 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
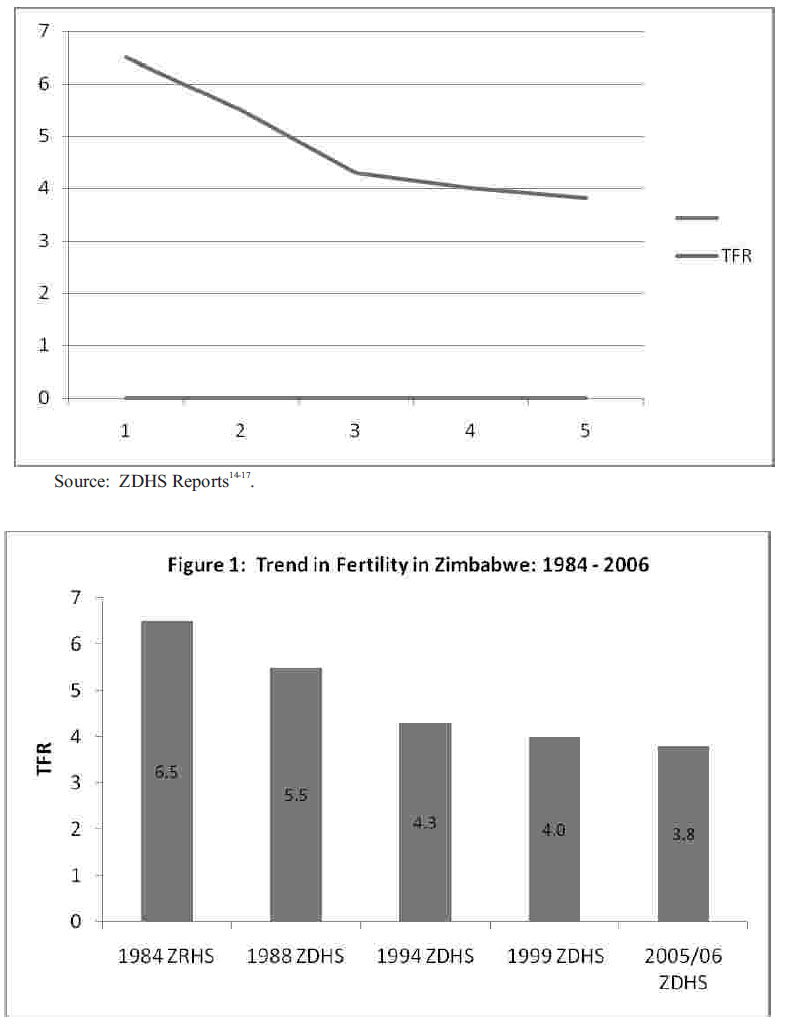
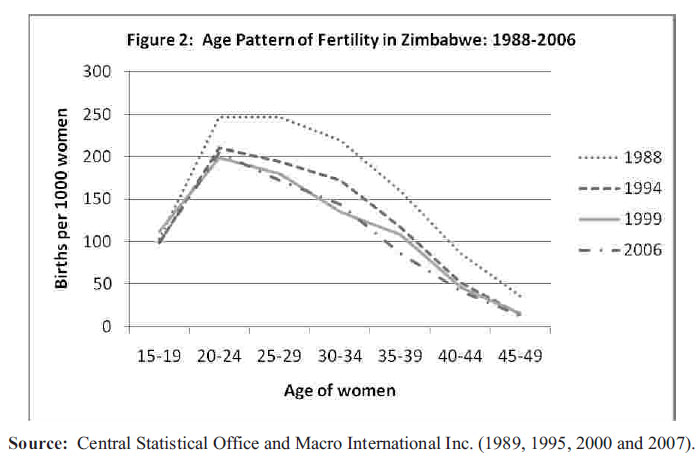
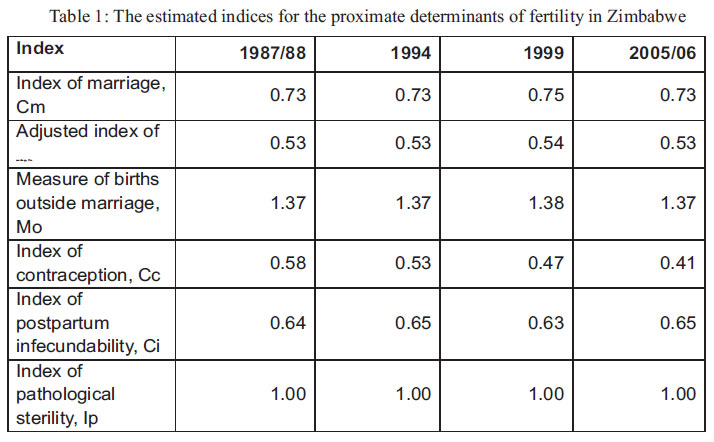
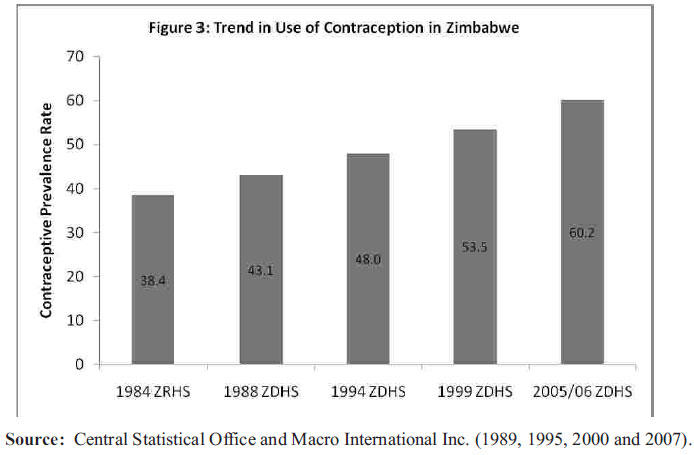
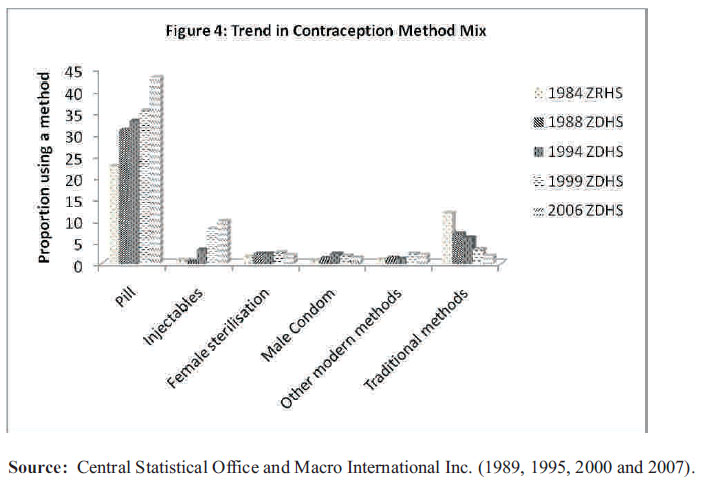
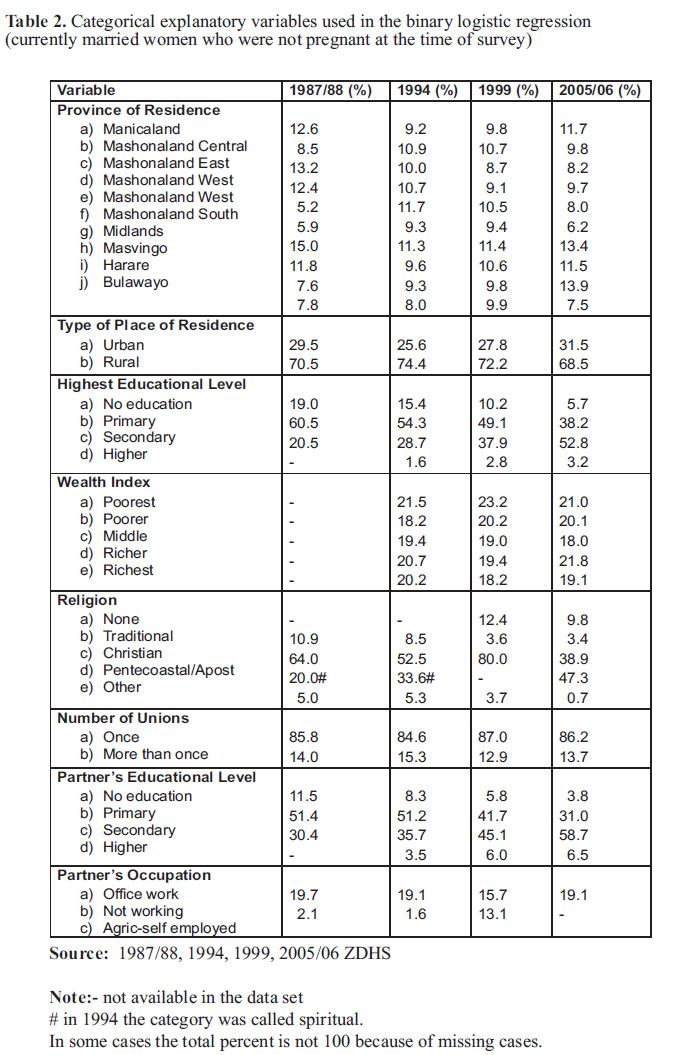
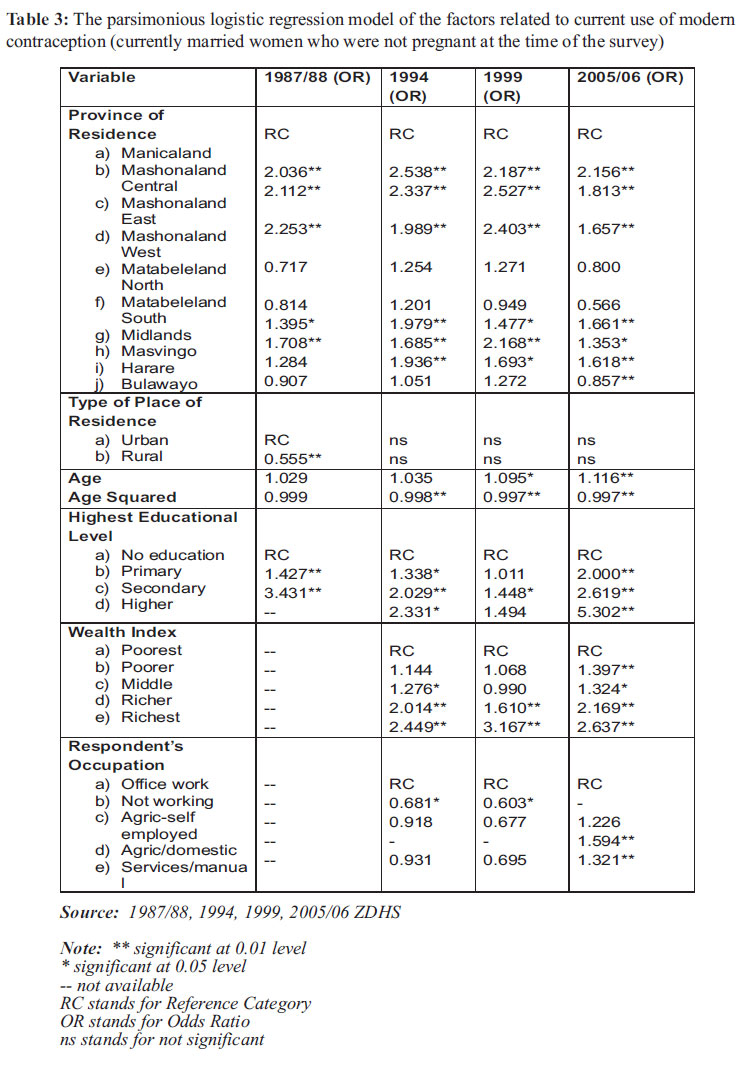
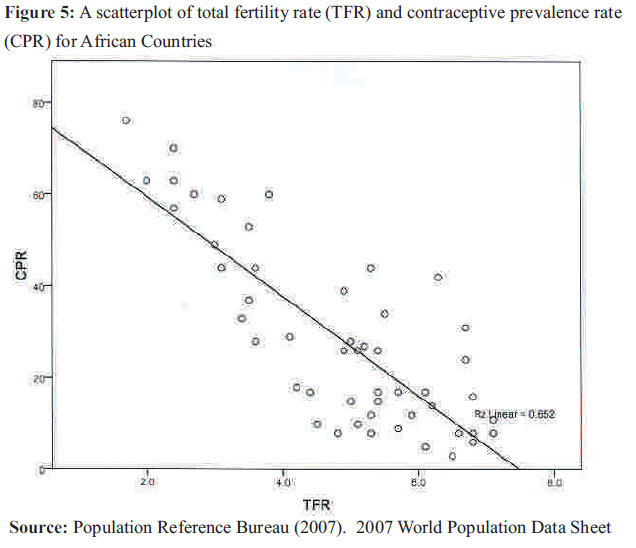
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 31-44 ORIGINAL RESEARCH ARTICLES Falling Fertility and increase in Use of Contraception in Zimbabwe Akim Mturi1 , Kembo Joshua2 1Population Training and Research Unit, Faculty of Human and Social Sciences, North-West University (Mafikeng Campus), Mafikeng, South Africa. 2 Bureau of Market Research University of South Africa Pretoria, South Africa. For Correspondence: Akim.Mturi@nwu.ac.za Code Number: rh11018 Abstract Zimbabwe does not feature much on the current debate of fertility transition in sub-Saharan Africa. This article is trying to fill this gap by analysing the ZDHS data. The total fertility rate of Zimbabwe was close to 7 births during independence in 1980. However, it has declined to 3.8 in 2006. This does not only show that fertility in Zimbabwe has been declining over the years, but it is one of the lowest in the region. The fertility trend observed is mainly explained by use of contraception. The contraceptive prevalence rate was 60 percent in 2006. It is noted that the contraceptive uptake has continued to increase even during the years when Zimbabwe was going through serious political, economic, social and health challenges. This is because the groundwork done on the family planning programme soon after independence put a solid foundation in motivating women to use contraception. Résumé Le Zimbabwe ne figure pas beaucoup dans le débat actuel sur la transition de la fécondité en Afrique subsaharienne. Cet article essaie de combler ce vide en analysant les données de l'EZDS. Le taux de fécondité totale de Zimbabwe est à peu près 7 naissances pendant l'indépendance en 1980. Néanmoins, il a chuté jusqu'à 3,8 en 2006. Ceci montre que non seulement la fécondité au Zimbabwe baisse au cours des années, mais elle est une de plus faibles de la région. La tendance de la fécondité que nous avons constatée est largement expliquée par l'emploi de la contraception. Le taux de la prévalence contraceptive était de 60% en 2006. On constate que l'acceptation ne cesse de s'accroitre même pendant les années ou le Zimbabwe traversait des moments difficiles sur les plans politiques, économiques, sociaux et sanitaires. Ceci parce que le travail préparatoire qui a été fait sur le programme de la planification familiale peu après l'indépendance a assuré une base solide à la motivation des femmes à utiliser la contraception. Key words: Fertility, Family Planning, Contraception, Zimbabwe, Sub-Saharan Africa Introduction Fertility is highest in sub-Saharan Africa than any other region in the world. Until late 1980s it was believed that fertility rates did not have any indication of declining. The reasons behind the persistently high fertility rates in the region have been suggested to include strong pronatalist forces inherent in the kinship system in Africa1 . This has caused a considerable controversy over the likelihood of fertility rates declining in the near future in sub-Saharan Africa. The analyses documented since 1990 based on the Demographic and Health Surveys (DHSs) have shown a different impression. Fertility levels were still the highest in the world but a declining trend was observed in several African countries notably Kenya, Botswana and Zimbabwe2-4. South Africa was also among this group of countries5 , but it was less documented because of the international isolation caused by the apartheid policies. Since then more countries observed fertility decline in the region. Of the three countries, Kenya has been documented more than the two. Recently, a Population Council study showed that the fertility decline in Kenya has stalled meaning that it is not declining any more6 .This finding has motivated the current study by looking at Zimbabwe as one of the champions of fertility decline in Africa. Is fertility trend in Zimbabwe still declining or has stalled like Kenya, and what is determining the observed trend? In the past two decades or so, Zimbabwe has changed a lot. In early 1990s, it used to be a glamorous country in many aspects. The economy was strong, the infrastructure was one of the best in Africa and the health sector was very sound. Potts has commented on the urban population of Zimbabwe that in the beginning of 1990s it was less poor and generally more economically and socially secure than any urban population in sub-Saharan Africa . 7Things started to deteriorate from mid-1990s. By late 1990s, a political and economic crisis unfolded in Zimbabwe. As a result the country witnessed a twodigit negative growth rates, a sky-rocketing inflation, a decline in the rule of law and a disintegration of markets8 . Before the collapse of the local currency (in 2008), it was not surprising to find a bank note of one million Zimbabwe dollars displayed in various places around the world to indicate that that was the highest denomination of a bank note and yet it does not have much value. One expects this kind of changes in a country to have an impact on various demographic outcomes. This is so much the case for childbearing which depends mainly on a public driven family planning programme. The hypothesis is that people who are living under so much stress because of poverty will not have time and energy to look for contraceptives (even if they are available) for limiting or stopping births. The article presents the trend in and pattern of fertility in Zimbabwe during the post independence period (i.e. 1980 – 2006). The determinants of fertility trend in contraceptive use are also analysed and discussed. In addition, the paper discusses the future fertility prospects given the new twist on the political situation of the country and economic recovery witnessed in the last few years. The specific objectives of the article are outlined as follows:a) To examine the fertility trend in Zimbabwe; b) To investigate the proximate determinants of fertility; c) To assess the performance of the family planning programme over the years; d) To discuss the factors associated with use of modern contraceptive methods; and e) To explore the future fertility decline prospects. Data and Methods of Analysis Zimbabwe has been conducting a series of the Demographic and Health Surveys (ZDHS) since the beginning of the worldwide DHS programme. The first post-independence national survey to collect demographic and health data was conducted in 1984. This opened way to four ZDHSs in 1987/88, 1994, 1999 and 2005/06. These five data sets are used as data source for this article. All data sets have been used before by various authors for fertility analysis except for the 2005/06 ZDHS. The descriptive analysis will be used in examining the trend in and pattern of fertility by making use of the tabular as well as graphical analyses. The proximate determinants of fertility will be analysed using the Bongaarts' Model. Bongaarts has developed a framework for analyzing the proximate determinants of fertility which he later elaborated with his colleagues9-10. The framework shows that group variation in fertility is due to four main factors: proportion of women married; practice of contraception; induced abortion; and period of lactation infecundability. Each factor can be represented by an index which take a value between 0 and 1 depending on the magnitude of the fertilityinhibiting effect. That is, the closer the index is to 1 the weaker the fertility-inhibiting effect and its effect becomes strong if the index is closer to 0. Although the Bongaarts Model has been very useful in understanding the proximate determinants of fertility, several shortcomings have been documented 11 . However, in the absence of a different model to serve the purpose we have decided to use the Bongaarts Model, as refined by Jolly and Gribble12. The refinement includes adjusting the index of marriage to take into account births outside marriage and introducing the index of pathological sterility. The factors associated with use of modern contraceptive methods are analysed using the binary logistic regression analysis. This choice is due to the fact that the response variable is dichotomous, that is, one is given to a woman who is using any modern method and zero is for a woman who is either not using any method or is using a method that is not classified as modern. The explanatory variables were selected taking into account the association reported in the literature. These include women's characteristics such as age, education, residence, occupation, religion and selected partners' characteristics. Trend in and Pattern of Fertility The first post-independence national survey was conducted in Zimbabwe in 1984 under the name Zimbabwe Reproductive Health Survey (ZRHS). The total fertility rate (TFR) estimated for women aged 15-49 was 6.5 births per woman13. As shown in Figure 1, the 1987/88 ZDHS indicated that TFR declined by one birth to 5.5. Although not at the same pace, the decline in fertility continued as the 1994 ZDHS registered a TFR of 4.3 and the 1999 ZDHS estimated a TFR of 4.0. The most recent ZDHS of 2005/06 showed that, for the first time in Zimbabwe, the TFR declined to less than four births. In other words, during the two decades, Zimbabwe managed to reduce TFR by 2.7 births per woman. This represents a fertility decline of 41.5 percent. This is a remarkable fertility decline for a sub-Saharan African nation. The age pattern of fertility during the period 1988-2006 is presented in Figure 2. It can be observed that Zimbabwe has been moving from the broad peak to early peak. In 1987/88, fertility rates were similar for age groups 20-24 and 25-29. This changed in 1994 as the the fertility rate for age group 20-24 was slightly higher than 25-29. It was very clear in 1999 and 2005/06 that age group 20-24 was having a higher fertility rate than 25-29, indicating an early peak. Figure 2 also shows that teenage fertility has remained at more or less the same rate over the years. With the exception of 1984, the fertility rate for women aged 40-44 and 45-49 has not changed much as well. Which means the bulk of fertility changes over the years took place for 20-39 year olds. Another observation of the age pattern of fertility presented in Figure 2 is that the curves for survey years 1987/88, 1994 and 1999 do not cross any where except for teenagers. But the 2005/06 curve do cross the 1999 curve. Based on this evidence, one may conclude that the characteristic of African fertility transition mentioned by Caldwell and others that fertility decline is found at all ages perhaps applies only at certain stages of the transition 3. Figure 2 shows that when TFR is 4 or higher, fertility declines at all ages except teenagers. But when TFR gets lower, there is a distortion as some ages experience a rise in fertility. Proximate Determinants of Fertility Table 1 presents an analysis of the indices of the proximate determinants of fertility in Zimbabwe. The indices that are depicted in Table 1 relate to marriage, contraception, postpartum infecundability and pathological sterility. These indices are shown for the years 1987/88, 1994, 1999 and 2005/06. It should be noted that the index of pathological sterility, Ip, computed was greater than 1 in all surveys indicating that the value of 1 should be assigned12. It is also important to point out that the data for the computing the index of abortion are not available hence was excluded from this study. The data indicates that there is a consistent decline in the index of contraception (Cc) from 0.58 in 1987/88 to 0.41 in 2005/06, which confirms that use of contraception played a significant role in fertility decline in Zimbabwe. Conversely, it would appear that the contribution to fertility decline from the other indices, namely the index of marriage and the index of postpartum infecundability is marginal. The adjusted index of marriage (C'm) fairly remained constant at 0.53 from 1987/88 to 2005/06. This indicates that the marriage is not a significant factor in explaining the observed fertility decline in Zimbabwe between 1987/88 and 2005/06. It should be noted also that 37 percent of births in Zimbabwe were born outside marriage during the period under study. The index of postpartum infecundability (Ci) also remained fairly the same during the period under review. Thus postpartum infecundability had a minor effect in reducing fertility during this period. Contraceptive Prevalence and the Family Planning Programme The contraceptive prevalence rate (CPR) is the proportion of currently married women aged 15-49 who are currently using any form of contraception. Use of contraception was classified to be low just after independence in 1980. Boohene and Dow Jr reported that only 14 percent of married women were using modern contraceptives in 1980-8118. But as Figure 3 depicts, the trend in CPR during the period 1984-2006 was very promising. Over the years Zimbabwe has been very successful and the leader in the region in terms of use of contraception. The 1984 ZRHS estimated a CPR of 38.4 percent. This rate was quite high comparing with CPR of other African countries at the time. It consistently increased over the years. By 1999, over half of the married women in childbearing ages were using contraceptives. The 2005/06 ZDHS showed that the CPR had increased to 60.2 percent. Figure 4 presents the proportion of women using different types of contraceptives over years. It is very clear that the pill is the most used type of contraception in Zimbabwe. The proportion using the pill has been increasing consistently from just over 20 percent in 1984 to well over 40 in 2005/06. The second most used contraceptive is injectables. However, the proportion was just under 10 percent in 2005/06. It is surprising that male condoms is minimally used in Zimbabwe especially because Zimbabwe is one of the African countries most affected by the HIV and AIDS epidemic, with the adult HIV prevalence of 18 percent in 2005/0614. The discussion above shows that Zimbabwe is a success story as far as the family planning programme is concerned. In fact, it is only South Africa that has a family planning programme that is performing better (using contraceptive prevalence rate as an indicator) than Zimbabwe in sub-Saharan Africa. What makes the Zimbabwe Family Planning Programme perform this well given a long list of challenges the country is facing? One would expect that the era of political, economic, social, and health challenges that has lasted for almost two decades should have run down any previous efforts of motivating people to use contraception but this is not the case. This section tries to outline the reasons behind the good performance of the Family Planning Programme. It will be observed that the foundation lied down especially during the period just after independence was secret behind this success. Maggwa et al report that modern family planning methods were first introduced in Zimbabwe in 1953 and there was no formal structure to coordinate these activities until 1965 when the Family Planning Association of Rhodesia (FPAR) was established19. The association was mainly financed by the government which made it possible to expand rapidly especially in urban centres (Boohene and Dow Jr, 1987). During the early years, the association concentrated on the distribution of the pill to the extent that the fieldworkers were nicknamed pill agents18. This effort made the pill to be the main method used to date. However, during the mid-1970s to the period of independence, many indigenous people perceived family planning as a strategy used by Europeans to reduce the African population while increasing their own18,19 . This notion affected the family planning efforts negatively. Short period after independence (September, 1981), the new government took over the FPAR and worked hard to change the image of the Family Planning Programme. In 1984, the association was changed into a parastatal organization under the Ministry of Health and the name of the organization was changed to Zimbabwe National Family Planning Council (ZNFPC) with a mandate of guiding family planning policy development on behalf of the Ministry of Health19. The commitment of the Zimbabwe government, through ZNFPC, on the Family Planning Programme was unquestionable. Lee et al report that the then first lady (Sally Mugabe) provided high-level leadership, and she worked very closely with her sister (Ester Boohene) who later became the director of ZNFPC. The political will from the very beginning made a serious contribution to the foundation we observe today20. Zinanga, a former director of ZNFPC, outlines the laws on family planning that have been put in place in Zimbabwe since the early years of independence as another mechanism that helped the Family Planning Programme21. The first is the Zimbabwe National Family Planning Council Act of 1985 which outlines the responsibility of the ZNFPC. There are various other laws and policies that encourage and promote use of family planning in Zimbabwe. This includes the abolition of fees for the low income group, which removed one of the barriers to contraceptive use21. Other initiatives were various ways to target the rural population in terms of availability and accessibility of contraceptives such as providing family planning services through the Primary Health Care system and using an old prescription to get supply of contraceptives21. Another effort done after establishing ZNFPC was to expand it and its functions. By the end of 1980s, the ZNFPC had a total of six units. Three service units that operated nation-wide: Community-Based Distribution (CBD); Medical/Clinical, and Youth Advisory Services. And three support units namely the Information Education and Communication; Evaluation and Research; and Training. The CBD, which mainly supply oral contraceptives and condoms, was and still is the principal means of outreach. Although there were problems observed, an assessment conducted in 2001 indicated that CBD is still performing reasonably well across the country and managed well at provincial level19. The improvement of the status of women in Zimbabwe has also played a key role in the success of the Family Planning Programme. Mhloyi and Mapfumo have explained the efforts made since independence to change the status of women which included expansion of the education system which gave more opportunities to women and legislative changes that gave women the right to own property and to enter into contracts22. Hindin in further analysis of ZDHS 1994 data also showed that women's household decision-making autonomy played a significant role in fertility-related behaviour in Zimbabwe23. In that study, Hindin observed that women who had no decision-making autonomy had 0.26 more children than women who had some decision-making autonomy23. It can be concluded therefore that the foundation on having smaller families and motivation of using contraception was very solid. Hence the family planning programme continued to be relevant to people even when they were facing many challenges. Multivariate analysis of the factors associated with current use of modern contraceptive methods The binary logistic regression analysis was used to analyse the factors associated with current use of modern contraceptive methods. Women who were not currently married or living with a man were excluded in the analysis. In addition, women who were pregnant were excluded from the analysis. The dependent variable is use of modern contraceptive methods. Women who were using any modern method (i.e. female sterilization, male sterilization, pill, IUD, injectables, implants, and male condom) at the time of the survey were coded one. Women who were not using any method, or who were using either traditional or folk methods were coded zero. Based on the literature, twelve explanatory variables were chosen from the data sets. Table 2 presents the frequency distribution of eleven explanatory variables. The twelfth variable is 'age' of respondent which is a continuous variable. It was also important to include 'age squared' since age is known not to have a linear relationship with use of contraception. It should be noted that variables were identical in all data sets except the 1987/88 ZDHS which missed wealth index and respondent's occupation. The parsimonious logistic regression models were fitted for four data sets: 1987/88, 1994, 1999 and 2005/06 ZDHS. The results are presented in Table 3. Both 'age' and 'age squared' were included in all four models whether they were significant or not because they are basically control variables. The geographical location of the respondent which is represented by the province of residence is a very important predictor of use of modern contraceptive methods. The reference category is the Manicaland province. Women who were residing in five provinces (Mashonaland Central, Mashonaland East, Mashonaland West, Midlands and Masvingo) were found to be consistently more likely to use modern contraceptive methods compared to Manicaland. Whilst the odds ratio indicating use of modern contraception for Harare (the capital city) was not significant in 1987/88, women in other surveys were found to be more likely to use modern contraception than those residing in Manicaland. Bulawayo (the second urban centre in Zimbabwe) residents were not significantly different to Manicaland except for the most recent ZDHS (2005/06). Also women residing in Matabeleland North and Matabeleland South were not significantly different to Manicaland province in all four surveys. The observed variations in use of modern contraception could partly be due to the variation in the demand and supply of modern contraceptives among these provinces in Zimbabwe. For instance, an assessment of the Zimbabwe National Family Planning Council's community based distribution programme conducted in 2001 indicated that the average number of visits (for both new and re-visit clients) undertaken by community based distributors (CBDs) during 1998 in Manicaland (803) was below the national average (918). CBDs in Mashonaland East, Midlands, Mashonaland Central and Mashonaland West conducted 1433, 1155, 1055 and 985 visits respectively19. The relatively higher proportions of women using modern contraception in Mashonaland Central, Mashonaland East and Mashonaland West provinces could also partly be attributed to the proximity of these provinces to Harare and Bulawayo in the case of Masvingo and Midlands provinces. Manicaland province has the highest population density (44 persons per kilometre) in Zimbabwe and the highest number of health facilities. Accessibility to these services (including family planning services) is hampered by geography. Manicaland province is highly mountainous. In Manicaland, metric distance from home to health facility is very low, due to the high density of health facilities, but time distance is the longest. This implies that for a community health worker (CBDs included), it takes longer to travel a distance unit, say 1km relative to other provinces in Zimbabwe. Notably also, Matabeleland North and Matabeleland South provinces have the least population densities (9 persons per kilometre) and health facilities are few and sparse. The foregoing could be explanations for the observed provincial differentials in the use of modern contraception in Zimbabwe. Type of place of residence has been found to be related with use of contraception in many African countries24 . Women residing in rural areas are less likely to use contraception compared to urban dweller. The same pattern has been observed in Zimbabwe in 1987/88. However, the significance of the type of place of residence disappears when the wealth index is introduced in the models for 1994, 1999 and 2005/06 data sets. Note that the 1987/88 data set did not have a wealth index variable. As expected, women who are living in households that have high score in their wealth index are more likely to use modern contraceptives than those in poorest households. In fact, women in the richer and richest quartiles are consistently significant in the three surveys. What is there in the wealth index that makes type of place of residence insignificant? It seems the main reason causing women who reside in rural areas to use contraception less than those residing in urban areas is due to the deteriorating economic situation. Although Zimbabwe as a country has been facing serious economic problems, the rural areas are affected more than urban. Women's and their partner's characteristics are known to have influence on use of contraception. The educational level of women has been cited as the most important variable associated with contraceptive use in many countries. It has been observed that better educated women are more likely to use contraception than women with no education24. The Zimbabwean situation reflects this pattern. So the investment of Zimbabwean government on education has assisted a lot in motivating women to use of modern contraceptives22, 25 . Table 3 shows that partner's education has a stronger and more consistent relationship with use of contraception. The higher the level of education of a partner the more likely the woman will use contraception. This is not only about having knowledge of both availability of contraceptive methods and where to get them, but also it indicates that these women are motivated to stop giving birth or space the births. Respondent's occupation has been found to be related with use of modern contraception. Women who are not working are less likely to use modern contraceptive methods that those who have 'office' work in 1994 and 1999. The 2005/06 data set shows that women who are working in the agricultural sector as labourers, domestic workers, those doing services and manual jobs are more likely to use modern contraceptives than those who have 'office' work. These types of work are known to pay less and usually do not have the benefits like maternity leave, hence women working in these sectors are less motivated to have children. It should be noted that partner's occupation was not found to be significant in any of the four models. The sample analysed includes only currently married women, so the issue of marital status does not arise. However, the number of lifetime marriages a woman has been involved with has been included in the analysis. Women who have been married more than once are less likely to use modern contraceptives than women who have been married only once. This finding is consistent in all four surveys. There is a tendency of women trying to have children in every relationship they join so these women are not likely to use contraceptives. Judging from the size of the odds ratios, the total number of living children a woman has a strong influence on using or not using modern contraceptives. The higher the number of living children the woman has the higher the likelihood of using a method. The same applies with the number of dead children. Women who have lost some of their children are less likely to use a method than those who have not lost any. No wonder some researchers have suggested that reduction of childhood mortality is a prerequisite for reduction in fertility26. Zimbabwe is a predominantly a Christian society. Just a small proportion of women said they don't have any faith or are Muslims or they have traditional religion. It is therefore not surprising to find out that religion is not associated with use of modern contraception as most women have the same belief. Concluding Remarks This study has presented the declining trend in fertility in Zimbabwe. TFR was estimated to be 6.5 in 1984, which declined to 3.8 in 2005/06. Currently, Zimbabwe has one of the lowest fertility rates in the region. The analysis of the proximate determinants of fertility showed that the decline of fertility was mainly caused by use of contraception. The proportion of currently married women aged 15-49 years who were currently using contraception was 14 percent just after independence in 1980-81, this has increased to 60.2 percent in 2005/06. The index of contraception (Cc) decreased from 0.58 in 1987/88 to 0.41 in 2005/06. It should be noted also that the contraceptive prevalence rate (CPR) in Zimbabwe is one of the highest in sub-Saharan Africa. The paper has discussed the history of the family planning programme in Zimbabwe. It seems there is good explanation as to why the programme continued to perform well even after the country went through political, economic, social and health challenges during the last two decades. The main explanation is that there was a solid foundation on the family planning programme which did not change focus that much during the crises. Zimbabwe is therefore a typical example of a country where experienced high contraceptive usage and low fertility when poverty is at a high level. The factors associated with use of modern contraceptive methods were analyzed using the binary logistic regression model. All four data sets collected during the period 1987-2006 showed that there are significant provincial variations on use of modern contraceptive methods. This implies that there is a need to look at province specific intervention for the high rates of use of contraceptive methods to continue. For example, the community based distribution, which is one of the major methods utilized in Zimbabwe for the distribution of contraceptive methods, should be assessed by province. Good practices for the provinces doing well should not be copied mechanically to other provinces but should help in considering what to do in the provinces that are not doing well. The wealth index is also found to have a significant effect on use of modern contraceptive methods in all four surveys. Women residing in better off households are more likely to use modern methods than other women. Various women and their partner's characteristics have been found to influence use of contraception, including childhood mortality and the family size. The future prospects of fertility decline in Zimbabwe depend on a number of factors. The first issue is that of mismatch between the level of use of contraception and fertility rate. Figure 5 presents a scatterplot of TFR and contraceptive prevalence rate (CPR) for countries in sub-Saharan Africa which had such data in 2007. The regression line shows where a country is expected to be if TFR is a true reflection of CPR. It is clear from the figure that Zimbabwe has high TFR given the level of CPR observed. Further studies on fertility in Zimbabwe need to address this issue. The other factor to look at is that the most popular contraceptive method used is the pill. Given that the pill is used for spacing purposes, there is need to find ways to market other methods especially those intended for stopping births. The future prospects of fertility decline in Zimbabwe look gloomy unless the issues of TFR and CPR mismatch and use of mainly pills are seriously addressed. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11018t3.jpg] [rh11018f2.jpg] [rh11018f5.jpg] [rh11018f1.jpg] [rh11018t1.jpg] [rh11018f3.jpg] [rh11018t2.jpg] [rh11018f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}