an injury, infection or disease).15 Worldwide, adolescent reproductive health is a key development and public health. Addressing it often requires overcoming sensitivities and resistance. The HIV pandemic, disproportionately affecting young women, makes this task even more urgent. In sub-Saharan Africa, more women than men are living with HIV and young women aged 15–24 years are as much as eight times more likely than men to be HIV positive.5 The highest prevalence and incidence of (and overlap between) many health problems occur during adolescence in Africa.19 Although the global burden of disease does not estimate the burden of disease for 10-24 years old as a separate group, it is during the second decade of life (10-19 years) that most of a person's long-term health-related behaviors (e.g., smoking, diet, exercise, use/abuse of drugs or alcohol or other substances, sexual practices, attitudes and preferences related to reproductive behavior including fertility and contraception, and health and disease) are formed, as well as coping strategies for dealing with such situations as stress, pain, aggression or disappointment. Diseases and unhealthy behaviors which are important problems in young people have been classified into five broad categories:19 those which are specific to young people (e.g., disorders of secondary sexual/social development, suboptimal adolescent growth spurt, and sexual assault/abuse); those which affect young people disproportionately (e.g., maternal disorders, alcohol and other substances abuse, tuberculosis, STI/HIV/AIDS, schistosomiasis, maternal mortality and morbidity, accidents, intestinal helminthes); those which manifest themselves primarily in young people but originate in childhood (e.g., rheumatic heart disease, polio, and chagas disease); those whose major health implications are on the young person's future health (e.g., smoking, diet, exercise, STI including HIV/AIDS, dental health, and leprosy); and those problems which affect young people less than children but more than older adults (e.g., stunting, anemia, and cerebral malaria). Successful interventions should aim not only at making the behavior of young women healthier but at improving health systems so that more young women, especially those living in rural areas or in impoverished households, can have access to welltrained and well-supplied primary health care services and referral networks. III. Data sources and statistical analysis We use comparable data from 95 Demographic and Health Surveys (DHSs) fielded from 1988 to 2008 in 40 African countries, as well as MDG4 and MDG5 mortality indicators for 51 African countries from two independent sources.6,20 Analysis of mortality requires that deaths are measured on a representative population for which conditioning exogenous characteristics are known. While recollections from women concerning the births and survival status of their children retrieved from the DHSs provide reasonably reliable basis for direct estimates of mortality and fertility (and are used in this study), no similar scheme has proved fully satisfactory for maternal mortality; hence, we use the latest peerreviewed estimates published.6 Several approaches have been developed for forecasts of population health and mortality using stochastic models and textbooks written on systematic account of linear time series models and their application to the modeling and prediction of data collected sequentially in time.21 Several existing unconditional methods for setting confidence intervals for the difference between binomial proportions have shown that interval estimation for proportions and their differences encounters two problems: intervals that do not make sense and a coverage probability (or achieved confidence level) that can be quite differentto the intended nominal 1-a.22-23 Unfortunately, standard statistical software has nothing to offer the user. Hence, by default, the computationally simplest asymptotic methods continue to be used, despite their known poor coverage characteristics and propensity to aberrations.23 For these reasons, we use a simple statistical approach for assessing changes over time in reproductive health-related progress indicators of MDG4 and MDG5. We consider a constant rate of change for a given inter-survey interval and compute an average yearly rate of change in proportions and rates. We have not built into our forecast any degree of acceleration or deceleration of change, and have assumed a uniform distribution of change in progress indicators of MDG4 and MDG5 over time under two scenarios: one for the targeted level of under-five mortality rate (U5MR) and maternal mortality ratio (MMR) expected by 2015; another for the expected year for reaching the targeted U5MR and MMR by 2015 at the current average yearly rate of change between 1990 and 2008. IV. Results To save space, findings are graphed; tables from which they are derived are available upon request. 1. Delayed marriage and sexual debut during the second decade of life and beyond Initiation of sexual activity is a normal component of human development and it often occurs during adolescence and beyond, with profound implications for sexual and reproductive health including unsafe abortion which is a major cause of maternal mortality among teenage women in Africa.4,16,18,24 We examine age-specific rates of celibacy among women aged 15-49 years and illustrate the emerging patterns in Figure 1. At the exception of Egypt, Mali, Nigeria, Senegal, Kenya, Tanzania and Zimbabwe, the rates of celibacy during adolescence have consistently risen in African countries. These rates have also risen among the 20-24 years old for all countries but Mali, Niger, Madagascar, Malawi, Tanzania, Zimbabwe and Cameroon. Early marriage remains important in Niger and Mali. Average yearly rates of increase (AYRI) in celibacy rates among adolescents raised most in Western Africa (3.51% in Mali, 2.23% in Guinea and 2.03% in Burkina Faso), followed by Eastern Africa (1.51% in Uganda, 1.45% in Eritrea and 1.16% in Mozambique) and Central Africa (1.39% in Cameroon). Trends towards postponement of marriage are reinforced in the 20-24 and 25-29 years age groups as well for most countries: AYRI in age-specific celibacy rates are highest in West Africa. Countries in East Africa witness substantial increases in AYRI in celibacy rates. Madagascar is the sole country with declining proportions for the 15-29 years old women. We also assess the history of sexual activity among never married women in all African countries with available data, and document average yearly rates of change in proportions of never married women by history of sexual activity and median ages at first sex among women aged 15-29 years. Early marriage put girls at elevated risk of reproductive health problems including HIV infection and AIDS-related deaths.5,16,18 Three patterns surface (table not shown, available upon request): rates of sexual abstinence have consistently increased or have remained unchanged or have declined in African countries. First, the rates of postponement of adolescent sexual activity have consistently risen in 15 sub-Saharan African countries: Benin, Burkina Faso, Côte d'Ivoire, Mali, Senegal and Togo (Western Africa); Eritrea, Ethiopia, Kenya, Malawi, Rwanda, Uganda and Zambia (Eastern Africa); and Cameroon and Chad (Middle Africa). Rates of sexual abstinence have also increased among unmarried women aged 20-24 years in Burkina Faso, Ghana, Mali, Niger, Senegal, Eritrea, Kenya, Uganda and Cameroon. Second, the rates of sexual abstinence are stable among women aged 15-19 years in Guinea, Mozambique and Zimbabwe. Third, the rates of sexual abstinence have been fluctuating or declining in Niger, Nigeria, Ghana, Madagascar, Tanzania and Namibia. Early marriage can lead to greater risks of STI through unprotected sex with partners who have higher rates of STI and pregnancies that put young women at risk for obstetric fistulae and can be a risk factor for HIV infection. Changes in early marriage and sexual debut have translated into variations in median age at first sex among women aged 15-24 years old. Increases in the median age at first sex are found in Burkina Faso, Côte d'Ivoire, Ghana, Mali, Senegal, Togo, Eritrea, Ethiopia, Kenya, Malawi, Mozambique, Uganda and Cameroon. Changes in median ages at first sex have been fluctuating in Benin and Madagascar or small in Nigeria, Rwanda, Zambia, Zimbabwe, Tanzania and Namibia. Data from all African countries (but Madagascar, Niger, Zimbabwe and Kenya) show a positive association between rates of marriage and sexual activity and age. Overall, robust postponements in marriage concurrently with adjournment of sexual debut during adolescence and beyond are found in most countries. 2. Changes over time in fertility rates and contribution of adolescent fertility to total fertility There is a vast literature showing that adolescent pregnancy and childbearing are closely linked to maternal, newborn and childhood health outcomes. Adolescent mothers are more likely to suffer severe complications during delivery due to physiological immaturity which results in higher morbidity and mortality for themselves and their offspring. Adolescent pregnancies may also encourage illegal abortion which is usually performed under unsafe conditions leading to elevated risks of reproductive health problems including pelvic infection and death. Figure 2 highlights the main changes in the fertility rate for women aged 15-19 (or adolescent fertility rate -- AFR) and the total fertility rate (TFR) within and between countries, from 1988 to 2008. We also examine the proportion of total fertility contributed by adolescent fertility (PFAF). TFRs are highest in Africa. Three trends emerge. First, countries with declining rates of fertility along with a reduction or stagnation in the PFAF comprise: Northern African countries, Burkina Faso, Côte D'Ivoire, Ghana, Guinea, Liberia, Mali, Senegal, Togo, Eritrea, Madagascar, Malawi, Uganda, Zimbabwe, Chad and Namibia. Second, countries with stagnation or reversals in their fertility decline are: Benin, Niger, Nigeria, Kenya, Mozambique, Cameroon and Rwanda. Third, countries with divergent or fluctuating trends in fertility along with increasing or stagnating PFAF over time include: Ethiopia, Tanzania and Zambia. In Western Africa, estimates of the PFAF are under 10% only in Ghana, Mauritania and Togo. In Eastern Africa, estimates of the PFAF are less than 10% only in Rwanda, Burundi, Comoros and Eritrea. Middle and Southern African countries have their PFAF at 10% or higher. Countries with reversals in fertility decline also have the highest PFAF (>10%), notably Mozambique (16%) and Cameroon (14%). Two countries stand out with increasing average yearly rates of TFR: 0.94% in Mozambique (Eastern Africa) and 0.60% in Guinea (Western Africa). Three African countries all from Eastern Africa have increasing yearly rates of change in AFR (0.79% in Ethiopia, 0.76% in Mozambique and 0.05% in Malawi). Eritrea is the sole African country with the innermost decline in average yearly rates of change over time in both AFR and TFR (6.69% and 3.95% for AFR and TFR, respectively). Asides from Northern Africa with average yearly rates of decline over 2% per year for AFR and TFR, average yearly rates of decline in AFR are generally deeper in Western Africa than in Eastern Africa (but Eritrea) or Southern Africa. 3. Changes over time in under-five mortality rates and contribution of neonatal mortality Levels of mortality remain uniformly high in Africa. Seven of the 40 countries analyzed have reversals in U5MR across age categories: Côte d'Ivoire, Nigeria and Togo (Western Africa), Kenya (Eastern Africa), Cameroon and Chad (Middle Africa) and Namibia (Southern Africa). The 19 countries with improved child survival are: Egypt and Morocco (Northern Africa), Benin, Burkina Faso, Ghana, Liberia, Mali, Mauritania, Niger (Western Africa), and Eritrea, Ethiopia, Madagascar, Malawi, Mozambique, Rwanda, Tanzania (Eastern Africa). Remaining countries have inconsistent trends (i.e., Guinea, Senegal) or no time series data. Declines in neonatal and under-five mortality are evident in 18 countries: Egypt, Morocco, Benin, Burkina Faso, Ghana, Guinea, Liberia, Mali, Niger, Senegal, Togo, Eritrea, Ethiopia, Madagascar, Malawi, Mozambique, Rwanda and Zambia. Côte d'Ivoire, Nigeria, Kenya and Cameroon experienced consistent increases in both neonatal and under-five mortality. The case of Kenya is alarming because rates of neonatal mortality rose by 23% between 1989 and 2003 and U5MRs increased by 24% over the same period. Figure 3 also shows that the contribution of neonatal mortality to under-five mortality has been substantial, varying between regions and countries. For the African continent as a whole, the lowest proportion of U5MR contributed by NNMR is found in Niger (19.6% in 2006) and the highest in Egypt (44.7% in 2005). In Northern Africa, it varies from 31.7% in Sudan to 44.7% in Egypt. In Western Africa, it varies from 19.6% in Niger to 41.3% in Mauritania. In Eastern Africa, it is lowest in Burundi (21.0%) and highest in Comoros (40.0%). In Middle Africa, it varied from 23.5% in Chad to 34.8% in Gabon. In Southern Africa, Swaziland has the lowest proportion (21.8%) and Botswana has the highest (40.0%). There are strong fertility-mortality linkages in Africa. For the 40 countries considered, all those with high age-specific adolescent fertility (AFR>100) and total fertility rates (TFR>5) also have the highest rates of NNMR and U5MR. Furthermore, neonatal and underfive mortality rates are consistently higher among adolescent mothers that women of older age groups. The secular decline in both fertility and mortality is most noticeable in Ghana for almost a generation (1988-2008). The data across surveys and countries quite often show highest rates of NNMR and U5MR among adolescent mothers or oldest mothers (aged 45-49 years). These patterns are depicted in Figure 4 (for NNMR) and Figure 5 (for U5MR). 4.Antenatal care and place of delivery Antenatal care provides opportunities for gestating women to get information on warning signs of complications during pregnancy, at delivery and beyond. Adolescent mothers are unlikely to utilize health care services before/during/after delivery, and there is a high level of unmet need for information on pregnancy complications in sub-Saharan Africa.25 Skilled attendance at childbirth is also crucial for reducing maternal and neonatal mortality; most obstetric complications occurring around the time of delivery are unpredictable. We use available time series data from African countries to assess rates of change using yearly rates of changes in use of reproductive health-related services by gestating women and their neonates. Yearly rates of changes in proportions of live births without antenatal care establish two distinct groups of countries across regions in Africa: those which have consistently experienced increases, and those which have had declining rates of changes over time. The three African countries with increasing yearly rates comprise: Madagascar (2.89%), Rwanda (0.77%) and 0.08% in Ethiopia in Eastern Africa; Nigeria (0.46%) and Togo (0.06%) in Western Africa. These increases are located among women aged 20-34 years in Nigeria (0.92%), 35 years or older in Togo (0.47%), adolescent mothers in Ethiopia (0.17%) and Tanzania (0.94%). They are generalized to all age groups in Madagascar (0.47% for adolescents, 2.87% for the 20-24 years old mothers and 6.42% for older mothers) and Rwanda (0.91% for teenagers, 0.87% for 20-24 years old mothers and 0.36% for older mothers). The yearly rates of changes have consistently declined in all other African countries, varying for all mothers from 0.22% (Ethiopia) to 9.96% (Mozambique), for teenagers from 0.03% (Nigeria) to 13.42% (Mozambique), for 20-34 years mothers from 0.13% (Togo) to 9.85% (Eritrea), and for older mothers from 0.95% (Nigeria) to 7.68% (Liberia). Countries which have achieved prominent performances in terms of reducing the prevalence of live births without antenatal care across all age groups consist of Mozambique, Eritrea, Senegal, Namibia, Liberia, Ghana, Burkina Faso and Mali. Of the 95 surveys and 40 countries examined, there are only three surveys/countries with consistently low proportions of adolescent women who both did not use antenatal care (under 5%) and delivered at home (less than 20%): South Africa (1998), Gabon (2000) and Namibia (2007). This suggests that accessibility and utilization of antenatal care and health facility delivery remain elusive for women (and adolescents) in most African countries. A contrasting link also exists between use of antenatal care and home delivery. Several countries have very low proportions of live births without prenatal care contrasting sharply with very high proportions of live births with home delivery. This is especially the case for Ghana, Liberia, Togo, Senegal, Kenya, Rwanda, Tanzania, Uganda, Zambia, Zimbabwe, Lesotho and Swaziland. In Northern Africa, over a quarter of live births had no antenatal care and over 30% of them took place at home. In the remaining countries, the proportions of live births without antenatal care and who were delivered at home are still uniformly high across ages at maternity and over time within countries. In Ethiopia for instance, over 70% of live births to women still have no antenatal care and over 90% of them still take place at home. Average yearly rates of change in prevalence of home deliveries have substantially increased in Madagascar, Tanzania and Zimbabwe. Declining yearly rates have been highest in Northern Africa (6.57% in Egypt and 5.77% in Morocco), and substantial in Western Africa (5.61% in Benin, 2.94% in Senegal and 2.11% in Ghana), Eastern Africa (3.37% in Malawi, 2.07% in Eritrea) and in Southern Africa (3.91% in Namibia). Mozambique has reduced quite substantially the prevalence of home deliveries among teenagers. Such findings and others 5. Medical maternity care We assess the extent to which levels and trends in neonatal mortality rates (NNMR) vary consistently and in the expected direction to the extent that medical maternity care (i.e., no antenatal care nor delivery care, either antenatal care or delivery care, both antenatal care and delivery care ) was received by the mother at the time of delivery. If we assume that births without antenatal or delivery care would have higher mortality risks than births with either antenatal care or delivery care, and that these births in turn would have higher mortality risks than those having benefited from both antenatal and delivery care, one would expect a gradient in the association between levels of neonatal survival and medical maternity care. Across 95 surveys for each of the 40 countries analyzed, such as association is inconsistent when there is no positive or negative association given the conjectured link. Our model predicts eight countries with two or more surveys behaving as expected with negative association between maternal maternity care and neonatal mortality rates: the vast majority is made of countries from Eastern Africa (Malawi, Rwanda, Uganda, Zambia and Zimbabwe), Guinea (Western Africa), Chad (Middle Africa) and Namibia (Southern Africa). Single-survey countries with expected negative associations consist of Sudan and Tunisia (Northern Africa), Congo, Congo DR and Gabon (Middle Africa), and Botswana, Lesotho, South Africa and Swaziland (Southern Africa). Trends in NNMR indicate robust and generalized declines in most regions and countries. The deepest (over 3% per year) declines in average yearly rates of change in NNMR among live births with full maternal medical care (both antenatal care and delivery care) are found in Eritrea (11.94%), Chad (8.74%), Malawi (7.00%), Benin (6.20%), Morocco (5.59%), Uganda (5.13%), Tanzania (4.18%), Mali (3.78%), Rwanda (3.72%), and Nigeria (3.16%). In contrast, the highest increases in yearly rates of change in NNMR among live births with full maternal medical care occurred in Ethiopia (58.04%) and Côte d'Ivoire (11.6%). Deleterious effects of lack of antenatal care are reinforced by increases in yearly rates of change in NNMR in Côte d'Ivoire (18.16%), Eritrea (6.50%), Nigeria (2.56%), Togo (1.22%), Kenya (0.96%), Mozambique (0.83%), Tanzania (0.26%) and Senegal (0.06%). These yearly rates of change in NNMR by maternal medical care show that medical maternity care does not necessary translate into better survival prospects. While full coverage with skilled birth attendants is a main objective of the MDG5, causal link between use of medical maternity care and decline in mortality is not straightforward. Provision of skilled obstetric care at health centers may not reduce maternal mortality due to structural constraints of implementation. 6. Contraception use among sexually active and unmarried men and women Meeting the unmet need for reproductive healthrelated MDG4 and MDG5 is critical as increasing numbers of adolescents and young people are sexually active and entering their reproductive years. A study of the age pattern of fertility in Africa found that premarital fertility accounted for 21 percent of all births and for 47 percent of births among women aged 12-26, and stressed that this pattern of high premarital fertility was indicative of low incidence of contraceptive use before the first birth among adolescents.26 Such findings and others 4,5,16-18,25 calls for a reorientation of the reproductive health policy and programs, which tend to target married women and women who have been pregnant once, while failing to address the contraceptive needs of young women before their first pregnancy. When we assessed trends in modern contraceptive use and condom use among unmarried sexually active men and women aged 1549 in 40 African countries (table not shown, available upon request), we found that with the exception of Comoros where the prevalence of modern contraceptive use tends to be consistently higher at each age group for unmarried sexually active women than their male counterparts, the prevalence of modern contraceptive use is generally higher among men than women within and between countries. The prevalence of contraceptive use among adolescent men and women is also lower than among people aged 20-24 years and the latter tend to use more modern contraceptive methods and condom than their older counterparts; this pattern is found in Benin, Botswana, Burkina Faso, Côte d'Ivoire, Guinea, Liberia, Mali, Senegal, Gabon and Namibia. The condom is the preferred method of contraception among adolescents, across time and space. 7. Progress towards MDG4 and MDG5 and waiting times to achieving the targets set for 2015 In our analyses, the average yearly rates of changes are calculated to classify countries according to their progress indicators. We start with the estimated underfive mortality rates (per 1,000 live births) and maternal mortality ratios (the number of maternal deaths per 100 000 live births) in 1990 and 2008, which show that these rates and ratios are very high in sub-Saharan Africa. We answer the following questions: a) what are the yearly rates of change in U5MR (respectively MMR) from 1990 to 2008 versus the yearly rates of decline needed to reach the targeted U5MR (respectively MMR) from 2008 to 2015? b) What is the expected year to reach the targeted U5MR (respectively MMR) for 2015 based on the MDG4 (respectively MDG5), assuming the yearly rate of change in U5MR (respectively MMR) from 1990 to 2008? In Africa, solely Egypt had by 2008 an average yearly rate of decline (7.27%) that allowed it to reach the targeted 2015 level of U5MR before the target date. The average yearly rates of decline in U5MR in Tunisia (4.60%) and Morocco (4.44%) are also above the yearly rate of decline needed to reach their MDG4 (3.53% and 3.93% for Tunisia and Morocco, respectively). In sub-Saharan Africa, at their average yearly rates of U5MR decline from 1990 to 2008, Madagascar (5.41%), Eritrea (5.11%) and Cape Verde (4.28%) are likely to achieve the MDG4 by 2015. Overall, only six African countries (Egypt, Tunisia, Morocco, Madagascar, Eritrea and Cape Verde) have reached by now or are on track to reach the MDG4 by 2015. Five sub-Saharan African countries (with three in Middle Africa) have missed both the targets and the trends: Congo, Zimbabwe, South Africa, Cameroon and Chad. These patterns are depicted in Figure 9. Average yearly rates of change in MMR in Africa portray regional and national features of trends in MMRs. All countries of Northern Africa (but Sudan with a yearly rate of decline of only 3.61% against the needed rate of decline of 9.83%) are likely to meet the MDG5 by 2015. The average yearly rates of decline in MMR needed to reach the MDG5 is uniformly too high for most African countries, especially those in Southern Africa, Middle Africa, Western Africa and Eastern Africa. Countries which are notable exceptions with respect to needed average yearly rates of decline to reach the MDG5 in Sub-Saharan Africa include Cape Verde (3.78%) and Equatorial Guinea (6.14%). These patterns are illustrated in Figure 10. To determine the expected year to attain the targeted U5MR and MMR for 2015, we calculated waiting times (in years) from 2008 to reach the targeted U5MR (respectively MMR) for 2015, assuming the yearly rate of change in U5MR (respectively MMR) from 1990 to 2008, and added these waiting times to 2008 to obtain that expected year. The expected year for African countries which will reach the MDG4 by 2015 include: Egypt (reached by 2008), Madagascar (2010), Eritrea (2011), Tunisia (2013), Morocco (2014), Cape Verde (2015). At their current yearly rates of change, several African countries are at risk of not achieving even by 2100, the MDG4 set for 2015, including Burkina Faso and Mauritania (Western Africa); Burundi and Kenya (Eastern Africa); Cameroon, Central African Republic, Chad, Congo, Congo DR (Middle Africa); and Botswana, Lesotho and South Africa (Southern Africa), as shown in Figure 11. Continental and national progress indicators of MDG4 and MDG5 are deceiving or at best mixed. Our analyses substantiate a recent report of the World Bank which notes that progress is too slow on healthrelated outcomes (e.g., maternal and child mortality) for the world to achieve these MDGs by 2015.27 VI. Conclusion and implications This study shows that poor sexual and reproductive health contributes to poor survival of mothers and children and to ill health among survivors, and impedes efforts for achieving the MDG4 and MDG5. There is an immediate need to place preconceptional and interconceptional influential factors on maternal and child health, in the context of women's health in her lifetime, to reverberate the Institute of Medicine.4 The contribution of adolescent fertility to total fertility in most African countries has changed little over time. Adolescent fertility is an indicator of reproductive health summarizing a wide range of issues including accessibility of information and services, relevant health risks, and the living conditions of young people including early marriage, and the risk of maternal mortality among very young adolescents is expected to be highest. Unintended pregnancy remains a major reproductive health problem among young people in sub-Saharan Africa where adolescent fertility accounts for 10 to 16 percent of total fertility. Sadly, little has changed in the last two decades since the Save Motherhood Initiative.4,19,25,27 Our findings on 51 African countries further confirm this trend and substantiate that while there is wide variation in early initiation of reproductive behavior and health outcomes across countries and between subgroups in the same country in Africa, the overall pattern is that of high adolescent fertility, unacceptably high levels of mortality of mothers and their offspring under-five, and reproductive health-related problems with immediate and long-term consequences on maternal and child health and survival. This study shows that while the quantity and accessibility of maternal maternity care services has generally increased in most African countries, the quality may not have increased given the continuing high levels of neonatal mortality. This might be one reason that progress has been slower for MDGs measured by outcomes (i.e., MDG4 and MDG5) than for those measured by access to maternal medical health care services. Programs aimed at improving incentives for service providers and consumers and making service providers directly accountable to users are essential to improving MDG-health related outcomes, as pinpointed by the World Bank in its Global Monitoring Report 2011.27 Such programs should be implanted within a lifespan framework covering preconceptional and interconceptional periods as targets for intervention in improving health and well-being for women and under-five children in Africa. Indeed, a woman regardless of life options will spend the bulk of her reproductive life span in either preconceptional or interconceptional periods. Acknowledgements This study is an extended version of a paper commissioned by the United States National Academy of Sciences (Washington DC, USA), which was presented at the Fifth Annual International Conference of the African Science Academy Development Initiative (ASADI) Conference on “Maternal, Newborn and Child Health in Sub-Saharan Africa”, held in Accra (Ghana) on November 10-11, 2009. This extension was carried out while Prof. Barthelemy Kuate Defo was on sabbatical research leave at INED (Paris, France). References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11017f9.jpg] [rh11017f10.jpg] [rh11017f3.jpg] [rh11017f4.jpg] [rh11017f8.jpg] [rh11017f6.jpg] [rh11017f11.jpg] [rh11017f5.jpg] [rh11017f7.jpg] [rh11017f1.jpg] [rh11017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}