 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 45-56 ORIGINAL RESEARCH ARTICLES Trends in contraceptive use among female adolescents in Ghana Lutuf Abdul-Rahman1* , Gaetano Marrone2 , Annika Johansson2 1 Pals Solutions P. O. Box TL 430, Tamale –Ghana, 2 Division of Global Health, Department of Public Health Sciences, Karolinska Institutet, Stockholm-Sweden Code Number: rh11019 Abstract Within the past one and half decades many efforts have been made to improve the availability and access to adolescent sexual and reproductive health services. Despite these efforts, adolescents still face a number of sexual and reproductive health problems. This paper uses data from the 2003 and 2008 Ghana Demographic and Health Surveys to examine changes in contraceptive use among sexually active female adolescents (15-19 years old). The results show that between 2003 and 2008 there was a significant increase in the current use of any contraceptive method (from 23.7% to 35.1%, p=0.03). It also indicates a shift from modern to traditional contraceptive methods. Traditional methods recorded about 60% (7.8 percentage points) increase as compared to 5.5% (2.6 percentage points) for modern methods. Also ever use of any traditional method recorded a higher increase as compared to any modern method. There was a slight decline 7% (4.4 parentage points) in the number of non-users who intended to use contraceptives in the future. On the whole the findings indicate increasing unmet need for modern contraception due to barriers such as limited access, cost and misconceptions about the effects of contraceptives. Résumé Depuis maintenant une d écennie et demie, on a fait beaucoup d'effort pour améliorer la disponibilité et l'accès aux services de la santé sexuelle et de reproduction. Malgré ces efforts, les adolescentes font toujours face à un nombre des problèmes de la santé sexuelle et de reproduction. Cet article se sert des données tirées des Enquêtes Démographiques Ghanéennes de 2003 et 2008 pour examiner les modifications dans l'usage des contraceptifs chez les adolescentes sexuellement actives (âgées de 15-19). Les résultats montrent qu'entre 2003 et 2008, il y a eu une augmentation importante dans l'usage actuel de n'importe quelle méthode contraceptive (de 23,7% à 35,1%, p=0,03). Ils indiquent également un changement des méthodes contraceptives modernes vers les méthodes traditionnelles. Les méthodes traditionnelles ont enregistré une augmentation d'environ 60% (points de pourcentage de 7,8) par rapport au 5,5% (points de pourcentage de 2,6) pour les méthodes modernes. En ce qui concerne celles qui ont déjà employé les méthodes modernes, il y a eu une augmentation plus élevée par rapport à n'importe quelle méthode moderne. Il y a eu un petit déclin de 7% (points de pourcentage de 4,4) dans le nombre de non usagers qui voulaient employer les contraceptifs dans l'avenir. Dans l'ensemble, les résultats ont montré une augmentation dans les besoins non satisfaits à l'égard de la contraception moderne dû aux obstacles tels l'accès limité, le coût et les idées fausses concernant les effets des contraceptifs. Key words: Adolescents, young people, contraceptive use, sexually active, Ghana Introduction Young people, (15 to 24 years old) who represent one sixth of the world population1 , face a number of sexual and reproductive health problems. Key among these are sexually transmitted infections (STIs) especially HIV, teenage and unwanted pregnancies. There are about 12 million young people living with HIV and AIDS globally of whom 62% live in Sub-Saharan Africa. An additional 6000 are infected every day, representing more than 50% of all new HIV infections in the world 2. Globally, adolescent girls (15 to 19) account for 14 million births annually2 . These births put them at high risk of death and lifelong complications because they are still not well developed to start child bearing. The birth rates among female between 15 to 19 years in Africa is estimated at 143 per 1000, which is two times more than the world average of 653 .Many have unwanted pregnancies4 some leading to abortion. Because of the limited availability and high cost of abortion service when these young people decide to abort a pregnancy they usually resort to unsafe methods. These unsafe abortions have been reported to be a major contributor to the high rates of morbidity and mortality among adolescent girls and young females 5 . In a review of 69 studies on unsafe abortion published between 1985 and 2002, Shah and Ahman estimated that young people account for 57% of all unsafe abortions occurring in Africa 6 . Abortions are very controversial in Africa, with most countries still having laws which prevent access to safe abortion services. According to the United Nations Population Fund (UNFPA) sub-Saharan Africa has the lowest demand (30%) and use (20%) of contraceptives among 15-19 year olds. They further commend that lack of access to family planning services and negative attitudes of health workers towards adolescent contraceptive use have contributed to high rates of pregnancies among adolescent1. The problems faced by adolescents in Ghana are not too different from their counterparts all over Africa. They include teenage pregnancies, low knowledge and usage of contraceptives, high fertility rates and high incidence of HIV. For example between 2008 and 2010 the HIV prevalence among young people (15 to 24 years old) in the country increased from 1.9% to 2.1% 7. According to the 2008 Ghana Demographic and Health Survey (GDHS) about 14% of all Ghanaian female adolescents have started child bearing, with only 8.0% of them using contraceptives8. Adolescents in Ghana have also been reported to have a generally poor knowledge on contraceptives8. According to Kumi-Kyereme et al pre-marital pregnancies and HIV are the main health problems of adolescents in Ghana9 . They have also been reported to have the greatest unmet need for family planning (want to delay or stop childbearing but are not currently using contraceptives). About 62% of them have unmet need as compared to 33% among 30-34 year olds10. Unfortunately the pre-marital sexual especially among adolescents is highly unacceptable in all Ghanaian cultural and religious settings. This makes it difficult for the adolescence to discuss any sexual problems they might have with adults for support. Anecdotal evidence shows that some health workers even turn away young adolescence you come to their health facilities to seek for family planning services. There have been a number of studies carried out on youth sexual and reproductive health (SRH) in Ghana. These studies however present little information on the behaviour of adolescents over time11, 12. Most of the recent studies focus on specific regions, districts or communities within the country; they therefore fail to give a clear picture of adolescent sexual and reproductive health (ASRH) in the country. Nonetheless, national level information is needed to assess how the country is meeting the SRH needs for the adolescents. This information is also required to evaluate current changes in ASRH12. In line with this thinking, the National HIV/AIDS and STI Policy specifically called for more research on youth sexual and reproductive health (SRH) and vulnerability to HIV in particular. This study therefore explores changes in contraceptive use among sexually active female adolescents (15-19 years old) in Ghana by comparing the data from two demographic and health surveys. Data and Methods Data from the GDHS conducted in 2003 and 2008 was used for this study. The GDHS is a quantitative study that collects data using closed ended semi structured questionnaire. Respondents for the GHDS 2003 and 2008 were selected using multistage random sampling. This sampling technique was adopted to permit the reliable calculation of key demographic indicators such as infant and under five mortality, fertility, contraceptive prevalence and nutritional status for the whole country, each region and for rural and urban areas8; 13 . Sample clusters were selected using the enumeration areas of the 2000 Ghana Population and Housing Census. The first stage of the sampling was carried out using probability proportional to size sampling techniques in which the number of clusters selected in each region was proportional to its population. In both surveys 412 clusters were selected at this stage (ibid). The second stage of sampling involved the selection of households within each cluster using systematic sampling. The aims of this stage of the sampling was to guarantee that sufficient number of completed individual interviews was carried out to provide estimates for key indicators with adequate precision. The number of households selected was 6,628 and 12,323 for the 2003 and 2008 GDHS respectively. Half of the households sampled were selected for individual interviews. In these households all women between 15 – 49 years and men 15 – 59 years were interviewed using the individual woman and man questionnaires respectively. The women questionnaire was used to collect information on issues about background characteristics, reproductive history, knowledge and use of family planning, reason for non-use, intention for future use of contraception, sexual activity, etc. It was also used to collect information on child health and nutrition and antenatal and postpartum care. Apart from the section on domestic violence in the 2008 survey, and that on birth histories and child health and child nutrition, the men questionnaire contained the same questions as the women one. This study makes use of responses to selected questions in the women questionnaire. Respondents 15 -19 years old in the women data set who had had sex within four weeks preceding the survey were selected for this study. There were 198 respondents in this category in 2003 and 162 in 2008. The variables we looked at were;
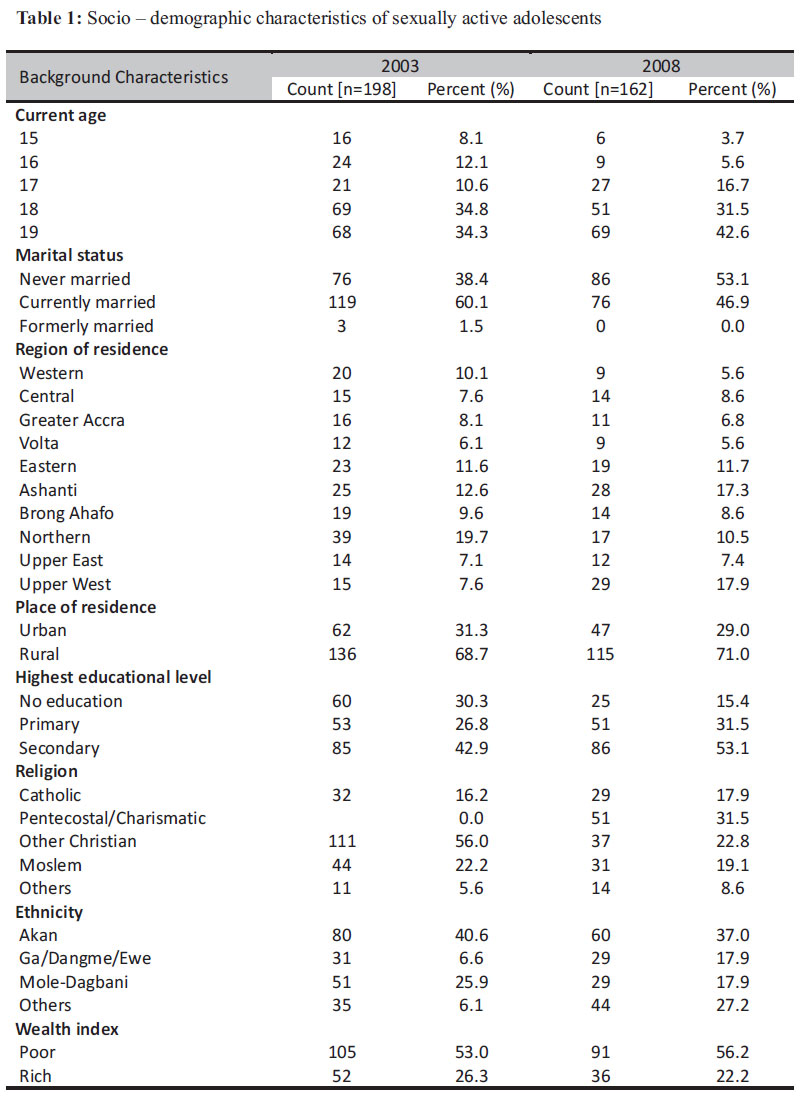
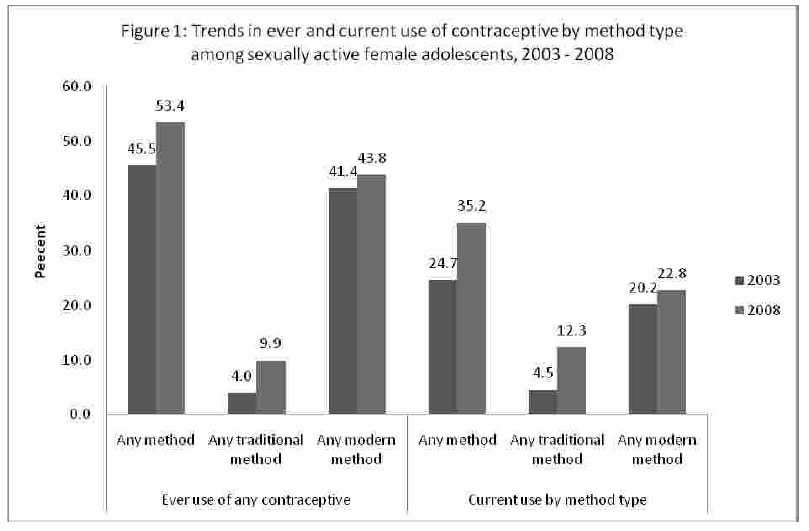
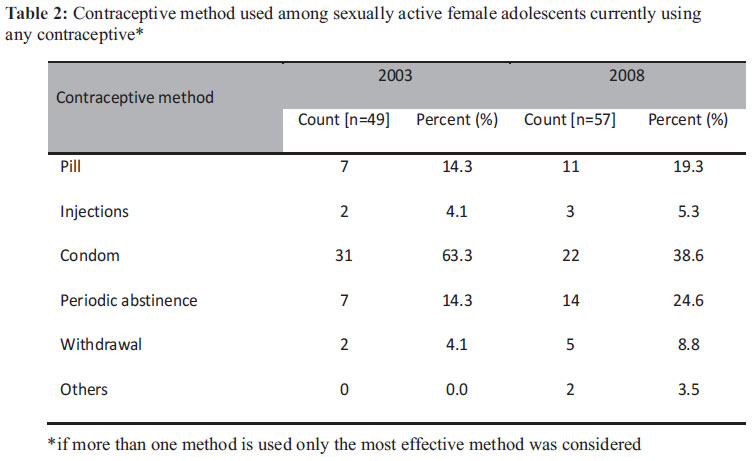
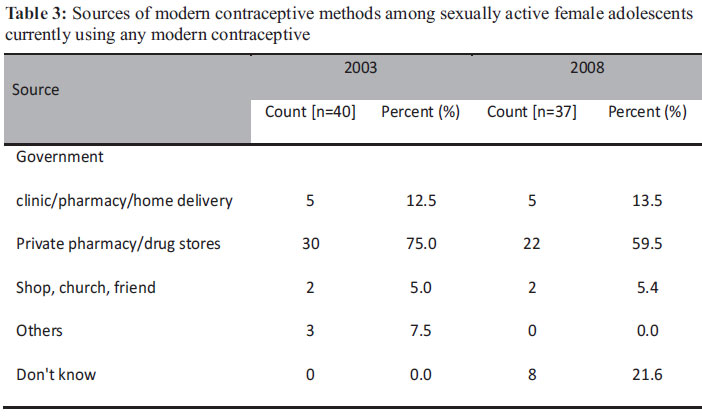
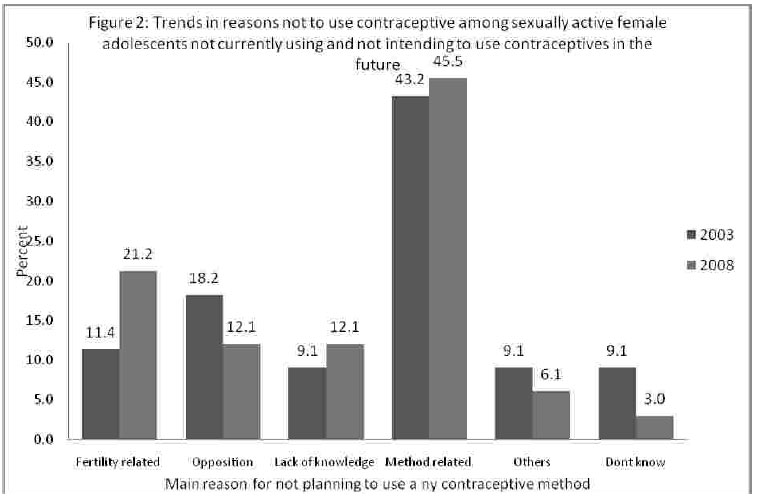
Statistical Package for the Social Sciences (SPSS) software version 18.0, (SPSS, Inc., Chicago, IL) was used to analyse the data. Mean and standard deviation were used to describe numerical variables collected and proportions and percentages for the categorical variables. Chi-square tests were used to determine significant differences in proportion between the 2003 and 2008. P-values less than 0.05 were considered to indicate significant changes. Results The study covered 198 and 162 female adolescents (15-19 years) in 2003 and 2008 respectively who were sexually active (married or unmarried). Their mean ages were 17.8 (SD± 1.3) in 2003 and 18.0 (SD ± 1.1) years in 2008. Among the 2003 subjects the majority (60.1%) were married, 38.6% had never been married and 1.5% had formerly been married. For the 2008 subjects 53.1% had never been married and 46.9% were currently married. The majority of the girls (about 70%) from both surveys were from rural areas and educated up to the secondary school level. More than 50% of the respondents from both surveys were from poor households (table 1). The Northern region (19.7%) and Upper West (17.9%) were the regions most represented in 2003 and 2008 respectively. The Akans and Moledagombas were the main ethnic groups represented in the sample for both surveys. Figure 1 shows the changes in contraceptive use between the two demographic and health survey (DHS) measured by ever use and current use, by contraceptive method. Between the two DHS the sexually active female adolescents who had ever used contraceptives increased by about 14.5% (45.5% in 2003 and 53.4 in 2008). Among those who had ever used contraceptives, traditional methods had increased between 2003 and 2008 by 59.6% (from 4.0 to 9.9%). Modern methods had also increased in the same period but only by 5.5% (from 41.4 to 43.8%). Current use of any contraceptives increased significantly from about one in four sexually active adolescent girls in 2003 to one in three in 2008 (p=0.03). Current use of any modern and any traditional method increased by 2.6 and 7.8 percentage points respectively. Among those currently using a contraceptive the most frequently used methods for both surveys were condoms, pills and periodic abstinence (rhythm method) (table 2). Whilst the use of condoms decreased significantly by 64% between 2003 and 2008 (63.3% to 38.6, p = 0.011), the use of all other methods increased. Periodic abstinence had the highest increase of about 10 percentage points (14.3% in 2003 to 24.6% in 2008) and injections the lowest (1.2 percentage points ) (4.1% to 5.3%). In 2003 about 41% of the adolescents who were not currently using any modern contraceptive knew where to get it. They mentioned stores and the market as a place where they could get modern contraceptives. Among the 2008 adolescents who were not using any modern contraceptive none of them knew any source of such methods. As shown in table 3 the main sources of modern contraceptives for adolescents currently using any modern contraceptive method were private pharmacies/drug stores (75% in 2003 and 59.5% in 2008) and government clinics/pharmacies/home delivery (12.5% and 13.5% in 2003 and 2008 respectively). About 5% from both surveys obtained modern contraceptive from their friends or from the Church. Among the sexually active adolescents, all respondents who were not currently using a contraceptive method (149 in 2003 and 105 in 2008) were asked of their intention to use a contraceptive in the future. In both surveys the majority indicated that they intended to use contraceptives in the future (66.4% in 2003 vs 62% in 2008). About 4% and 7% in 2003 and 2008 respectively were either not sure of whether or when they will use contraceptives. Almost one third of the female adolescents not currently using any contraceptive method indicated they had no intention of using contraceptives in the future. This did not change between the two surveys (table not shown). The adolescents who did not intend to use contraceptives in the future were asked why they did not intend to use it. The reasons were categorized into those related to fertility, to lack of knowledge, to the contraceptive method, to opposition by the respondent (e.g. due to religious views forbidding use of contraceptives) and/or by others (such as husband or other family members) (results are shown in figure 2). In both surveys the main concern for not intending to use contraceptives was related to the method (43% in 2003 vs 46% in 2008). These concerns included issues related to fear of side effect, “interference of the contraceptive with normal body function” and inconvenience of using contraceptive methods. Fertility related reasons accounted for about 11% and 21% of the reasons for not intending to use contraceptives in 2003 and 2008 respectively. These reasons were related to having infrequent sexual intercourse and the need for more children. Religion, husbands' and respondents' own opposition in addition to opposition by others make up 18 and 12% of the reason for not intending to use contraceptives in 2003 and 2008 respectively. Generally there was an increase in all the categories of reasons for not intending to use contraceptives in the future, except opposition to using these methods. Discussion The sample sizes of 198 for 2003 and 162 in 2008 are quite small. This is because the DHS is not specifically designed to study sexual activity and contraception among adolescent. The sample can however still be considered to be representative of sexually active adolescents in Ghana considering the robust statistically methods employed in the selection of the respondents for the GDHS. The finding of this study should be interpreted in the context of Ghana though it can provide some insight into contraception among sexually active adolescents in Africa as a whole. The observed increase in ever and current use of any contraceptive can be considered to be substantial though much still needs to be done. Other countries such as Benin and Nigeria recorded only 2.8% and 1.7% increase over a ten year period14 , that is less than 1% average annual increase in current contraceptives use. Cleland and Ali have argued that a 1.4% annual increase in condom use among young females is a modest success considering that acceptance of contraception needs considerable adjustment in behaviour15. Comparing our finding to those of Agyei et al who reported that in 1996 only 26% of sexually active adolescents' females were using any contraceptive16 , it can be deduced that the trends in contraceptive use among adolescent females in Ghana have been on the increase in the past one and half decades. According to Biddlecom et al about 21% of sexually active adolescents' females (12-19 year olds) in Ghana have ever used any traditional method of contraception17. Figures for the current study are much lower (4% in 2003 and 10% in 2008). This difference in the results of the two studies might be due to the different definitions of “sexually active” adopted by both studies. The current study defined being sexually active as having had sex within the four weeks before the survey whilst Biddlecom et al defined it as sex in the last 12 months preceding their survey. Much of current increase is nevertheless due to the increase in usage of traditional contraceptive methods. This situation presents a double issue that would need to be addressed. On one hand it is an indication that adolescents are willing to use some form of contraception to avoid getting pregnant, which is a positive sign. On the other hand adolescents using traditional methods are at risk of sexually transmitted infections and unwanted pregnancies since these methods are highly unreliable. Apter et al have even noted that the irregular nature of the menstrual cycle of adolescents increases the unreliability of traditional methods such as the rhythm method18. Hence in programming for adolescent SRH much emphasis should be placed in encouraging them to use a modern method. Cost of modern contraceptives though subsidized could still be beyond the reach of many adolescents. In 2008 Lunginaah observed that the cost of a pack of three condoms in the Upper West Region of Ghana was more than the daily minimum wage19. Condoms are even cheaper than the other contraceptives. So if the adolescents cannot afford condoms, the situation for the other contraceptives will be worse. Health system factors such as attitude of health workers9; 20 and the limited availability of health facilities in rural area might further limit access to and use of modern contraceptives. Results from the current study show that for both the 2003 and 2008 surveys, only about half of the female adolescents who had ever used a modern contraceptive method were currently using it. Ann Blanc and her colleagues (2009) have noted experimentation and inconsistent use of contraceptives to be common among young woman in developing countries 15 . This observation could explain why the percentage who has ever used any contraceptive is more than those currently using it. Karim et al 21 also reported that only one in ten sexually active unmarried female youth in Ghana used condoms consistently. The reasons for this discontinuation might not be too different from that given by older women. Some of the reasons are related to the nature of the contraceptive method, misconceptions that contraceptives can cause infertility and opposition from partners. To derive the maximum benefit from contraceptive use, consistency in use is very essential. This can be achieved by improving the quality of services offered to adolescents and also educating them on all the possible side effects of any method they want to use. The current study identified condoms, periodic abstinence and pills to be the most commonly used contraceptives by the sexually active female adolescents. Similar findings have been reported from numerous studies in Ghana and other African countries, showing condoms to be the most commonly use contraceptive by both young and older women13;16;21 . Other methods such as pills, injections and period abstinence have also been found to be commonly used by adolescents in Ghana16; 22. It was not surprising that none of the respondents in the current study was using the female condom as it is difficult to use and not widely available in Ghana. Though condoms were the most widely used contraceptives, the percentage using condoms however decreased between the two surveys. As mentioned earlier cost of condoms, could account for this situation. Additionally the “abstinence only” campaign of President Bush led to key Nongovernmental organisations (such as the Planned Parenthood Association of Ghana – PPAG), which were providing condoms to adolescents, losing their funding from USAID and hence had to stop the provision of condoms to adolescents. Contrary to the findings of Cleland and Ali15 the current study found that the increase in the use of traditional methods between 2003 and 2008 was higher than that for modern methods though the percentage using modern methods was still higher. This, as discussed earlier might be an indication of the lack of access to modern contraception or misconceptions about its side-effects. As a male controlled contraception the high prevalence of condom use among the young girls gives cause for some concern. Considering the power and gender inequalities in sexual relationships in Ghana, how will the young girls negotiate for condom use when their partners are not interested in using it? Making a request to a partner to use condom is even more difficult as it may be interpreted as of lack of trust in the partner. The vigorous social marketing campaigns carried out to promote contraceptive use are disproportionately promoting condoms as compared to other methods23. Condoms are easy to use and it takes a very short time to teach a person how to use them and highly skilled staff is not required to do this. This has made it easy to distribute condoms almost everywhere as compared to other contraceptive such as injection and to some extent pills which needs more time and skilled health workers to administer. The high prevalence of condom use may also possibly be due to its increased use among single women15. Higher rate of condom use compared to other contraceptives is advantageous as condoms are the only contraceptives that provide dual protection form pregnancy and STIs including HIV. Unfortunately adolescents in Ghana use condoms because of the fear of getting pregnant, not to prevent STIs22. It has however been suggested by Mayhew and Adjei that the risk of dying from unwanted pregnancy through abortion might even be higher than from HIV for young girls in Ghana24. Knowledge of the sources of contraceptives for adolescents would help in the design of programmes to make contraceptives accessible to adolescents through various outlets. A study by Biddlecom et al in Ghana, Malawi, Burkina Faso and Uganda indicated that the most sexually active adolescents do not use contraceptives because they do not know where to obtain them17. Similar findings were made in the current study. For example among the 2008 subjects who were not currently using any contraceptive no one knew any source of contraceptives. The findings of this study are comparable to other studies conducted in Ghana8; 13; 22 . The current study identified private pharmacies and drug stores as the major sources for adolescents to obtain contraceptives. This is similar to results from other African countries. In an analysis of DHS data from 18 Sub-Saharan African countries John Cleland and Mohammed Ali found that in 15 out of the 18 countries more than 70% of the young female adolescents who used condoms bought it from private distributors (pharmacies and drug store)15. It reflects the inability of governments all over Africa to make contraceptives accessible to adolescents. In a study in Ghana, 62% of the female adolescents indicated they would prefer to get contraceptives from government clinics and hospitals as compared to 16% who preferred drug store and private pharmacies [22]. Contrary to this finding, the current study found that about 20% of the 2008 subjects did not know the source of the contraceptive though they reported using one during their last intercourse. Their partners might have been the ones who obtained the contraceptive, hence their lack of knowledge of its source. The reasons why some respondents were not planning to use contraceptives in the future were not different from those found by Agyei and his colleagues16. The major reasons were related to the health concerns and side effects respondent thought would result from contraceptive use, the desire for more children and those linked to opposition from their partners or religious prohibition. The reasons given for not intending to use contraceptives reflect a lot of misconceptions about modern contraceptives among the adolescents. This is probably because their concerns about contraceptives are not being addressed well by service providers23. It might also mean that the reported high knowledge of contraceptive among adolescents22 is not detailed knowledge but just 7. recognition of the existence of specific contraceptives. In conclusion, the findings of this study indicate that though sexually active female adolescents are willing to use contraceptives, factors such as physical access, cost and misconceptions about their effects limits their access and use. Future ASRH programmes in the country would have to address these factors, focusing on information and education not just on contraceptives but also on the potential side effects and how to deal with them. It should also focus on increasing access to modern contraceptives by addressing the problem of cost and physical access especially in rural areas. On the whole if the current contraceptive use among sexually active adolescent girls is not improved, then the country is likely not to meet the objectives of the national adolescent reproductive health policy, and the Millennium Development Goal of achieving universal sexual and reproductive health. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11019f1.jpg] [rh11019t3.jpg] [rh11019t1.jpg] [rh11019f2.jpg] [rh11019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}