 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
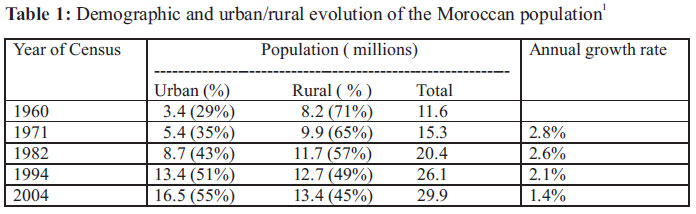
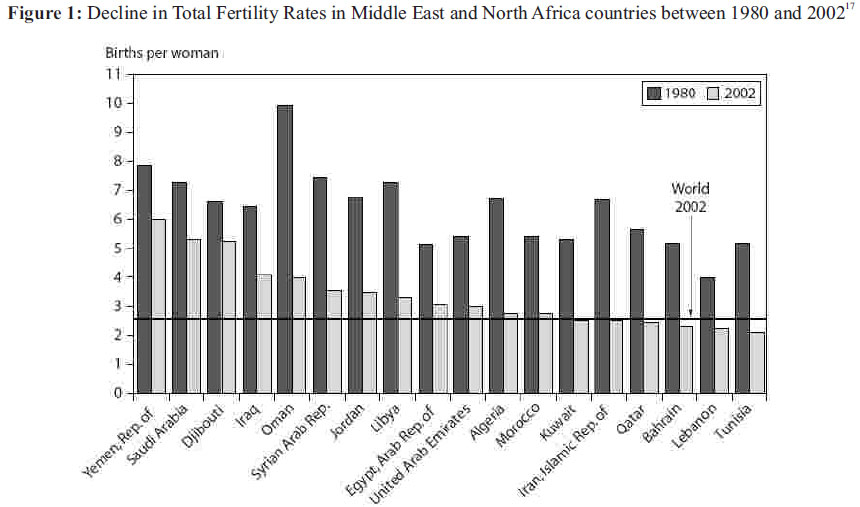
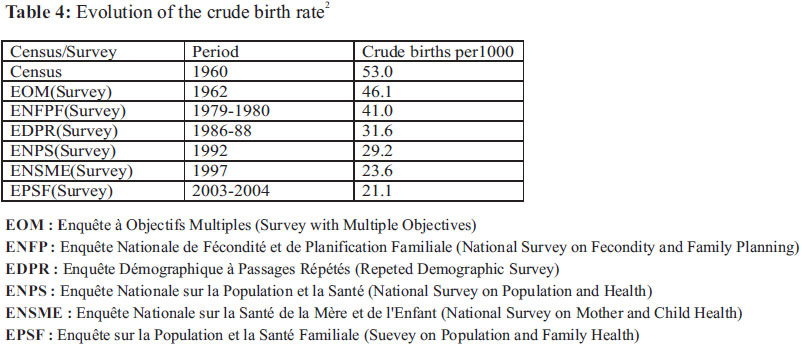
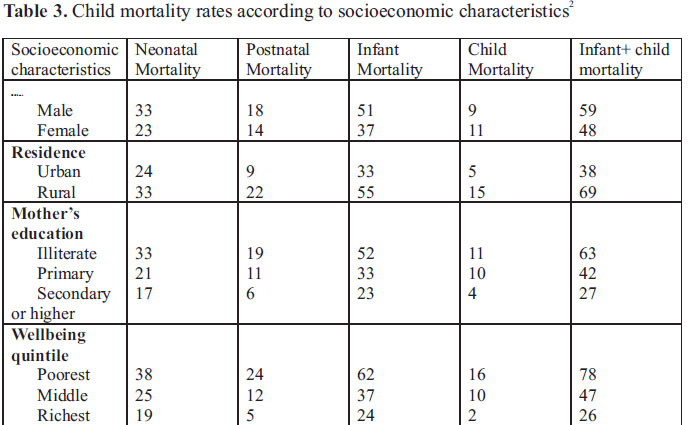
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 57-66 ORIGINAL RESEARCH ARTICLES Social Determinants of Reproductive Health in Morocco Boutayeb Abdesslam LaMSD, Faculty of Sciences, University Mohamed Ier, Oujda, Morocco, Unité Associée au CNRST URAC04 E-mails: x.boutayeb@menara.ma, masraab@brunel.ac.uk Code Number: rh11020 Abstract Moroccan population has known a growing demographic trend. However, beyond the global tendency, reproductive health remains characterised by inequalities and disparities between urban and rural, rich and poor, developed and deprived regions.In this study, we relied mainly on data and statistics provided by the last five censuses, the four Demographic Health Surveys, Multiple Indicator Cluster Surveys, reports of international bodies and publications dealing mainly with health and development in the Arab World. During the last decades, fertility declined due to different parameters. Infant mortality decreased and should reach the corresponding Millennium Development Goal whereas maternal mortality has stayed nearly constant. The achievements accomplished in reproductive health remain insufficient. Family planning and contraception policies need to reach more women; and antenatal and postnatal care should be enhanced especially towards poor women living in rural areas and deprived regions. Résumé La population marocaine a connu une croissance démographique soutenue. Cependant, au-delà de la tendance globale, la santé reproductive demeure caractérisée par des inégalités et disparités entre urbain - rural, riche - pauvre, régions développées- régions sous développées. Dans cette étude, nous nous sommes basés sur les données et statistiques fournies par les recensements, les Enquêtes de Santé et Démographie, les Enquêtes à Indicateurs Multiples, les rapports des organismes internationaux et les publications traitant essentiellement des thèmes de santé et développement. Durant les dernières décennies, la fertilité a baissé pour différentes raisons, la mortalité infantile a diminué et devrait atteindre les Objectifs du Millénaire pour le Développement mais la mortalité maternelle est restée presque constante. Les efforts accomplis en matière de santé reproductive demeurent insuffisants. La politique de planification familiale et de contraception doit toucher plus de femmes, les soins prénatals et postnatals devraient augmenter pour atteindre le maximum de femmes et plus particulièrement celles vivant dans les zones rurales difficilement accessibles. Key words: Reproductive health, social determinants, inequity, regional disparities Background Morocco is a low-middle income country situated in North Africa with coasts on the Atlantic Ocean and the Mediterranean Sea. The Moroccan population has known a growing trend, passing from less than 12 million in 1960 to 30 million in 2005 (Table 1)1 . The rates of total fertility, crude birth, crude death and infant mortality have been decreasing during the last three decades2. Accordingly, the age structure is changing and the country is experiencing a transition on different levels (demographic, geographic, economic, political, and epidemiological). As stressed by the Worl Bank “in spite of the progress made in reducing income poverty, social indicators in Morocco are well below those of comparable countries and, within the country, there are enormous disparities in access to social services between urban and rural areas”3. Method In this paper, we relied mainly on data and statistics provided by the last five censuses (1960, 1971, 1982, 1994, 2004)1 , the four Demographic Health Surveys (1987, 1992, 1995, 2003-2004)2 , reports released by international organisms such as the World Bank3, World Health Organization (WHO)4-6, the United Nations Development Programme (UNDP)7, UNICEF8 and other publications dealing principally with health and development in the Arab World. Results and Discussion Demographic trends During the last four decades, the Moroccan population has known nearly a threefold increase, from 11.6 million in 1960 to 29.9 million in 2004. However, the annual growth decreased from 2.8% between 1960 and 1971 to 1.4% between 1994 and 2004. The urban/ rural repartition has also known an important evolution, shifting from a rural (70%) dominance in 1960 to an urban (55%) dominance in 20041 (Table 1). According to the last census in 2004, the Moroccan population is young, with 38% under the age of 15 years and 21% between 15 and 24 years. Table 2 shows that the country is undergoing a demographic transition leading to a new age structure with less people in the youngest class (0-14) and an increasing size of the elderly class (60+). During the next decades, the situation will be challenging for policy makers who will have to deal with the needs of young people in terms of education, health and employment; and to provide welfare and social care for the growing class of elderly people. Fertility and mortality are the main determinants of the age structure evolution, whereas the shift from rural to urban dominance is caused by socio economic parameters such as access to employment, social services, health and education facilities, etc... Reproductive trends and health indicators Life expectancy at birth has increased from 65 years in 1980 to 70.4 years in 2005 whereas the annual population growth rate decreased from 2.6 in the 1980s to 1.3 in 2005. These outputs are results of a decreasing trend in fertility, crude birth, crude death and infant mortality. Indeed, global total fertility (average number of children who would be born to a woman if she were to live to the end of her childbearing years) has decreased from nearly 6 children in 1980 to 2.5 children in 2005 independently of differences urban/ rural and poor/rich women (See Figure 1 for comparison with other countries). The fertility decline is mainly attributable to factors such as the use of contraception and the delayed age of marriage. For instance, between 1980 and 2004, the percentage of married women using contraception increased from 19% to 63% ; and during the same period, the proportion of married women aged 15-19 (respectively 19-24) declined from 21% to 11% (respectively from 64% to 36%)2. However, these factors are interrelated with cultural and socioeconomic factors such as the access of young girls to higher education, unemployment, unaffordable expenses of marriage for men (dowry, ceremony, festivity) and high cost of child bringing up. Culturally, more and more girls are having access to higher education and young women are getting jobs with responsibility. Consequently, the age of marriage is delayed and women are opting for fewer pregnancies. Economically, many young men are deterred from marriage because of it's direct and indirect expenses (dowry, festivity, appropriate housing, etc…). Then for young couples who succeed in getting married, the high cost of a decent living standard (food, housing, education, health, transport, leisure, etc…) becomes a real determinant of the number of children wanted. This tendency is found particularly among people with unsecured income (unemployed, part time workers, farmers with non irrigated land), educated couples and those of the middle class. The previous factors have also affected the crude birth rate which decreased from 5.3% in 1960 to 2.1% in 2004 (Table 4). Whereas, the crude death rate has seen a similar decrease from 0.95% in 1960 to 0.63% in 2004, due mainly to a general improvement of health conditions (vaccination, food and diet enhanced with micronutrients, hygiene, eradication and control of communicable diseases). Infant mortality rate decreased from 140 per 1000 births in 1980 to 37 in 2005. As indicated in Table 3, social status is a major determining factor of survival for Moroccan children. Illustration is particularly given by post-natal mortality which is mainly due to factors such as food, primary health care and hygiene. It is striking to see that for postnatal mortality:
Maternal mortality ratio (MMR) decreased from 332 per 100 000 in 1980 to 228 in 1990 but since then it has remained nearly constant, indicating, in particular, that the goal fixed by the Millennium Development Goal(MDG5) to “reduce by three quarters the MMR between 1990 and 2015” and “achieve universal access to reproductive health” is difficult to realize. As indicated by a WHO review on social determinants of health in seven Mediterranean countries, the main reasons why MMR remained quasi constant in Morocco during nearly two decades can be summarised as follows9:
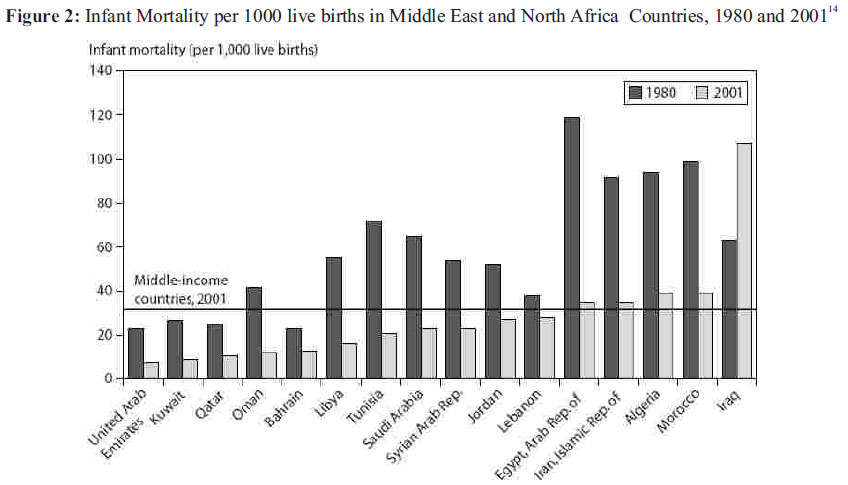
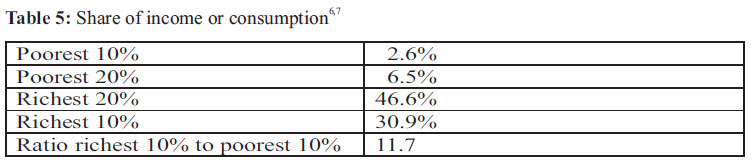
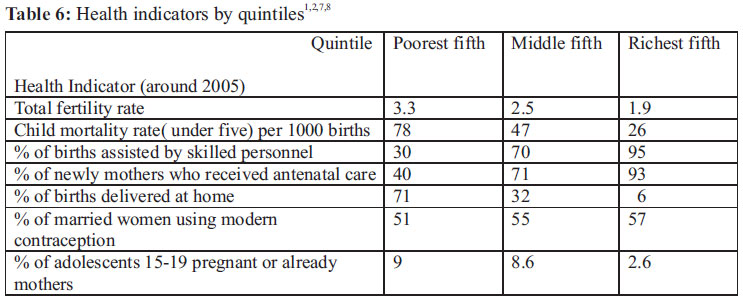
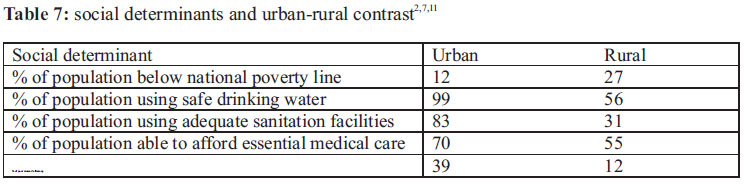
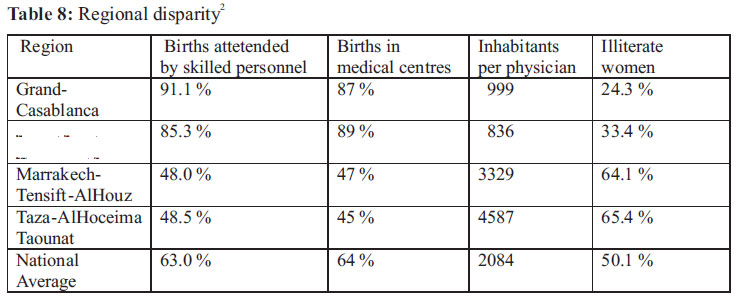
More efforts are needed to improve health indicators associated with women's reproductive health and maternal mortality, namely: MMR, proportion of births assisted by skilled medical personnel, antenatal care visits, adolescent birth rate, contraceptive prevalence and unmet need for family planning. Reproductive health and social determinants. As stressed by the WHO Commission on Social Determinants of Health in its report “Closing the gap in a generation”6 , health is influenced by the socioeconomic conditions in which people are born, grow, live, work, reproduce and age. In particular, reproductive health is quantitatively and qualitatively determined by conditions such as poverty, income, employment, food security, housing, education, discrimination, and the women status in general. In a previous paper dedicated to human development and health indicators in the Arab region, we carried out a data analysis on life expectancy at birth, infant mortality, maternal mortality, expectation of lost healthy years, deliveries attended by skilled attendants, pregnant women receiving prenatal care, number of inhabitants per physician, percentage of children under weight and data related indirectly to health such as percentages of literacy and enrollment. It was seen that very few Arab countries do globally worse than Morocco12. In another study devoted to infant mortality in 16 Arab countries, sociodemographic, perinatal and economic factors were considered, showing that Egypt, Morocco, Sudan, Yemen and Iraq were classified in the group with the highest infant mortality rate 13. Figure 2 shows how Morocco compares with other countries in terms of infant mortality and its reduction between 1980 and 2001. Despite a substantial improvement in health indicators globally during the last decades, the Moroccan administration has embarked on the third millennium under the burden of inequity and large disparities between rich and poor, urban and rural, and developed regions opposed to deprived ones. Rich-poor: The country is characterised by huge inequalities in terms of income and consumption. The richest 20 % of the population absorb nearly 50% of income and consumption yielding an 11.7 ratio between the richest 10% and the poorest 10% of the population7 (Table 5). In terms of reproductive health and its determinants, the gap between rich and poor is illustrated by a multitude of health indicators such as the number of antenatal care visits, use of modern contraception, births attended by skilled medical personnel, adolescents pregnant or already mothers, infant mortality and others 2,8,12,14 ( Table 6). Rural-urban During more than 50 years of independence, Moroccan policy makers have given little attention to the rural world. Consequently, by the beginning of the third millennium, only 56% of rural populations have access to safe drinking water, 31% have access to adequate sanitation and more than 40% are unable to afford essential medical care. A dramatic urban-rural contrast is seen in access to education, housing, drinking water, sanitation, economic opportunities and social services in general (Table 7). Given the fact that nearly half of the Moroccan population lives in under-served rural areas, the consequences on reproductive health are obviously negative. Regional disparities: Sixty years ago, the country's regions used to be classified into two classes: “useful regions” and “non useful regions”. By the dawn of the third millennium, one can still state that “Morocco is a country of contrasts and dualistic development where debilitating urban and rural poverty coexists alongside modern urban centres”15. Indeed, as illustrated in Table 8, exorbitant disparities exist between regions in access to basic services such as education and health. A woman living in the deprived region is twice unlikely to give birth in a medical centre or to be assisted by skilled medical personnel than a woman living in a developed region. Similarly, the ratios of illiterate women and the number of inhabitants per physician are nearly 3:1 and 5:1 respectively. Women status In developing countries, it is often stressed that economic development will remain disabled unless women status is enhanced to allow them to fully participate economically, politically and socially side by side with men. According to the author of a study in Islamic and Arabic countries16 , the low social and economic status of girls and women is a fundamental determinant of maternal mortality and reproductive health in many Islamic and Arab countries. Aware of the importance of women empowerment, the Moroccan parliament adopted in 2004 a new family code (Moudawana). Hoping to enhance the woman status, the reform stipulates amongst other the following women rights:
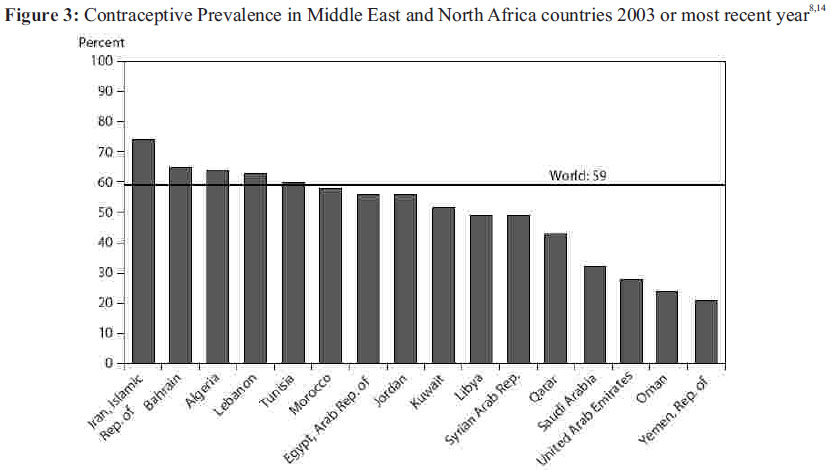
Family planning Noticeable results were achieved by the Moroccan family planning program launched in the early 1960s, followed by the legalisation of contraception in the same period. Indeed, the percentage of women using any contraceptive method increased from 19% in 1980 to 42% in 1992 to reach 63% in 2003. According to the last national survey carried out in 2003/2004, 54.8% of women used a modern contraceptive method and 8.2% used traditional contraceptive methods (periodic abstinence, withdrawal, plants,..). Among modern methods, pills are the most used (40.1%), followed by IUD (5.4%), MAM (2.8%), female sterilisation (2.7%), injections (2.1%), condom (1.5%) and jelly (0.1%). The use of any contraceptive method varies slightly among the different social groups. For instance, modern methods are used by 56% of urban women, compared to 53.2% of rural women; and also used by 53.7% of illiterate women compared to 56.4% of use among women with secondary or higher level of education. The association with wellbeing quintiles shows a modern contraceptive prevalence of 58.3% amongst the poorest women compared to 69.9% in the richest quintile. In 2003, about 10% of women aged 15-49 years had unmet need and the association with the different social categories was not very high (11% for illiterate women compared with 8% for women with secondary or higher level of education; 11% for rural women versus 8% for urban women, and 12% for the poorest women compared with 8% for the richest women). Feed-back studies indicate the possibility to improve the efficiency of these services, which are available through vertical programs, by more integrated and comprehensive ones. There is still room for quantitative and qualitative improvements in terms of percentage of women using contraception (63%) (Figure 3), diversification of contraceptive methods and reduction of unplanned pregnancies especially among young women who are behind the estimated 150 000 illegal abortions performed annually. In morocco the abortion is performed in a legal way only for three reasons: mother's health problems, foetal abnormalities, rape or incest. However, women resort to abortion in other cases like: not being able to afford and bring up a baby, having problems with the partner, constraints of education or work, unwanted pregnancy. The problem of abortion becomes a striking and dangerous phenomenon especially when teenage girls and/or young poor women are not able to pay for ''illegal assisted'' abortion by doctors and hence resort to traditional and dangerous practices with unpredictable results that may lead to death. According to the Moroccan Association to combat Clandestine Abortion (AMLAC), despite the ban, between 600 and 800 abortions are carried out every day with medical care in Morocco while 200 others take place on the back streets. Conclusion During the last decades, Morocco has globally made noticeable achievements in terms of reproductive health. The achievements, however, remain insufficient compared to other developing countries with similar level of economic development18, 19 . While, due to immunisation efforts, infant mortality has been decreasing during the last four decades and should reach the corresponding Millennium Development Goal (MDG4), the MDG5 seems difficult to realize since maternal mortality has stayed nearly constant during the last 15 years. As stipulated by the 2008 report released by the Wold Health Organisation4, now more than ever, an efficient primary health care is needed if countries like Morocco are to reach the goal of health for all. Family planning and contraception policies need to reach more women; antenatal and postnatal care should be enhanced, and more skilled medical personnel are needed to assist women during labour, especially for poor women living in rural areas and deprived regions. Generally, reproductive health in Morocco can be improved by adopting targeted and equitable health strategies that aim to enhance the mean status of the whole population but at the same time to reduce regional disparities between developed and disadvantaged regions; inequalities between rich and poor, and marginalisation of the rural population. For a real sustainable development and in the light of the general uprising affecting most of Arab countries, Moroccan decision makers are urged to act on unjustifiable and avoidable inequalities. Limitations of our research The present paper is based on available data related to reproductive health in Morocco. It should be stressed, however, that sometimes data may vary from one source to another. For instance, a higher level of maternal mortality rate (140 per 100 000 in 2005) was given by the estimation provided jointly by WHO, UNICEF, UNFPA, and the World Bank5. Acknowledgements: This paper is an improved version of a poster presented at the XXVI IUSSP International Population Conference held Sep 27-Oct 2, 2009 in Marrakech, Morocco. Improvement was undertaken during a visit to CRPH at the Faculty of Health Sciences of the American University of Beirut which was funded by the Wellcome Trust. Dedication: This humble contribution is dedicated to Moroccan women living in rural areas. Competing interest: The author declares that he has no competing interests. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11020f1.jpg] [rh11020t6.jpg] [rh11020t4.jpg] [rh11020t2.jpg] [rh11020f2.jpg] [rh11020t5.jpg] [rh11020t3.jpg] [rh11020t8.jpg] [rh11020t1.jpg] [rh11020t7.jpg] [rh11020f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}