 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
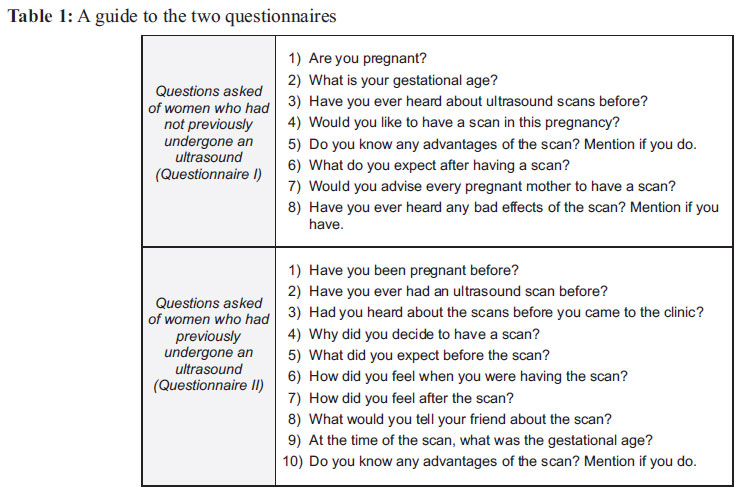
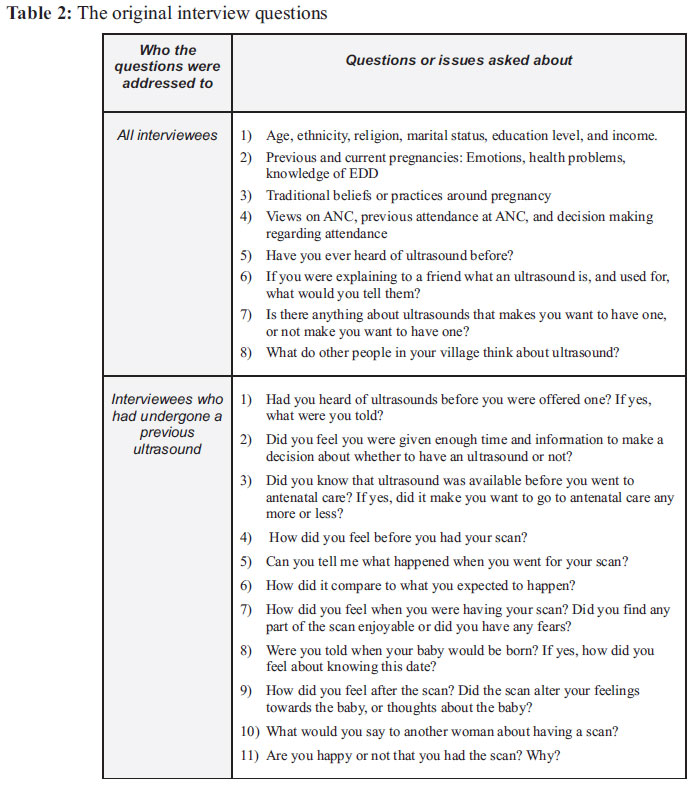
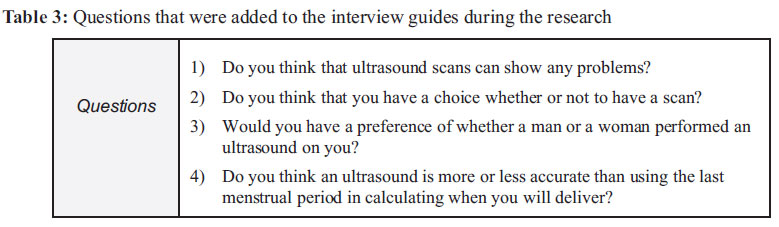
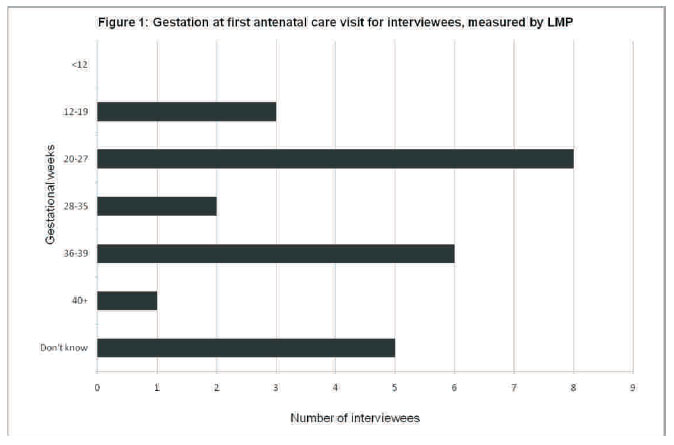
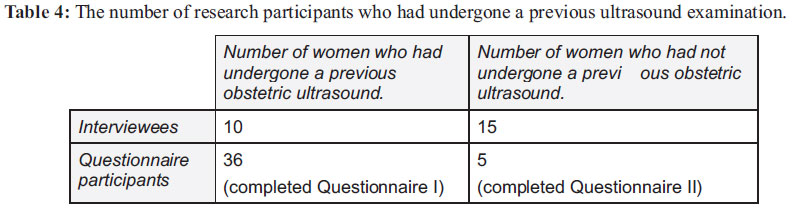
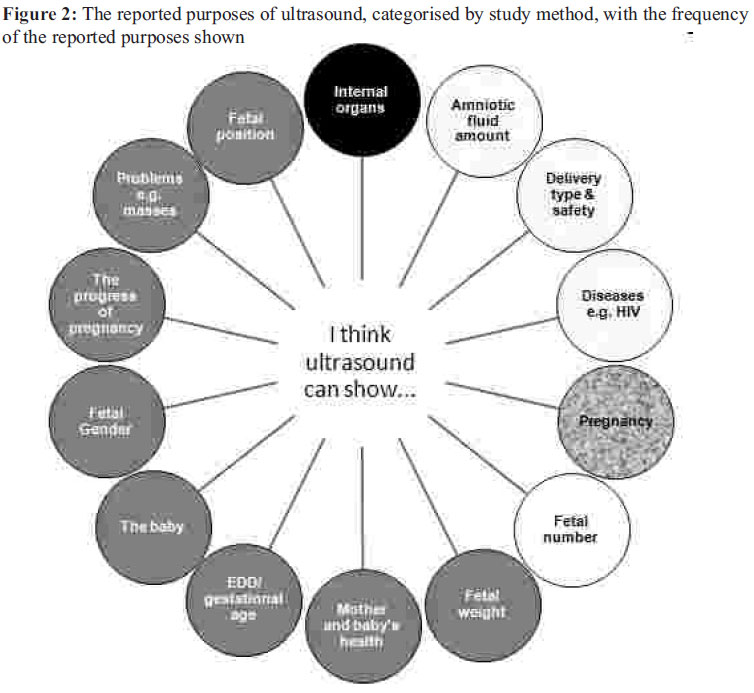
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 91-108 ORIGINAL RESEARCH ARTICLES Pregnant women's beliefs, expectations and experiences of antenatal ultrasound in Northern Tanzania Emma Rebecca Firtha , Pendo Mlayb , Richard Walkerc , Peter Richard Silld . a School of Medicine, Sheffield University, UK; b Department of Obstetrics & Gynaecology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania; c Department of Medicine, North Tyneside General Hospital, North Shields, UK; d Department of Obstetrics & Gynaecology, Wansbeck Hospital, Northumberland, UK. *For correspondence: E-mail: em_firth@hotmail.com Code Number: rh11023 Abstract This qualitative study explored pregnant women's beliefs, expectations and experiences of the recently introduced antenatal ultrasound service in BomaNg'ombe hospital, Tanzania. Thematic analysis of 25 semi-structured interviews and 41 questionnaires was employed. The majority of women desired ultrasonography despite many not understanding the procedure or purpose. Patient's expectations included discovering fetal position, fetal sex and pregnancy problems. However, women frequently over-estimated the capacity of ultrasound, and had significant fears of harm. One sixth of questionnaire respondents said they did not want ultrasonography. Nonetheless since the service was introduced no woman has declined, and numerous interviewees believed scans were obligatory. Despite fears, some women reported enjoyment of ultrasound. Interviewees believed ultrasound would increase antenatal care (ANC) attendance. An informed consent policy and an education campaign are needed to reduce fears and maximise uptake and health gains. The effects of ultrasound availability on timely ANC uptake, including amongst women not currently accessing ANC, should be further researched. Résumé Cette étude qualitative a exploré les croyances, les attentes et les expériences des femmes enceintes par rapport aux services de l'ultrason prénatal qui ont été nouvellement introduits dans l'hôpital BomaNg'ombe, en Tanzanie. Nous avons employé l'analyse thématique de 25 interviews semi-structurées et 41 questionnaires. La plupart des femmes avaient besoin de l'ultrasonographie malgré le fait que beaucoup d'entre elles ne comprenaient pas la procédure ou l'intention. Les attentes des patientes comprenaient la découverte de la position fœtale, le genre fœtal et les problèmes de la grossesse. Pourtant, les femmes ont souvent surestimé la capacité de l'ultrason et elles avaient beaucoup du mal. Une sixième des interviewées à travers les questionnaires ont déclaré qu'elles ne voulaient pas l'ultrasonographie. Néanmoins, depuis que le service a été mis en place, aucune femme n'a refusé et plusieurs interviewées ont cru que les écogrammes étaient obligatoires. Malgré les craintes, quelques femmes ont déclaré qu'elles aiment l'ultrason. Les interviewées ont cru que l'ultrason va augmenter la fréquentation aux services prénatals (FSP). Une politique du consentement éclairé et une campagne éducative sont nécessaires pour réduire les craintes et pour tirer au maximum la captation et les rapports de la santé. Il faut approfondir des études sur les effets de la disponibilité sur la captation opportun de la FSP, y compris chez les femmes qui ne profitent pas actuellement de la FSP. Key words: Fetal ultrasound, obstetric ultrasound, beliefs, expectations, experiences, Tanzania Introduction Many women in Northern Tanzania present with problems late in pregnancy without a record of gestational age and estimated date of delivery (EDD). Knowing an EDD aids delivery management and preprocedural planning, and reduces pre- and post-term births1 and labour inductions 2,3. Obstetricians report that a lack of an accurate EDD and late referral of women with complications are two key causes of obstetric mortality in Kilimanjaro Christian Medical Centre (KCMC), a large referral hospital in the Moshi District, Northern Tanzania. Date of last menstrual period (LMP) and physical examinations have traditionally been used to estimate gestational age. However, antenatal ultrasound is now recognised as the most accurate method4,5. Whilst antenatal ultrasound is widely established in the developed world6,7, it is a recent introduction in many developing countries such as Tanzania. Due to a shortage of ultrasound machines and trained sonographers in the country, antenatal ultrasound is only usually available at certain private and tertiary hospitals in Tanzania. To increase access to ultrasound, in 2004 Northumbria Healthcare NHS Foundation Trust provided ultrasound machines and sonography training, initially at KCMC, and subsequently at BomaNg'ombe District hospital where an ultrasound service was introduced in 2009. Around 144 women had undergone a routine ultrasound as part of the pilot service by the start of this study. Whilst this project offers great promise for improving clinical outcomes, it is agreed that new technology and interventions should be introduced cautiously in resource-poor settings8 . Indeed, the United Nations' appraisal framework for the introduction of new technology includes the 'appropriateness' of the new intervention as one of six key considerations9. International research into the cultural acceptability of antenatal ultrasound remains largely Euro-American and Australian. There is a paucity of research into the beliefs, understanding and experiences of antenatal ultrasound in developing countries, where ultrasound technology is often a relatively new concept. Specifically, only Nigerian10-13 and Botswanan14 studies represent the views and experiences of pregnant African women. To date, no studies report women's prior knowledge of, or opinions or beliefs about ultrasound in Tanzania. Tanzania has rich tribal diversity, and witchcraft and spirits are thought to be associated with pregnancy, infertility, and abortions in some regions15-17. Belief systems can affect health-seeking behaviour and service uptake18 , and cultural beliefs may specifically affect ultrasound acceptability, so setting-specific research is essential. Research into women's knowledge and attitudes towards ultrasound services is especially important given that previous studies have documented significant psychological harm from antenatal ultrasound7,14,19, as well as positive psychological effects6,7,14. This is especially common in areas where an ultrasound service has been newly introduced. For example, when antenatal ultrasound was introduced in Botswana, some women feared they were going to die, fears which staff were unaware of14. This highlights the importance of direct reports from women when investigating the beliefs and experiences of women regarding ultrasound scans. Although most women (94%) in Tanzania achieve at least one ANC visit during their pregnancy20 only 62% make the four visits recommended during pregnancy. Moreover, 80% of women make their first visit late (after 16 weeks) with one-third of women seeking no ANC until six months has passed21 which is too late for accurate ultrasound calculation of EDD3,4. Maternal mortality in Tanzania is estimated at 950 deaths per 100,000 births20 , double that of the average maternal mortality rates for developing countries22. In this context, timely uptake of ultrasound and of ANC, are each potentially life-saving. Moreover, ultrasound examinations may have the power to positively or negatively affect the timely attendance at ANC. Understanding the views of pregnant women towards ultrasound scans is therefore of crucial importance. Methods 25 semi-structured interviews and 41 questionnaires were completed during May and June 2010, with pregnant women aged 18 years and over attending BomaNg'ombe antenatal clinic. Ethical approval was provided by Leeds University, KCMC ethical committee and the Hai District Medical Officer. The research took place between 19th May and 3rd June. Two questionnaires were created: Questionnaire I (completed n=36) for women who had not previously undergone an ultrasound examination and Questionnaire II (completed n=5) for women who had experienced a previous ultrasound examination. See Table 1 for a guide to the questionnaire. Questionnaires were offered to all patients at the antenatal clinic reception by nurses during the research period. Questionnaires stated that if an individual completed a questionnaire this acted as consent for participating in this study. All responses were anonymous. For translation and interpretation between English and Swahili the original research proposal was to employ one translator/interpreter from the community, to allow consistency of interpretation and translation, and to enable women to speak freely. However, senior hospital management required instead the employment of two hospital physicians as interpreters, one of which also translated the questionnaires. All patients who attended a consultation with one of the physicians acting as interpreter during the research period were invited to be interviewed within their normal consultation. In this way, convenience sampling was employed. An information sheet was explained and offered to all patients. No patients declined to participate in this study. Informed consent for interviews was gained via signature (n=20) or thumb print (n=5). If an ultrasound scan took place during an interview (n=23), questions were asked of the participant before and after the ultrasound. Interviews were recorded via note-taking, as ethical approval was not available for audio recording. The original research proposal to interview any women who had declined ultrasound scans was not viable as no woman had declined a scan between commencement of ultrasound provision and the end of this study. See Table 2 for a guide to the original interview questions. Interview responses were analysed thematically throughout the research process. Through this continual analysis the research followed an emergent design23. This emergent design meant that as participants provided new topics that had not previously been asked about, extra questions were then added to the original interview guide and subsequent interviewees were asked about these issues. This learning and adapting the research design through an inductive approach is one of the most important characteristics of qualitative research23,24,25. See Table 3 for questions that were added. Interviews ended when no new themes emerged (n=25) in accordance with 'saturation' of the data23. The questionnaire data was then cross-analysed looking for new themes, and for repetition of themes identified through interviews. Quotations from interviews and questionnaires were selected for transparency of emerging themes and to provide a deeper understanding of participant perspectives. Simple frequencies and distributions were calculated for select questionnaire and interview data. Appraisal of methods This study was done during a pilot of routine ultrasound examinations as it seemed important to investigate beliefs, expectations and experiences prior to, or early in the establishment of, the fetal ultrasound service. Views may differ if ultrasound services become well established. Women not attending ANC and those under 18 years old are not represented in this study. Illiterate women were unable to complete the written questionnaires. Reliance on note-taking during interviews may have weakened the detail of recorded responses26 but equally may have allowed more freedom of speech. Interpreters did not consistently give verbatim translations. Bias may also have occurred, as some interviewees openly expressed the desire to give the 'right answer' rather than their own. Usually this seemed in order to please the researcher, although may also have been in order to please the physician acting as the interpreter. To improve rigor, the questionnaire translations by the physician in the study were verified by an independent non-medical translator. No significant differences in the meaning of women's responses were noted, but there were language differences. For example, translations by the physician in the study included medical terms such as 'fetus', whereas the independent translator used everyday terms such as 'baby' for seemingly equivalent words. Findings and discussion Background: belief systems and health-seeking behaviours Pregnancy and local beliefs Ultrasound can identify malformations and non-viable fetuses 2,27. In countries where abortion is legal, some women choose to terminate a pregnancy in this situation. In Tanzania abortion is illegal28 and often viewed as immoral17 ; this is an important cultural consideration when introducing ultrasound services. Beliefs in witchcraft and spirits were widespread amongst interviewees, and many expressed the view that such supernatural forces could affect pregnancy. The negative effects of witchcraft on pregnancy have also been previously noted in other Tanzanian studies15 , as well as in other African research, for example in Botswana14 , the Gambia29, and Zimbabwe30. In this study, not all pregnancy problems were attributed to spiritual powers. Equally doctors, praying and witchdoctors were stated as methods for protection and cure from pregnancy problems. It is also of note that no aspect of ultrasound scanning – the procedure, the mechanism, or results – was linked to witchcraft by any interviewee. This trust in modern medicine alongside religion and witchcraft suggests 'medical pluralism'. Medical pluralism describes a model in which healthcare is made up of medical professionals and scientific technologies alongside traditional beliefs and practices31 , and has previously been reported amongst urban and rural Tanzanians15,32. The finding of medical pluralism in this study suggests that beliefs in witchcraft are not a barrier to the acceptance of ultrasound into local culture. In further support of this idea, the traditional practices women reported during pregnancy (such as sexual abstinence, and resting) did not appear to conflict with ultrasound services. It should be noted however that one interviewee described the belief held by older women in her community that “…if you tell your date of delivery to someone they can prevent you delivering on that day.” This belief was not noted in reviewed literature. Depending on how widespread this cultural concern is the disclosure of EDD, whether calculated by LMP or by an ultrasound scan, needs to be handled sensitively and confidentially. The decision to attend antenatal care Interviewees in this study commonly discussed ANC attendance with their husbands, and occasionally with relatives or partners if not married. The balance of decision making power differed between women: “For this pregnancy I discussed going to ANC with my husband and my mother, and gained their permission to go.” “I told my husband.” “Did you talk with him, tell him or ask his permission to go?” “I just told him.” A women's dignity project, in Dar es Salaam, Tanzania33 , has found that family, friends and the partner of a woman often directly and indirectly influence her choices regarding pregnancy, labour and delivery. The influence of family and friends was especially strong if the woman is especially young, poor, or disempowered. Service uptake is known to be affected by gender roles in Tanzania15. In this study, interviewees who were questioned about gender of sonographers predominantly had no preferences. However, a minority explained they were uncomfortable with the idea of male sonographers: “If it was a man I would let him because I want help but I would feel very shy...” “I would have a female doctor only.” Nonetheless, all women were always unaccompanied during consultations with both male and female ultrasonographers. Gestation at first ANC visit Interview participants made their first ANC visit between 1-7 months gestation (Figure 1). These timings were not inconsistent with National statistics showing that 80% of women make their first visit after 16 weeks, and 33% after 24 weeks 21 . Many interviewees were unsure of the advised time to start attending ANC. Notably, knowledge and beliefs about timing did not always correspond with practice. “… I know I should come earlier but I just didn't.” No interviewees attended for their first ANC visit before 12 weeks. Only 9 (36%) interviewees confirmed their 1st attendance at ANC was before 24 weeks. The pilot ultrasound service offers routine ultrasounds to all women between 12-24 weeks gestations, as this has been identified as the optimum time for accurate EDD calculation. Ensuring women attend at least one ANC visit within this period may prove difficult. Basic knowledge: service awareness, sources of information, procedure understanding Experience and awareness of obstetric ultrasound Table 4 shows the number of women participants (interviewees and questionnaire respondents) who had undergone a previous ultrasound examination. In both groups the majority of women had not previous had an obstetric ultrasound. The difference was particularly notable for questionnaire respondents; the small number of women who completed Questionnaire II (n=5) compared to Questionnaire I (36) likely reflects the limited use of ultrasound prior to this study. Some interviewees, and 11 (31%) of the questionnaire I participants who had not had a previous ultrasound were totally unaware of the ultrasound as a concept. Among women who had heard about the use of ultrasound in pregnancy, knowledge that a prenatal ultrasound service was routinely available at BomaNg'ombe was poor. “Were you told about ultrasound at the local clinic?” “No I wasn't told about it or that it was available in BomaNg'ombe.” Sources of information Most interviewees had heard or learnt about ultrasound from other community members. Family and friends were key sources of information for participants in this study, which is consistent with prior qualitative studies into knowledge of ultrasound in developed and developing countries alike 13,19. In this study, all individual members of the community who had given information about ultrasound scans to interviewees were female; a friend, neighbour or relative. No interviewee mentioned a man giving information or advice on ultrasound. We are unaware of this being recorded in previous literature. Participants reported very little education about ultrasound from schools, health professionals or media. This is significant because women's expectations and experiences of ultrasound scans are known to be inherently linked to the amount of information given 14 . Inadequate information provision in health facilities, as found in this study has been recorded in other developing countries12,13,34,35 as well as developed countries7,36-38. The insignificant role of the media in education and awareness about ultrasound scans may be due to lack of access by women to TV, radio and printed media, and or a lack of ultrasound education content in the media. Understanding of the procedure Interviewees were questioned about their knowledge of the procedure before the doctor present spoke to them about the ultrasound examinations. Interviewees who had never heard of ultrasound scans logically were unaware of the procedure and purpose of ultrasound scans. Interviewees who had not previously had an ultrasound but were aware of them either knew nothing about the ultrasound procedure, or could describe the basic steps: “They put something oily on the stomach, apply something and see a picture through computer.” “No, I don't know anything about that, and I am worried that I could get pain...” After their ultrasound examination, some women said that certain aspects of the procedure were unexpected, such as having to lie on their back and being able to see the baby on the screen. For some of these women, this visit to the antenatal clinic was not their first suggesting a lack of adequate explanation about ultrasound during earlier contact with healthcare professionals. Perceived benefits: expected outcomes, accuracy and capacity and positive experiences Expected beneficial outcomes following ultrasound When interviewed, women often explained one or more ultrasound purposes, even if they did not know the procedure. Interviewees and questionnaire participants gave a range of perceived uses of ultrasound (Figure 2). However, whilst some of these perceived uses are accurate, some are possible but not certain, some are dependent on timing of the ultrasound, and some are misconceptions. Interestingly 3 interviewees said they did not know the purpose of ultrasound, but went on to give examples of uses through the interview. Nonetheless 16 (51.6%) women completing Questionnaire I had no knowledge of what an ultrasound was used for. In the UK, Sweden and Australia the pleasures of emotional reassurance and seeing the baby are common reasons for desiring ultrasound scans7,39. Perceived advantages of ultrasound recorded in this study appeared to be more clinically focussed than this, possibly because Tanzanian women are less aware that the mother can see the baby, and are less aware of the emotional benefits of ultrasound because ultrasound has only been recently introduced. Figure 2 quantifies how many women reported certain perceived purposes of ultrasound. Pregnancy and fetal viability verification was a commonly stated reason for wanting an ultrasound by participants in this study. This finding is consistent with research reports from Syria35 , South West Nigeria11 and Botswana14 . It has been proposed that this strong desire for pregnancy confirmation may be due to a lack of access to, or faith in, other methods of pregnancy testing, compared to in developed countries14,40. Another explanation, as has been suggested in South West Nigeria, relates to the cultural pressures of living in “a community where matrimonial success is hinged on conception and eventual delivery of a live baby”11 . This study found that a number of both interview and questionnaire participants desired ultrasound scans in order to determine the fetal gender. Desire to discover fetal gender, due to the want for a particular gender of baby, has been documented as a reason why pregnant women covet ultrasound scans in Nigeria10. In societies with strong male preference, such as India, ultrasound has been used for sex-selective abortions41. Whilst male-preference has been noted amongst the Chagga tribe in Northern Tanzania42 , in this study, (in which 13/25 interviewees were Chagga) there was no evidence of sex-preference through interviews or questionnaires. Currently it is not the practice to determine fetal sex during ultrasound examination at BomaNg'ombe. It should be considered whether women would find this a disincentive for the uptake of ultrasound scans or not. Understanding of accuracy and value of ultrasound Discussion about the accuracy of ultrasound versus LMP in estimating EDD took place with certain interviewees. Of these women, most correctly identified LMP as being less accurate than ultrasound. Nonetheless, certain interviewees who had not delivered by the exact day predicted by LMP immediately believed that they were overdue and there was a problem with their pregnancy. It seems that women often did not understand that EDD was an estimate not an exact predication, whether derived from ultrasound or LMP. Many women over-estimated the diagnostic power of ultrasound. The finding of over-estimation of ultrasound's diagnostic capability found in this study, was also recorded in Vietnam34 , Nigeria13 and Botswana14 following the introduction of this technology. Interviewees often remarked that ultrasound can show 'any' and 'all' problems. One dangerous misconception held by Questionnaire I participants, (with no ultrasound experience) was the expectation that ultrasound shows whether they or their baby had 'diseases'. One such participant specified a disease they believed could be detected: “I expect to know if I am affected with HIV virus so that I may prevent my baby from getting infection.” Under the assumption that ultrasound can detect all problems or diseases, women who are not told that they have a disease such as HIV, or that their baby has a disability, may interpret the absence of reporting of such problems to mean they are not there. Although this is supposition, the seriousness of the consequences of this makes it a worthy consideration. Equally, Tautz et al. have found that high ultrasound expectations can cause distress when ultrasound cannot diagnose a problem14 and distress may also occur due to inaccuracies in ultrasound. Interview participants commented that ultrasound works beyond the scope of midwives. Ultrasound was said to recognise problems that “can't be seen by eyes” and that without ultrasound “you will not know”. Over-reliance and over-use of ultrasound are possible consequences of this sort of attitude1 . For example, Botswanan women and staff de-emphasised history taking and physical examinations once ultrasound was introduced14 . Tautz et al.14 also found Botswanan women valued ultrasound over local practices, because of its associations with white doctors. Over-estimation of the capability of ultrasound, and subsequent over-reliance on the technology may relate to 'gizmo idolatry'. This phenomenon is described as an unconditional acceptance of a technology without the guarantee of its proven clinical benefit, linked to the conviction that machinery is inherently more valuable than a less technological approach, unless there is evidence to the contrary43. In contrast to over-estimation of capacity, some participants thought ultrasound scans are only useful following discovery of a problem, a view which could affect the uptake and acceptability of routine ultrasound scans. No Questionnaire II participant (who had already experienced ultrasound) suggested unrealistic expectations, except being told fetal gender, which is not current practice at BomaNg'ombe. Reported positive experiences Interviewees and Questionnaire II respondents who had experienced ultrasound said that being told the EDD was practically and psychologically helpful in preparing for the baby, including financial readiness and planning for hospital deliveries. The fact that women in this study found an EDD useful for planning delivery in hospitals is important given only 47% of births currently occur in Tanzanian health facilities 21. The value of an EDD was also found in both Nigeria13 and Botswana14. Many women enjoyed the scans. Enjoyment was often linked to relief following initial anxieties about harm from ultrasound, and the very fact that their desire to have a scan had been fulfilled. Viewing the baby was commonly the most enjoyable ultrasound feature in this study, as found in other research7,8,35. Certain participants found that seeing the baby was pleasurable, confirmed life and pregnancy, and brought closeness with their baby. “Did the scan alter your feelings towards the baby, or thoughts about the baby?” “Yes.” “In what ways?” “Because I saw the baby playing and moving, and felt close to the baby.” Other participants reported no difference in thoughts or emotions about the baby. Literature is divided on whether or not there are tangible effects of ultrasound on maternal-fetal attachment6,35,44. Anxieties and fears Worry about results In developed countries anxiety is often related to the potential or actual detection of fetal abnormalities7,19. Afew women in this study expressed such fears: “I had despaired that the baby had an abnormality…” “I am worried as I had an ultrasound and this showed a mass...” However, the detection of fetal abnormalities was not the most common cause of anxiety about ultrasound in this study. Anxiety about abnormalities may be lower in countries where induced abortions are illegal, such as in Tanzania28 as abnormalities are not associated with dilemmas of whether or not to terminate, as is found in developed countries7,19. Fears of harm A much more dominant fear amongst pregnant women was harm from ultrasounds. Many participants had heard, and/or strongly believed themselves, that ultrasound can cause significant pain, injury or impairment to mothers or their babies. This was mainly expressed in interviews. “...people say that ultrasound reduces the gestational age of the baby.” “Some say ultrasound isn't good because it causes disability and has radiation.” “Friends say that repeating the ultrasound several times it may cause you to become anaemic because it takes some blood from your body.” “Before my first ultrasound I had ideas that ultrasound reduced the number of years for the mother and baby to live.” “ ...during ultrasound the penetration of the rays may change the colour on the site it hits.” “On the mother?” “No, on the fetus, change the colour of their skin.” However, some Questionnaire I participants also expressed severe fears about the side effects of ultrasound. “Have you ever heard of any bad effects of the scan?” “Death of the fetus.” When questioned after ultrasound examinations, no participants said that they had experienced pain or injury. Nonetheless, significant fears, specifically of physical harm and pain, were not uncommon prior to ultrasound examinations. “I thought I would be harmed.” “What did you think was going to happen?” “I thought I was going to undergo some surgery…” The following is an extract from field notes made during the observation of a young Maasai woman having an ultrasound scan for the first time: 'The lady is very cautious about getting onto the bed, then reluctant about lying down...When the Dr. picks up the gel bottle and goes to put gel on her, she jumps and retracts...The Dr. gets out the transducer and she is again very scared and draws away...he shows her the transducer repeatedly and puts it on his skin, then her arm, then on her abdomen. She seems to accept the transducer but is still very frightened...she is looking away...When the Dr. twists a knob on the ultrasound machine, again she starts because she is very frightened about what he is doing.’ Following this interaction the doctor explained that the woman thought the doctor was going to cut her open with the ultrasound machine. Whilst the safety of ultrasound examinations has been contested in multiple countries, fear of harm to the fetus or mother is now an unusual concern in developed countries7,34 . Oakley37 argues that safety fears reduce with the time technology is in use. In countries where ultrasound has been recently introduced views seem mixed. 43% of interviewees in one Nigerian study were 'unsure' about harm13 whilst only 0.4% of Syrian women questioned the safety of ultrasounds in recent research34 . In Botswana, Tautz et al. found 75% of women saw no risks in ultrasound, but amongst the remaining women there were significant fears surrounding ultrasound scans, such as the light being turned off during an ultrasound scan being associated with impending death14 . This suggests that depending on local culture, small differences in hospital practice can have a great impact upon how ultrasound is experienced. Information and reassurance The fears of pregnant women recorded in this study highlighted a lack of understanding about the procedure, purpose and lack of harm, prior to ultrasound scans. Women reported that a lack of information was consistently associated with increased fear and misconceptions, and vice versa, concurrent with findings from various countries 2,6,13,14. Participants who believed ultrasound to be safe based this on trust in the knowledge of doctors, personal experience and experiences of others. “...I know women have it and trust the doctors.” Such participants wanted to reassure others that “It is ok, there is no harm, it will not hurt”. Uptake of ultrasound Option or obligation? No women interviewed expressed a belief that they had a choice regarding the decision to have an ultrasound scan. It was a common belief that if a woman attended ANC, an ultrasound scan was obligatory. “I think I have to have it.” The World Health Organisation emphasised the need for informed consent and choice before having an antenatal ultrasound examination as early as 198445 . Fully informed consent allows understanding of the purpose, limitations and procedure of ultrasound, and choice to accept or decline46,47 . The absence of informed consent has been documented worldwide6,7,12,13, 34-38. Do women want one? Some interviewees believed routine ultrasound scans, without clinical indication, were important. In contrast, other women thought only clinically indicated scans were necessary. “...I didn't get any abnormal problems or any conditions that made me think to have an ultrasound.” Ultrasound scans were generally seen as advantageous, and certain women described themselves as “anxious” to get one. All interviewees desired ultrasonography even when knowledge of the concept and purpose was limited. This corresponds to findings in Nigeria12 , Nicaragua3 , Hanoi34 , and other less developed country settings47 . All interviewees advised others to have an ultrasound, and one woman recommended that ultrasound scans be made available in rural clinics. From Questionnaire II, advice for friends about ultrasound scans was also positive: “I will tell that the scan is good and is very important for pregnant mothers.” Interview and questionnaire participants who hadn't experienced ultrasound gave lack of knowledge as one reason why they wanted ultrasound scans. “I want to know what it is, how does it work?” “I want to know advantages and disadvantages.” Whilst there was unanimous reported desire for ultrasound scans in interviews, 6 (17%) of Questionnaire I respondents (women without prior experience of ultrasound) did not want an ultrasound and 7 (19%) would not recommend it for others. The reasons for not wanting an ultrasound were not always related to fears of side-effects or harm. For example, one Questionnaire I respondent was aware of real benefits of ultrasound and had never heard of any negative effects of ultrasound, but she did not want to have an ultrasound. Despite certain women openly admitting to not wanting to have an ultrasound, and the fears of ultrasound expressed by women in this study, no-one has yet declined an antenatal ultrasound at BomaNg'ombe. There are multiple possible explanations for this. Firstly, it is possible that the women that do not want an ultrasound prior to consultations change their opinions during discussions with a doctor. Secondly, pressure on women to accept an ultrasound by staff, both perceived and real, has been recorded in multiple settings6,7,48 and this could account for the differences between views and decline rates in BomaNg'ombe. Finally, women at BomaNg'ombe may believe that ultrasound scans are obligatory, as did all study interviewees. This view may be compounded by the mere routine provision of ultrasound scans15,38 and lack of informed consent. The fact that Questionnaire I respondents included women who did not wish to have an ultrasound, whilst all interviewees expressed the wish to have an ultrasound, may be due to increased perceived pressure to show a desire for ultrasonography in front of the interviewer and doctors in interviews, versus the anonymous questionnaires. The implication of this is that questionnaires should be included alongside interviews in future qualitative research of this sort. Impact of ultrasound on uptake of antenatal care When interviewees were asked why they thought ANC was important, or why they wanted to attend, having an ultrasound scan was never offered as a reason. However, all interviewees said that they desired an ultrasound examination. Of this group, almost all said that ultrasound availability made ANC seem more appealing to them, and that they thought it would increase attendance at clinics by other women. “Yes, I would like to go to clinics with ultrasound because my problem was seen by ultrasound, and can't be seen by eyes.” “It [ultrasound] makes me want to go more.” Ultrasound could increase early attendance at antenatal clinics, providing that availability and timing requirements were well known about. This idea is supported by Hofmeyr8 . Such an outcome would be extremely valuable given the problem of late uptake of ANC in Tanzania. However, the hope that ultrasound could increase attendance from this study at antenatal clinics is based on opinions of participants who already attend clinics and who already desire ultrasound. This conclusion cannot be generalised to women not wanting ultrasound (6 (17%) completing Questionnaire I), or women not attending ANC. Key findings
Recommendations 1) Clinical practice There is a need to strengthen informed consent to facilitate understanding of the purpose, procedure and limitations of ultrasound scans and to protect women's autonomy46,47 . Training sonography and ANC staff in gaining informed consent will facilitate policy implementation. Cash et al.49 highlight the importance of training of health centre workers in how to counsel pregnant women about ultrasound, and of providing written material to women to take away following consultations. Where possible, women should have the option of a female sonographer if requested. If this is difficult logistically a chaperone policy may be useful. Information about date of delivery should also take account of cultural anxieties about this issue, and include an explanation to women that EDD (whether derived from LMP or ultrasound) is an estimate not a predication. 2) Public education Poor understanding and negative expectations and experiences of ANC and ultrasound may limit uptake. There is a need for improved public education which focuses on: the availability and recommended timing of ultrasound, benefits of ultrasound, and dispelling misconceptions. Education in health facilities Health care workers are an important tool for disseminating information about ultrasound, and increasing awareness of the service. Information regarding ultrasound may best be conveyed during normal clinic routines, as well as being incorporated into already existing education workshops for pregnant women and mothers. Posters advertising health promotion, breast feeding and other advice are already being utilised in BomaNg'ombe. Extending this to include posters giving information on ultrasound therefore seems appropriate. Using positive comments about ultrasound by local women may be a powerful method for dispelling misconceptions. Posters advertising health promotion, breast feeding and other advice are already displayed in BomaNg'ombe ANC clinic. Extending this to include posters giving information on ultrasound therefore seems appropriate. Using positive comments about ultrasound by local women may be a powerful method for dispelling misconceptions. Media education Internet programmes have been used as a tool for increasing understanding and choice amongst pregnant women about ultrasound screening tests in Canada50 . Whilst this may be effective in developed countries, where access to computers and internet is readily available, this approach seems currently unlikely to currently have widespread effectiveness in rural Tanzania. In efforts to increase education about obstetric fistulas across African countries, radio announcements, village theatre and print media have been employed51 . Options for print methods include newspapers, billboards, leaflets and posters in clinics or community areas. Given illiteracy is not uncommon in BomaNg'ombe it would be important to include at least one non-print delivery mechanism. Utilising religious leaders, market gatherings and schools has also been used effectively in rural African communities, where word of mouth and education from other community members is known to be critical51. Who to target? Given the involvement of many husbands, and family and friends, in a woman's decision regarding ultrasound and ANC, it is important not to focus education at pregnant women solely. Engaging men may be particularly helpful. This could be through workshops to change knowledge and attitudes as has been used in Uganda with regards to obstetric fistula education52 . Women who do not attend ANC, and under 18 year olds, should be key target groups for educational messages as these groups are at greater risk of obstetric complications21 . Maternity care could be included in school education. 3) Ideas and advice for further research This study excluded women who did not attend ANC and women under 18 years of age. These groups are particularly vulnerable to problems in pregnancy so ANC and ultrasound uptake should be especially encouraged among these women. It is likely that such women would have even less prior familiarity with the concept of ultrasound compared to those who are older, and have attended ANC. Further research with these groups of women is essential. Other groups in which it may be beneficial to investigate attitudes towards ANC and ultrasound include primigravidae, healthcare staff and women in traditionally living communities (e.g. Maasai). Regarding methods for similar future research, the use of community interpreters rather than medical practitioners may be prudent in similar research in order to increase freedom of speech and prevent 'medicalised' interpretations of what women are saying. As mentioned earlier, it was apparent in this paper that questionnaires may allow greater freedom of speech than interviews. It is therefore suggested that questionnaires make a valuable addition to a methodology alongside interviews for qualitative research. Research into women's beliefs, expectations and possible experiences of ultrasound should ideally have taken place before the pilot introduction of ultrasound into the BomaNg'ombe area, in order to guide best practice and reduce harms. It is widely stated that service user's views are important to health organisations. However, the importance of such views, and their impact upon uptake of series are often underestimated, and research into views and acceptability of a new intervention is not always explored before an intervention is established. This is something to think about when introducing a new intervention in any area. Acknowledgments We would like to thank all the women who participated in this study, for openly expressing their knowledge, feelings and experiences. In addition: the staff at BomaNg'ombe Reproductive and Child Health Clinic for their help in implementing this research, especially Dr. Swai and Dr. Kessy for their interpreting services; Dr. Paul Chaote for granting study approval; Dr. Ewan Hunter and Dr. Gerry Mshana who provided guidance on undertaking research in the locality; Dr. Mengiste Melese and others who taught the intercalated international health degree 2009/10 at The Nuffield Centre for International Health and Development. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11023t1.jpg] [rh11023t2.jpg] [rh11023t4.jpg] [rh11023f1.jpg] [rh11023f2.jpg] [rh11023t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}