 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
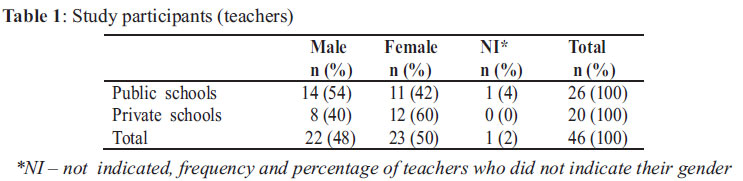
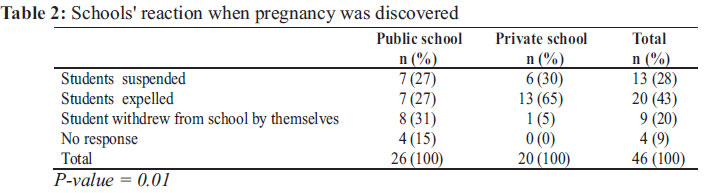
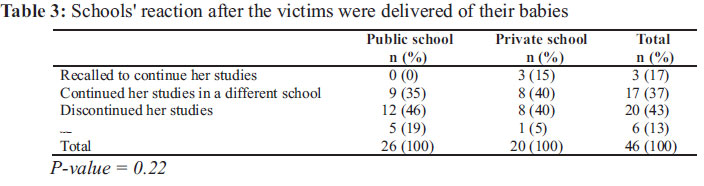
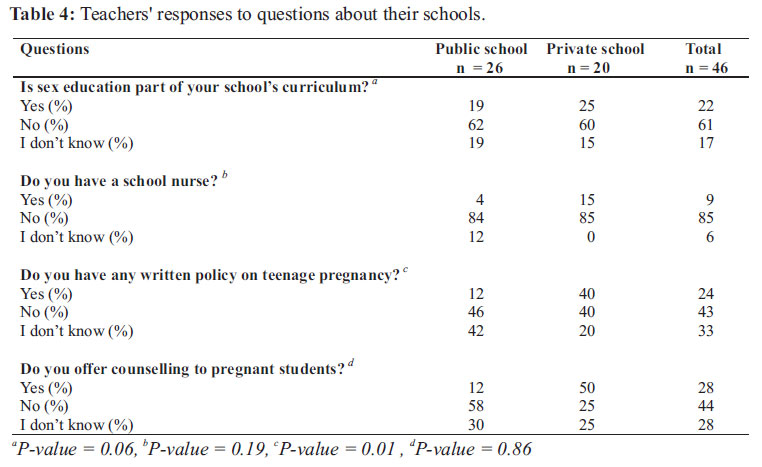
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 109-116 ORIGINAL RESEARCH ARTICLES Unintended pregnancy and termination of studies among students in Anambra state, Nigeria: Are secondary schools playing their part? Ifeoma N. Onyeka1 , Juhani Miettola1 , Amobi L. Ilika2 , Tuula Vaskilampi1 Address: 1 Institute of Public Health and Clinical Nutrition, University of Eastern Finland, Kuopio Campus, P.O.Box 1627, 70211 Kuopio, Finland and 2 Department of Community Medicine, Nnamdi Azikiwe University Teaching Hospital, PMB 5025, Nnewi, Nigeria. Code Number: rh11024 Abstract This study evaluated efforts of secondary schools to prevent unintended pregnancy among students and their reactions to pregnant students before and after delivery. A cross-sectional survey of 46 teachers in three public and two private schools in Anambra state, Nigeria was carried out. Information was collected using self-administered questionnaire. Of all the teachers in the study, 87% reported unintended pregnancies among students in the previous 3 years. Expulsion (43%) and suspension (28%) were the most common reactions. Private schools were more likely to expel pregnant students than public schools. Following the delivery of their babies, 43% discontinued their education in the same school, whereas 37% continued their education in a different school. Counselling was given before suspension or expulsion in 4% of public schools and 15% of private schools. Majority of the schools (61%) did not have sex education as part of their schools' curriculum. Students should be re-admitted in order to ensure continuity of their academic development, prevent unemployment and mitigate poverty-induced repeat pregnancy. Résumé Cette étude a évalué les efforts des écoles secondaires pour prévenir les grossesses non voulues chez les étudiantes et leurs réactions envers les étudiantes enceintes avant et après l'accouchement. Nous avons mené une enquête transversale auprès de 46 enseignants dans trois écoles publiques et deux écoles privées dans l'état d'Anambra au Nigéria. Les données ont été collectées à travers un questionnaire auto-administré. De tous les enseignants concernés dans l'étude, 87% ont signalé les grossesses non voulues chez les étudiants au cour de trois ans précédents. Les réactions les plus communes ont été l'expulsion (43%) et le renvoi (28%). Les écoles privées avaient plus la possibilité d'expulser les étudiantes enceintes que les écoles publiques. Suite à l'accouchement de leurs bébés, 43% ont cessé de fréquenter la même école alors que 37% ont continué leurs études dans une autre école. Avant la suspension ou le renvoi, 4% des étudiantes enceintes dans les écoles publique ont reçu des conseils d'orientation et 15% dans les écoles privées. Dans la majorité des écoles (61%), l'éducation sexuelle ne figure sur programmes d'études. Il faut réadmettre les étudiantes pour assurer la continuité de leur progrès académique, prévenir le chômage et réduire la grossesse répétée causée par la pauvreté. Key words: Teenage pregnancy, Cross-sectional Survey, Secondary School, Nigeria, High School Drop-out Introduction Unintended pregnancy is an important social and public health problem among young females in Nigeria. Due to cultural barriers, discussions around sexuality and reproductive health issues are not common between young people and adult members of their families. This leaves teenagers uninformed/ misinformed about sexuality and the risks associated with early and unprotected sexual activity, including unintended pregnancy, sexually transmitted infections (STIs), and HIV/AIDS 1 . Pre-marital sex and resultant pregnancy are seen as violation of moral principles, which attracts different forms of stigmatization from individuals and members of the community. For the student, the chances of expulsion from school increases with unintended pregnancy and this is often a measure to prevent contamination of other students. Therefore, unintended pregnancy is a major cause of termination of studies among females enrolled in secondary school. A previous study has documented similar situation in another African country2. Schools are agents of change and could play vital roles in preventing pregnancies among female students. Due to their proximity to the students, teachers are among the most important stakeholders in creating awareness of the consequences of sexual-risk taking, including unintended pregnancy. They are in good position to provide students with reliable information on sexual and reproductive health issues. In their study, Williams and Bonner3 found that sex education provided in school was effective in reducing unintended pregnancy and abortion. For pregnant students, continuity of education is very important for achieving Millennium Development goals 4. Termination of secondary school education will initiate a cycle of illiteracy, unemployment and poverty for the affected students. They are unable to take care of their babies due to little or no incomeearning capacities and are at risk of poverty-induced repeat pregnancy. There is need for schools to readmit students and their parents-teachers-association (PTA) meetings could be an avenue to prevail on parents to encourage their daughters to complete their secondary school education. This study aims to evaluate efforts of schools to prevent unintended pregnancy and reactions to students when they become pregnant and after the delivery of their babies. To the best of our knowledge, these areas have been largely unexplored in Anambra state. Methods A cross-sectional study was carried out in five secondary schools of which three were public and two private schools in Anambra state, south eastern Nigeria. The entire study is made up of a qualitative part involving parents from the community and a quantitative part involving students and their teachers. Details of the quantitative part of this study have been described elsewhere 5 and a brief description will be provided here. A total of 1,234 students and 46 teachers were surveyed using selfadministered questionnaires. The survey of both students and teachers in each school took place on the same day. However, in this research report, only data from teachers will be presented. Only teachers who were available on the day of survey took part in the study and this accounted for the small sample size. The teachers completed the questionnaires in their staff rooms. Items on the questionnaire included both multiple choice and open-ended questions. Participation was voluntary and participants were duely informed on the questionnaire that their responses would be handled confidentially. Written permissions were obtained from the principals/proprietors of all the schools. The Ethics Committee of Nnamdi Azikiwe University Teaching Hospital, Nnewi gave an approval for this study. Statistical differences were analyzed using Fisher's exact test and the level of significance was set at alpha (0.05). Data analysis was done using Statistical Package for Social Sciences version 14 (SPSS Inc Chicago, IL). Results Twenty-six teachers from public schools and twenty from private schools completed the questionnaires. Generally, there was near-equal gender participation in the study (Table 1). More than half of the respondents from public schools were males. Conversely, 6 out of 10 respondents from private schools were females. Of all respondents, 87% (n=40) reported unintended pregnancies among their female students within the last 3 years. In public schools, reports of pregnancy were more common (35%) among students in Junior Secondary School (JSS) year 2 and in private schools, more common among JSS year 3 students (40%). In all schools, Senior Secondary School (SSS) year 2 students had the least cases of unintended pregnancy. Overall, the pregnant students were either suspended or expelled from their schools when the pregnancies were discovered (Table 2). Most pregnant students in public schools withdrew by themselves before the schools found out while those in private schools were more likely to be expelled from school. The difference between the schools was statistically significant. In both types of school, most of the students either totally terminate or continue their studies in a different school following the delivery of their babies (Table 3). Termination of studies was more common in public than private schools. Some private school teachers reported that students were recalled to continue their education in the same school. However, this type of report was completely absent in the public schools. In public schools, almost 20% of all respondents did not know the post-delivery schooling status of their students. On the average, counselling was not provided to the pregnant students. More teachers in private schools (50%) reported counselling to pregnant students than teachers in public schools (Table 4). Where counselling was provided, it was mostly given as soon as pregnancies were discovered in both schools - 8% in public schools and 20% in private schools. Counselling was also given before suspension or expulsion in 4% of public schools and 15% of private schools. Students who were recalled to continue their studies in private schools also received some counselling (10%). Information provided during counselling sessions in both types of school was centered on the consequences of teenage pregnancy and abortion (17%), abstinence from premarital sex (4%) and keeping good company and joining religious groups (4%). However, 77% of public school teachers and 65% of private school teachers did not respond to the question on information provided during counselling sessions. In their opinions, most public (80%) and private (70%) school teachers recommended provision of counselling to pregnant students. Almost half of the teachers in public schools admitted that they did not have any written policy on unintended pregnancy. In private schools, four in ten teachers either gave a positive or negative response to the question. The only written policy mentioned by some of the public school teachers (12%) was suspension and re-admission of pregnant students after delivery of their babies. In private schools, written policies listed by the teachers were: suspension and re-admission of pregnant students (5%), expulsion from school with or without punishment (25%), and restricting visitation and intimacy between opposite sex (5%). On the average, almost eight in ten teachers failed to list any written policies in existence in their schools – 88% of teachers in public schools and 65% of those in private schools. There was no difference between public and private schools, in terms of availability of school nurses. Of all the teachers, more than 8 out of 10 reported that they did not have any school nurse. Similarly, majority of the schools did not have sex education as part of their schools' curriculum. Where sex education was offered, topics mostly discussed included social and economic problems associated with unintended pregnancy; abortion and complications arising from it; and sexually transmitted infections, including HIV/AIDS. However, more than half the teachers in both schools (55%) did not provide details of sex education offered to their students. In spite of this, majority of all the teachers opined that sex education was very important to the students. Eighty-four percent in public schools and 80% in private schools recommended that sex education should be provided at school. The remaining 15% and 20% respectively were opposed to the provision of such information. In general, one-third of the teachers suggested that unintended pregnancy could be prevented using a combination of moral/religious instructions, sex education, proper parental upbringing and adequate financial provision for female students. Other measures suggested were: having separate rooms/schools for different genders, providing counselling services, organizing seminars/workshops, movies and drama presentations, and involvement of PTA/advocacy groups. Discussion There were no written policies on unintended pregnancy in most schools in this study. Although some teachers responded positively to the question, majority of them failed to list such policies in existence in their schools. Again, this casts doubt on the credibility of their initial responses. Nevertheless, expulsion was the most common reaction to unintended pregnancy. Private schools were more likely to expel pregnant students than public schools. Some pregnant students were suspended but it is not known how many of such students were re-admitted following the delivery of their babies. This raises concern about termination of educational development of students. Besides, expelling pregnant students from schools triggers off a cycle of poverty which might eventually predispose their own children to unintended pregnancy. Several studies have shown that some victims of unintended pregnancy were more likely to be children of mothers with limited school education and history of unintended teenage pregnancies6,7,8. In broader sense, local education authority could work in collaboration with schools to ensure continuity of studies for the affected students. In South Africa, which has a high rate of premarital adolescent childbearing, official policies are in place to allow pregnant teenagers to stay enrolled in school and allow them re-entry after giving birth 9,10. Such policies help schools to retain or reabsorb victims, reduce pregnancy-related drop out rates and further promote high levels of adolescent female school attendance. It is arguable that South Africa differs from Nigeria in many ways and it may be very challenging to apply the same policies. An effective solution should be adapted to fit country-specific needs and conditions but the ultimate goal is to promote continuous academic development of pregnant students. Our results showed that unlike private schools, public schools did not recall any student and larger percentage of students discontinued their studies after delivery of their babies. Could it be due to more bureaucratic procedures in public schools compared with liberal ones in private schools? When such students return to schools, they face enormous challenges such as finding a balance between caring for their children and devoting time to their academic work. They are also mocked and bullied by their fellow students and sometimes by their teachers 11. However, life becomes even tougher if they do not complete their education. The communities might also play important roles in encouraging young mothers to continue their education and they could prevail on school authorities to readmit such student-mothers. Where this is not possible, they might be able to persuade the government to make other provisions to enable young mothers to “catch-up”, achieve their academic goals and reach their career targets. Are we promoting sexual-risk taking and pregnancy among students? Is this a ploy to make unintended pregnancy less undesirable? The answers are resounding “no”. Unintended pregnancy is not enough reason to deny young mothers the numerous benefits that come with education. If so, many victims may be left disaffected from the society with poor future employment and life prospects 12. Besides, the community would be at the risk of losing productive manpower. Provision of counselling to pregnant students was not a common practice in all the schools. However, it was commendable that some schools offered counselling to students, and private schools were more likely to do so than public schools. Information provided during counselling sessions was very silent on continuation of education after the babies were born. Most of the teachers could not provide details of topics discussed with pregnant students during the counseling sessions. This raises doubts on the accuracy of responses provided by other teachers. Majority of the schools did not have school nurses and this calls into question, the level of implementation of Nigerian School Health Policy. School nurses are important in order to address health problems of students and to provide useful health (including sexuality and reproductive health) information to students. Within the school-based clinics, trained nurses could offer reproductive health counselling to reinforce what is taught in the classrooms. This creates an opportunity for students to ask confidential questions and receive answers directly from health professionals. Such counselling units are highly essential to reduce teenage pregnancy 13. In addition, pregnant students could receive guidance and information on community support which may serve to prevent negative outcomes of pregnancy, prevent repeat pregnancy and encourage students to continue their education14,15. High number of unintended pregnancies among junior students may be connected to poor knowledge of sexuality and reproductive health issues. In most schools, sex education was not part of their academic curriculum and this indicates failure to apply the nationally-approved curriculum on sex education for Nigerian schools which has been in existence since 200216 . This became even more evident when more than half of all the teachers could not list contents of sex education offered to their students. Many misgivings exist about sex education, as some people believe that it is counter-productive. Despite conflicting research findings, there is no conclusive evidence that sex education encourages, or leads to greater sexual activity among young people. Safer sexual practice among young people may be achieved through providing appropriate education on sexuality to them. As Ilika et al. suggested, it may be more appropriate to pay attention to teachers' training, approach and contents of sex education programme to avoid sending conflicting and confusing information to teenagers 17. Limitations of study Participation by teachers from both public and private schools offered useful insights into general attitude of schools within the study community. Due to the small sample size, results of this study may not be generalized to all secondary schools in Anambra state. Being a rural community, efforts and reactions of schools located in urban communities may differ considerably from those reported by our study participants. However, this study provides a background for future research studies. It will be important to know the rate of re-admission of pregnant students to continue their studies following the delivery of their babies and the rate of retention in schools. Qualitative interviews may offer insight into challenges schools encounter in the fight against unintended pregnancy. Future studies should aim to include more schools and if possible, School Heads/Principals or Proprietors. Conclusion The school is an important stakeholder in the prevention of unintended pregnancy and could play more active roles to reduce the prevalence of pregnancies in this study community. Despite poor implementation of sex education and poor provision of counselling to most pregnant students, majority of the teachers had positive opinions about them. This highlights their willingness to follow through if there are official arrangements and guidelines within the schools to ensure compliance. Continuity of academic development of pregnant students should be given due consideration. Policies should be in place to re-admit students and to address stigmatization which either prevents students from re-enrolling or makes them drop-out from school after re-admission. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11024t4.jpg] [rh11024t2.jpg] [rh11024t1.jpg] [rh11024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}