 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
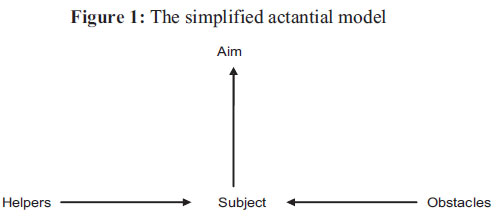
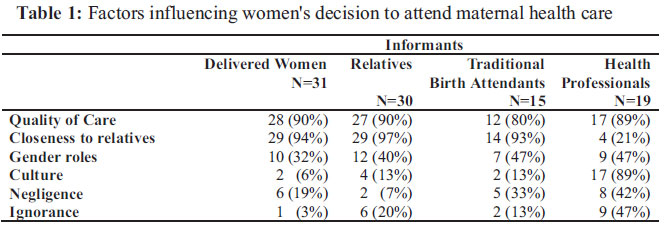
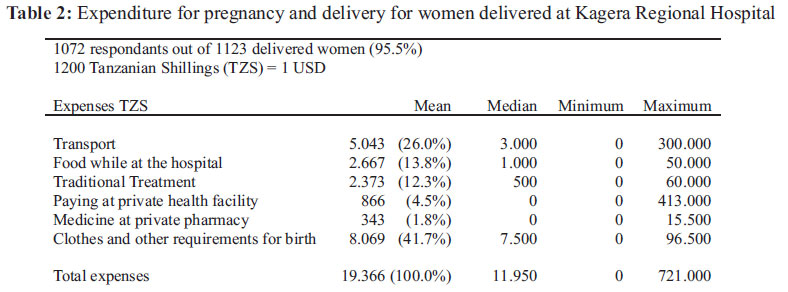
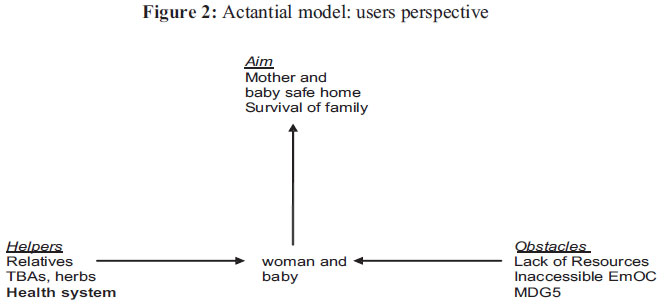
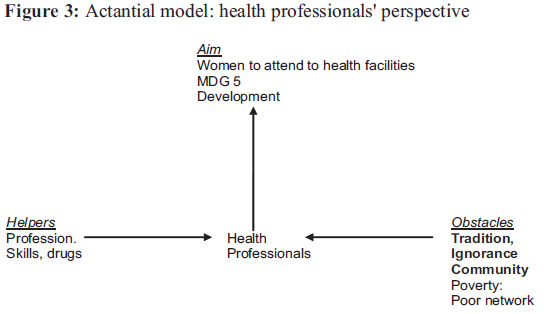
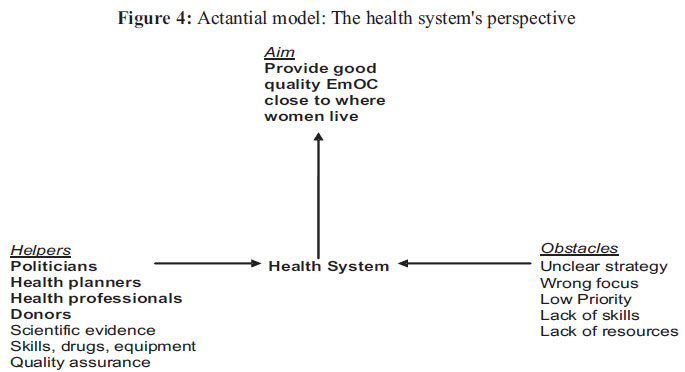
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 117-130 ORIGINAL RESEARCH ARTICLES User and provider perspectives on emergency obstetric care in a Tanzanian rural setting: A qualitative analysis of the three delays model in a field study *Bjarke Lund Sorensen1 , Birgitte BruunNielsen2, Vibeke Rasch13 , Peter Elsass4 1 Department of InternationalHealth,Immunology and Microbiology, Faculty of Health Sciences, University of Copenhagen, Denmark. E-mail: bjarkebjarke@yahoo.dk, 2 Department of Gynecology and Obstetrics, Aarhus University Hospital, Aarhus, Denmark, study supervisor. 3 Department of Obstetrics and Gynecology, Odense University Hospital, 5000 Odense C, Denmark, study supervisor. 4 Humanistic Health Research, Institute of Psychology, Faculty of SocialSciences, University of Copenhagen, Denmark, study supervisor. Code Number: rh11025 Abstract The aim of this field study was to analyze the main dynamics and conflicts in attending and providing good quality delivery care in a local Tanzanian rural setting. The women and their relatives did not see the problems of pregnancy and birth in isolation but in relation to multiple other problems they were facing in the context of poverty. Local health professionals were aware of the poor quality of care at health facilities but were still blaming the community. The study describes the difficulties within the conceptual framework of the widely used “three delays model” to disentangle different perspectives and to identify a feasible strategy of action to improve access to timely and effective emergency obstetric care. There seems to be a need for a supplementary analytic model that more clearly has the health system as the central agent responsible for improving maternal health. A modified “actantial model" is suggested for that purpose. Résumé Cette enquête sur le terrain avait pour objectif d'analyser les dynamique et les conflits centraux par rapport à l'assurance du soin d'accouchement dans un cadre rurale tanzanien. Les femmes et les parents n'ont pas perçu les problèmes de la grossesse et de l'accouchement isolément, mais en relation aux autres multiples problèmes auxquels elles font face dans le contexte de la pauvreté. Les professionnels de santé locaux étaient au courant de la mauvaise qualité de soin dans les établissements sanitaires, mais elles blâmaient toujours la communauté. L'étude fait une description des difficultés dans le cadre conceptuel du « modèle des trois retards » qui est communément utilisé pour démêler les perspectives différents et pour identifier une stratégie d'action faisable pour améliorer l'accès à un soin obstétrique d'urgence opportun et efficace. Il semble qu'il y ait le besoin d'un modèle analytique supplémentaire a plus clairement le système de santé comme l'agent central qui est responsable de l'amélioration de la santé maternelle. Un « modèle actionnel » est préconisé pour la circonstance. Key words: Teenage pregnancy, Cross-sectional Survey, Secondary School, Nigeria, High School Drop-out Introduction Maternal mortality is the health indicator with the highest disparity between rich and poor countries; out of 100 maternal deaths 99 happen in low resource countries1 . For decades world leaders have promised to reduce maternal deaths, as set out in the fifth Millennium Development Goal (MDG 5) by the United Nations: A 75% reduction in maternal mortality by the year 2015 compared to 19902 . Until now the overall progress has been disappointing3 . A number of countries in Asia and Latin America have had significant improvements but in Tanzania and other sub-Saharan African countries, where problems have been most severe from the beginning, progress has not been satisfactory4,5. Most maternal deaths happen around the time of birth in 'low risk pregnancies'. The main strategy to reach MDG 5 is to have 90% of births attended by a 'skilled birth attendant' (SBA); a midwife or a person trained in midwifery skills capable of managing normal deliveries and diagnosing, managing or referring women with obstetric complications. It has been argued that SBAs can prevent complications from developing into life threatening situations6 . However, a review of ecological, observational studies from developing world contexts concludes that there is 'little evidence that giving birth with a health professional reduces the risk of dying, and in some settings it appears to be associated with an increased risk of dying'7 . An explanation for these findings could be that SBAs cannot assure 'skilled birth attendance' if working in a 'non-enabling environment' lacking necessary supplies, staff, training and supervision8. Globally, the most common causes of maternal deaths are bleeding complications, especially post partum haemorrhage (PPH), complications from abortions, eclampsia, infections and obstructed labour. There is increasing awareness that it is of central importance that SBAs can manage these complications. The United Nations have stated signal functions of emergency obstetric care (EmOC)1. Basic EmOC should be provided at any health facility providing 'skilled birth attendance' and accessible within two hours from where women live while Comprehensive EmOC that includes caesarean section and blood transfusion should be accessible within 12 hours9. Thaddeus and Maine proposed a three delays model that has been the dominating framework for discussing delays in EmOC over the last 15 years. When women suffer obstetric complications, delays in getting relevant care are divided into three categories; 1) delays within the family and community in the decision to seek care; 2) transport delays; and 3) delays within the health facilities. Quality of care affects all three levels of delay; the perceived quality of care is likely to affect decisions in the family10-13, the distance to travel depends on how far the nearest health facility with good quality EmOC is, and, obviously, the quality of the EmOC provided at the health facility influences the outcome of lifethreatening complications14-17. Therefore, quality of care was suggested by Thaddeus and Maine as the most important point of intervention to prevent maternal deaths18. Health professionals' and users' understandings of quality of care may differ. Some have claimed that different understandings of what is good care can cause conflict19, while others have argued that users do not need health professionals to have a shared understanding of good health care20. An anthropological study from Uganda describes how people when encountering health problems look for possible solutions, one among several available being biomedicine. Health problems are discussed and negotiated with relatives as well as health providers21. Pragmatism has been described as the ruling principle of poor people; “the pressing concerns of most people are not problems of interpretations or existential issues of ontological certainty. They are worries about the money and supportive relationships that can give them steerage in getting through the uncertain passages of suffering”22. The objective of this study was to analyze the main dynamics and conflicts in attending and providing good quality delivery care among the involved agents in a rural setting in Tanzania. A further issue was to discuss the appropriateness of the three delays model to identify feasible ways to improve maternal health. The study aimed to 1) describe and compare the perceived quality of care and barriers to access it from both the users' and the providers' perspectives; and 2) To suggest a supplement to the three delays model that identifies an effective strategy to provide timely and good quality EmOC to women suffering obstetric complications. Material and Methods The field study took place in Kagera Region in Northwestern Tanzania between July and December 2007. Semi-structured in-depth interviews were carried out with 97 involved providers and users of delivery care at 31 births at home, at village-based health facilities and at Kagera Regional Hospital. As a supplement, 1123 women who delivered at the hospital in Fall 2008 were interviewed about their expenditure in relation to pregnancy and birth. Setting: Bugabo Division in Kagera Region was pointed out by health authorities to have a high number of maternal deaths and, therefore, it was chosen as the study site. The population in Bugabo is around 41.000, spread out between 'shambas' (fields) where subsistence farming of plantain and different tubers are combined with cash crops, mainly coffee. Dirt roads connect the 17 “villages” with the regional capital Bukoba and the distance by car is between 30 minutes and three hours. To get to a road many have to walk for up to an hour. There is one health centre and eight health dispensaries in Bugabo, all but one staffed with one or more trained nurse-midwives. In 2006, 1212 (72%) of the expected 1695 births took place at a peripheral health facility, and 109 (6%) at Kagera Regional Hospital. Delivery care is free at government health facilities. At the health centre and at one health dispensary run by faith based organisations user fees are charged. Based on the framework of Gill et al., a “walk through assessment” of the 'readiness' of emergency obstetric care in Bugabo Division was performed23 and it revealed a very limited capacity to manage obstetric complications due to the pronounced lack of basic equipment, drugs and staff. For example did only three out of the nine health facilities in Bugabo have a working sphygmomanometer and basic drugs, sutures and instruments for delivery kits were often few or missing. These drugs and equipment were supposed to be supplied by the governmental 'Medical Stores Department'. It was not within the scope of this study to explore where in the supply chain the delays were. Women suffering obstetric complications usually had to be referred to Kagera Regional Hospital that is equipped and staffed to provide comprehensive EmOC but even here substandard care and considerable delays were observed. Population The field study had as the point of departure births of conveniently sampled women from Bugabo taking place in three different locations: a) at home, b) at village health facilities (the health centre and two government health dispensaries), and c) at Kagera Regional Hospital. At (b) and (c) the births included were those that took place when the primary investigator was present to observe delivery care. After the birth the involved users and health providers were interviewed. Due to various reasons it was not possible to observe home births. Each of the TBAs conducted few deliveries, and many would not openly admit to do so as they had been threatened to be jailed by health authorities. Another problem was that many TBAs could not use a mobile phone to call the primary investigator when about to conduct a birth. Instead, the cases of home births were identified from health facility birth registers and from traditional birth attendants. All of the included home births had taken place within two weeks from the interviews. In total, 97 informants were interviewed; 31 delivered mothers, 32 relatives, 19 health professionals and 15 traditional birth attendants. The health professionals were mainly nurse-midwives and clinical officers with a three to four years theoretical training. The delivered mothers ranged in age from 18 to 40 years. Ten gave birth for the first time, and seven for the fifth time or more. At the hospital eight of the 10 deliveries were complicated for mother or child, three deliveries were by caesarean section and there were three neonatal deaths. At the health facilities in Bugabo four of 10 deliveries were complicated, three by prolonged labour, one by ante partum haemorrhage. Two of the four were referred to Kagera Regional Hospital. At the home deliveries complications were reported in only one case where the mother attended the health dispensary nearby and the placenta was delivered spontaneously. After five days the baby contracted sepsis and was taken to Kagera Government Hospital but died seven hours after admittance. Data collection All observations and interviews were performed by the PI, a medical doctor with three years of clinical training in obstetrics. Health facility deliveries were observed in the labour room while notes about clinical and non-clinical care and other events were taken down. After birth, semi-structured in depth interviews were performed with involved persons. Interviews were in English with the majority of health professionals. Interviews with mothers, relatives, traditional birth attendants and four health professionals were carried out with the help of an interpreter proficient in both English and Haya, the native tongue in Kagera Region. The interview guide had been developed by the authors and pilot tested in Bugabo by the PI and further discussed and adjusted together with the interpreter, a nurse working at the gynaecological ward at KRH. Most interviews with users and with all the TBAs took place in their homes. Some users and the health professionals were interviewed under privacy in an undisturbed room at the health facility where the birth took place. The purpose of the study was explained to informants before they were asked written informed consent. An effort was made to create a relaxed atmosphere by a welcoming attitude and by explicitly acknowledging and appreciating all answers given. It was stressed that anything could be said openly and that anonymity would be strictly maintained. There was good time available for the interviews, time was allowed for periods of silence and for active listening. All interviews were sound recorded while notes were written by the PI. The interviews lasted on average 63 minutes (15-100 minutes) and focussed on perceived dangers during pregnancy and birth, understanding of good delivery care and barriers to receive it, and suggestions for reducing the number of maternal deaths. Data analysis The interviews were transcribed verbatim by the PI. Twenty five interviews were transcribed and translated by a person fluent in both English and Haya. The Haya transcripts and their translation into English were compared to the interpreter's translations during the interviews. As no major meaning disturbing differences were found the interpreter's direct translation was found reliable. Interviews were entered in Nvivo 8 software, read through and coded by the main themes of the interview guide. The themes were read through and further coded by categories emerging from the reading, helping to structure the analysis of the extensive material. Emerging themes regarding attendance to maternal health care were 'perceived quality of care', 'support from relatives', 'gender roles', 'culture', 'negligence' and 'ignorance'. Emerging categories regarding access to health care were 'distance' and 'costs'. Survey data The qualitative data was supplemented with survey data collected at Kagera Regional Hospital the following year. In 2008, between August and November all women delivered (1123) at Kagera Regional Hospital during two seven weeks periods were included. In structured exit-interviews performed by research assistants women were asked what expenditure they had incurred in relation to their pregnancy and birth. The data were entered in Epi-Info (TM) 3.5.1 software and listed in main categories by descriptive statistical parameters. Actantial models The 'actantial model' was developed by the French-Lithuanian linguist Greimas inspired by the analysis of folktales24. The actants are the 'constant roles' that are claimed to be always present in the deep structure of a narrative. Greimas' actantial model has three pairs of actants opposing each other: 1. Subject versus Object, 2. Sender versus Receiver, and 3. Helper versus Opponent. The model is useful to make clear the important points: what should be moved towards what aim, what are the obstacles and what are the helpful factors. Compared to other narrative analytical approaches, like for example discourse or semiotic analysis, the actantial model was chosen for this study to emphasize the importance of identifying responsible agents and feasible strategies of action to improve access to timely and effective EmOC. To keep the analysis as clear and simple as possible the sender-receiver axis was omitted; it was considered of more peripheral relevance given that the study focus was the dynamics in a local setting not covering more general political and organisational structures. This simplified actantial model (Figure 1) was used to disentangle the users' and providers' perspectives and to suggest an action-oriented supplement to the more “one-dimensional” and descriptive three delays model. Ethical considerations: The study had ethical clearance from the National Institute of Medical Research in Dar es-Salaam. All participants gave informed consent prior to inclusion. It was made clear that participation was voluntary and could be interrupted upon request with no consequences for further care and that anonymity would be maintained. Results Findings will be presented in three main themes corresponding to the three steps in the “three delay” model: 1) Decisions to attend to health care, 2) Access to health care, and 3) Care needed for a safe birth, followed by 4) Suggestions for improving maternal health care. The users' perspective will be presented in most detail followed by the deviating aspects of the health professionals' perspectives. Informant codes are related to place of delivery and informants as follows; “BHF” is short for “Bugabo Health Facility”, “KRH” for “Kagera Regional Hospital” and “BHD” for “Bugabo Home Delivery”. “User” means the woman that gave birth, “HP” is short for “Health Provider” and “TBA” for “Traditional Birth Attendant”. 1. Decisions to attend to health care Women usually did not decide alone when and where to seek care. They followed advice from more experienced family members like the mother in law, a sister, a TBA and health professionals. The husband had a major role in the decision as he usually was the one holding the money needed to pay for transport and food. “The wife and the husband both decide. There are some husbands that never care, they just say; 'you decide where to give birth'. But those husbands who are concerned, they just arrange together” (BHDUser10). The most often mentioned factors influencing the decisions were perceived quality of care and the closeness to the support from relatives (Table 1). Perceived quality of care Women's decision of place of delivery was often influenced by perceived quality of care: “To be delivered by the TBA is not good, they induce native drugs, they can cause the death of the mother and even the baby. TBAs are not experts, their skills are very low. It is better to find the money and go to the hospital” (KRHUser8). No one questioned the skills of the health professionals but most users perceived the village-based health facilities to be incapable of managing complications at birth: “A woman in labour may attend the health centre or dispensary, but later she needs to go to the hospital. They can't do much. … It happens sometimes when people reach the health facility, especially during the night, the clinical officer or nurse tells them to wait until the morning. So the patient can be left with no care for six hours, they may die” (KRHUser2 Husband). Some users were not convinced that giving birth at home with TBAs was less safe than at a health facility: “It has been reported that maternal deaths happen even in the hospital. So it is not because the mothers are attended by the TBA [that women die]. They don't receive enough care at the hospital. The health providers they are not always close to the mother, the mother may request to be examined, but they just say; 'it is not the time for you, it is not yet'. She may bleed without anybody noticing it. But the TBA is always close to her, when she is requesting to come and see she is always available close-by, she may detect any changes that occur. I hear people talking that many women die at the hospital. Especially those who are not well experienced in service, the health providers, when they are called, they say; 'the time is not ready to push. Don't disturb me; we were not together when you conceived'” (BHDUser9). Being close to support from relatives Being near to relatives was mentioned by most users as a factor influencing decisions of health care attendance. Awoman pregnant for her first time living in the town with her husband went to the village to give birth at the small dispensary because she needed to be close to the care of the husband's mother and sister: “Being with your family you can explain any pain you have to them, your relatives are there to give you encouragements, being alone with a nurse in case of complications during delivery it will be difficult to handle. Your relatives are there to take care, being with them you feel comfortable“ (BHFUser1sisterinlaw). Gender roles No women reported to have been directly prevented from attending health facilities by their husbands. Some women were not living with a husband or their husband did not provide sufficient money. “If the husband can't fulfil his duties the pregnant woman is supposed by all means to prepare herself. … she is supposed to go to people who are able to help her either to plant something or to dig for them so that they could pay her. She has to save that money. It is not easy to keep it in the house. Because of the husband, those who are drinking alcohol, he may find that money and use it, so you have to keep it away from home. I looked for a trusted friend” (BHDUser2). Culture The health professionals often referred to 'culture' as the cause for women not attending maternal health care. A conflict between traditional beliefs and modern medicine was not found in the interviews with users. The health professionals considered the local drugs used by the women to cause complications: “The local drugs are dangerous, if they stimulate the uterus and they get repeated contractions, they can rupture the uterus, the babies can get fetal distress. ... We recommend them not to take these drugs but most do“ (KRHHP4). Negligence and ignorance Health professionals often felt that people did not follow advice because of negligence. This was not reflected in the interviews with the users; they were all concerned with the wellbeing of both the pregnant woman and her child: “To us they say yes, we will do this and this, but when they go to the village they drink this brew and talk about us two in the clinic saying; 'this is nonsense', they are not educated enough, you talk about this, they change it!! People neglect things, you talk, they neglect, we talk, we can't stop talking, we talk until they understand” (BHFHP5). Another explanation for poor compliance often mentioned by health professionals was that people in the village were “ignorant”. This was in contrast to the interviews with the users; they all knew of dangers like bleeding, fever and prolonged labor and generally mentioned the referral hospital as the place where the complications could be managed most safely. 2. Access to health care The access to health facilities was influenced by distance, availability of means of transport and costs. Travel at night was difficult, women were afraid of thieves and wild animals and it could be difficult to find a car to go to the hospital. Nevertheless, at all births observed where a woman or her newborn suffered complications they reached the health facilities, in most cases the hospital. Distance and transport means The first distance to cover for a woman in labour was from home to the peripheral health facility. A husband to a woman who ended having a home birth told the following: “I had to run to the neighbour to see if I could get a bicycle. But he was not around, so I had to run more and I saw my friend with a motorcycle, I requested him to take my wife but he said; 'I have not enough fuel to Kashozi'. I had to return back, I was afraid thinking; 'my wife is going to die'. I haven't seen her giving birth at home. So, while running I met with another friend who had a bicycle and I requested the bicycle. He said; 'I am running to the shop and then I will be back in few minutes'. When I came home I found my wife was just trying to push, I just passed the eye and saw something swelling. I didn't wait to see if it was the baby or not, I had to run, thinking where to run to the neighbour thinking that; 'my wife is dying', thinking of the mother who can help, one woman nearby, I had to run to her” (BHDUser4Husband). Costs In case of complications the more important access barrier was met after having reached the village based health facilities. Accessing the hospital in Bukoba implied costs that were a hindrance to many: “My sister lost her baby while giving birth because her husband had no money, he was not cooperative. She asked him to come to the hospital, he said; 'no, you will be at the dispensary'. At the dispensary they failed. Then when they told him to find a transport for her to come to the hospital, he said he had no money, so he left her there, went home. (…) and she ended with a dead baby” (KRHUser2). In the survey of 1123 women delivered at Kagera Regional Hospital the average expenditure in relation to pregnancy and childbirth were around 19000 TZS (16 USD). Expenses for transport were on average 26% of the total expenses but in cases of emergencies the cost could be 15000-50000 TZS (12-40 USD) or more (Table 2). The health professionals were aware of the difficulties in accessing the hospital: “I think there is a poor reference system in Bugabo. Those who come are already pale from the loss of blood. Mostly we receive the mother five minutes before they die while we take the cross-match for blood. I have seen one woman from Bugabo, the health centre referred her to the hospital, but because she had no money the husband referred her to the TBA instead. The TBA also failed and in a late stage they referred the mother to the government hospital” (KRHHP6). 3. Care needed for a safe birth. It is remarkable that only few informants mentioned maternal health when asked to list the most important health problems in the area. It was not because pregnancy and childbirth were not considered dangerous. But these dangers were not seen as isolated problems. A birth was considered as “good” when the mother and newborn survived and got home safe. At the same time most families were facing multiple other problems related to poverty and had to think of assuring sufficient resources for all its members to survive in the time after the birth . Care during pregnancy During pregnancy women tried to prevent problems by seeking care from different available sources. The ANC was considered important but many did not know what the drugs they received were good for. Most women consulted a TBA during the pregnancy for reassurance. The relatives were supposed to help her in the daily work with the heavy duties like fetching water and digging the shamba and also to help her follow the advice from the TBA or the antenatal clinic. The husband was responsible for saving money for transport in case of complications and for providing good food. All 31 women had taken local herbal medicine during pregnancy; some got it from TBAs, some from relatives and some knew where to find it themselves. These drugs were considered important to give strength and to prevent and treat maternal and neonatal complications: “Those drugs are to be given early in the pregnancy, they prevent the mother from having much fluids, prevent malaria to the mother and the fetus, prevent the mother from having bleeding after delivery, even these convulsions of the fetus after birth, and HIV. She is supposed to continue until after the birth, until the baby starts to smile.” (KRHUser2Husband). The health professionals strongly believed that if women attended ANC early and frequently, a large share of complications could be avoided: “I wish to see a pregnant woman as soon as she feels she is pregnant but they come with pregnancies starting at 5, 6, 7 months, that is too late. The ANC services start at when? Even before the woman is not pregnant yet. At least I would like them to attend ANC from at least 8 weeks, if we have a chance to identify the pregnancy that early then I think this lady has a chance to receive a good health service” (BHFHP7). Care during birth During birth the most important person for the woman was the birth attendant who should be closeby: “Thinking of the providers not being nearby makes me feel not giving birth at the hospital” (BHDUser10), “The TBAs are good because they are always close to the mother. They can easily detect the time when she are ready to push. But being at the hospital with the shouting and telling without examining; 'you are not ready yet'. So the TBAs are better than the nurses, being close all the time, not shouting” (BHDUser11). Also important was that the birth attendant was an 'expert' and knew how to manage complications. Most considered the health professionals at the hospital to have the highest expertise: “Being in the hospital, when I take my wife there, I am very, very satisfied of the care she is receiving. I don't feel afraid when the mother is with the staff within the hospital. Because in case of any problems they easily detect and they know much concerning conducting deliveries” (BHDUser4Husband) The health professionals were aware of the difficulties managing women with complications at the village health facilities: “We have only one delivery kit, small size, there is one forceps, two artery forceps, one scissors, one apron. A well equipped delivery kit can really help the mother to deliver. The catheter is missing. The glass for the kerosene lamp is broken” (BHFHP5). Even at Kagera Regional Hospital there were often delays in emergency obstetric care, especially at night when the doctor was on call from home. One nurse said: “If you have an emergency you have to find the supervisor, she has to find the doctor; maybe the doctor is at home at that time. So getting the doctor is sometimes postponed. You pray to God. You have to pick up all the staffs from different places. Getting the staffs there can take a long time. It is so painful. These doctors on call should be present at the hospital; you find that at other hospitals” (KRHHP7). Care after birth After birth the care from relatives was considered very important: “If you have a good birth with no problem, you need care after birth to buy soup, meat, sugar and other things” (BHDUser3Husband). “When there is a failure of care after birth, she doesn't receive good care it can cause her to die” (BHDUser5Husband). 4. Suggestions to improve maternal health care When asked to suggest how maternal health care could be improved the users repeatedly mentioned the need to strengthen the services at the village health facilities: “If it was possible to allocate in the village a doctor or midwife to conduct the deliveries. Because in the past we had TBAs, but now they are prohibited, so it is better to allocate doctors within the village because it is so expensive for the transport” (BHDUser7 Husband). “If it could be possible that every health facility has supplies and enough intra venous fluids. In case the mother has severe bleeding, she needs to be given more blood. So it could be better, if they could do it, could repair her here, and not to send her to the big hospital. Or if not that, transport must be available all the time” (BHFUser1). The health professionals were aware of the difficulties related to providing safe delivery care. Nevertheless, suggestions to prevent maternal deaths had a clear focus on the need to 'change the attitude of the community', described by some as a 'battle': “We are not big enough to attack the community, so that we talk and they understand” (BHFHP5). Home deliveries were considered to be the main cause of maternal deaths by health providers: “Even one home delivery I don't like. When somebody is telling me about a home delivery it is like delivering close to the grave. If I hear someone is delivered at home, I think even she lives today, tomorrow she is dead because she is not aware of the hazards of delivering with no skilled assistance. They tell me they gave birth on the way but they went to the TBA. But they think that I will take the TBA to the court if they tell” (BHFHP7). A practice had emerged that women who gave birth at home had to pay a 'fine' of 5000 TZS (4 USD), otherwise their newborn child would not be registered and vaccinated. Furthermore TBAs were threatened with imprisonment if they conducted deliveries at home. Discussion The users' perspective on the challenges of surviving childbirth did not in all aspects fit into the three delays model. Furthermore, the differences in the user and professional perspectives were difficult to embrace in the model at the same time. Most important for the users when making decisions about where to give birth was the perceived quality of care and being close to relatives. Not only 'expert' care was considered but also the 'closeness' of the care. After birth, the care from relatives was needed for the safety of the mother and baby. The health professionals did not see the relatives and the community as an important and helpful resource. They blamed cultural barriers, gender roles, ignorance and negligence to negatively influence women's attendance to delivery care. The importance of being close to the relatives could be categorized as a 'first delay' in the community, but this would considerably devaluate the positive quality attributed by the women. Delays within the health facilities was a major problem reported by informants and observed by the primary investigator. The peripheral health facilities in Bugabo were unable to safely manage obstetric and neonatal complications. The most important transport barrier to women suffering obstetric complications was met after reaching the health system as referral to the hospital was costly and transport not always available. The women and their relatives did not see the problems of pregnancy and birth in isolation but in relation to the other multiple problems they face in the context of poverty; the overarching theme in the interviews. For the users the story was not over at the health facility. They had to get back to the family with enough resources for themselves, the newborn and the rest of the family to survive. They suggested upgrading village health facilities to provide EmOC as the most important step to reduce maternal deaths. Even though health professionals were aware of the problems relating to poor quality of care and transport they still blamed the community as the main barrier to improve maternal health. In this way the three delays model gave room for health professionals to flee from responsibility leaving the important problems unsolved. Many studies of delays in EmOC has as a framework the three delays model and point towards community interventions for reducing maternal deaths without discussing if such interventions are reasonable or feasible25-28. One literature review concludes that innovative strategies are needed 'to bring the poor closer to obstetric care'29. A survey from Southern Tanzania found the quality of care at facility deliveries too low but contradictory suggests a need for education of women and men to 'raise awareness'30. A study from Uganda found 'cultural barriers' and 'adherence to traditional birthing practices and beliefs' to be the main causes of maternal deaths even though many users reported poor care at health facilities 31. A recent review concluded that surveys of determinants for attending institutional deliveries almost never looked at quality of care32 . A study from Tanzania combining qualitative methods with a survey of 21.600 households concluded that perceived quality of care and costs are main determinants for choosing place of delivery13. Other studies likewise emphasize the importance of users' perceived quality of care10,11 including the users' non-medical concepts19. Only few of the numerous studies using the three delays model as a framework focus on the actual quality of EmOC care provided by the health system. A qualitative study from Gambia's main referral hospital reported substantial barriers to EmOC within the hospital “related to inadequacies resulting from a plethora of shortages”14. An 'audit' of 129 health facilities in rural Northern Tanzania concluded 'that it is neither the mothers' ignorance nor their lack of ability to get to a facility that is the main barrier to receiving quality care when needed, but rather the lack of quality care at the facility”33. Interventions that effectively reduced maternal mortality have all had as a focus the strengthening of health systems to provide good quality EmOC34. At Kigoma Regional Hospital region in Western Tanzania the maternal mortality was reduced by two thirds over six years after EmOC was improved by low- or no-cost interventions35 . A similar intervention in Mali resulted in a 50% reduction in maternal mortality over four years36. An important question is if the three delays model leaves too much room for interpretation. Even the very simple MDG 5 of '90% skilled attended deliveries' was in the present study translated by health professional into a focus on the '90%' rather than the quality of 'skilled attendance'. The recent 'road map' from the Tanzanian Ministry of Health to reduce maternal deaths unfolds the three delays framework into hundreds of specific aims. Only few of these concern EmOC with the target that it should be provided at 70% of peripheral health facilities by 2015. In the light of the findings of the present study these aspirations seem difficult to realize37. There is a need to consider an alternative to the three delays model that clearly maps the agents, means, obstacles and needed actions towards the aim: to bring good quality emergency obstetric care as close as possible to where women live. The actantial model is useful to disentangle the perspectives of users and health professionals and makes clear the important points; what should be moved towards what aim against what obstacles and with what help available? For the users the aim was to get the women and baby safely home after birth and still have sufficient economic means for the survival of the whole family. The women sought available help from health facilities, relatives and TBAs. Opponents to these aims were often beyond the control of the women and their families. The MDG5 was, as it was translated by the health professionals as a 'battle against the community', another opponent for women and their families in their struggle to survive. A number of homebirths would inevitably happen in the context of poverty where sparse resources have to be spent carefully (Figure 2). The health professionals' aim was development as stated in the MDG5: to get women to give birth at the health facility. Relatives and TBAs, were seen as representatives of backwardness opposing development, and their importance for the women was not recognized. Health professionals were aware that they had no or limited ability to act in case of emergencies as was also observed by the primary investigator. They strongly believed in their ability to prevent complications from happening by antenatal care and other preventive measures. The literature has described prevention of complications as an ineffective strategy and that emergency obstetric care is the core service needed to reduce maternal mortality. In that light the health professionals were performing a 'symbolic ritual' with 'modern artefacts' to manifest professional status and power rather than providing effective care and assuring safe births. The health professionals blamed the users as responsible for maternal complications. In contrast, the users did not blame the health professionals for poor performance or lack of skills. This could indicate that the health professionals found themselves under pressure without the means needed for solutions. They had to place responsibility somewhere else. The health professionals were poor in more than one sense; they were assigned a task they were not able to fulfil, they had poor backup from their superiors and they were not really part of the community where they worked. They had their professional status at stake, losing that would isolate them even more. Under these conditions they were not able to point at feasible solutions to reduce the risk of maternal deaths (Figure 3). The earlier mentioned interventions that effectively reduced maternal mortality all had the focus on strengthening health systems and improving the quality of EmOC. Therefore the authors of this paper suggest an actantial model with the health system as the subject as the most likely model to point towards feasible strategies to reduce maternal mortality. While the responsibility for providing adequate health services should be within the health system, the care should be 'patient-centred', meaning that it should be organized in a way so it is accessible and acceptable to the users of the health services. Regarding maternal health the aim should be to move good quality EmOC close to where the women live. A wrong focus on community instead of health system barriers to EmOC is a main obstacle to reach that aim. Another obstacle seems to be lack of resources, lack of skills and poor political commitment (Figure 4). Limitations to the study apply to the nature of this exploratory field study. The main aim was to stimulate reflections on present and future strategies to reduce maternal mortality in the developing world. It builds on fairly solid and systematically collected empirical findings discussed and compared with relevant literature. The validity and generalisability can be discussed. No stories are neutral. In a conversation all participants have a perspective and a purpose of partaking. The information given will be shaped by the intentions and worries of informants in a process where the interviewer has an influential and active part to play. The answers given by informants were inevitably influenced by being interviewed by a male, European doctor, likely to be attributed high authority and power. The interviews with the users generally felt surprisingly 'unproblematic'. It must be noted though that conflicting information was given by users in relation to home births. Three out of 11 women claimed to have given birth 'on the way to the health facility'. This was in all three cases contradicted by their husbands and by TBAs that told that the birth had taken place with the help of the TBA in her house. When interviewing health professionals the atmosphere was more often influenced by an atmosphere of anxiety, something was at stake and answers seemed to be carefully considered before given. This situation changed somehow over time as the health professionals gradually accepted the PI as a 'collegue' with no threatening intentions. The reliability of data is always to some extent influenced by being translated and later transcribed. Non-verbal language and nuances in the conversation like intonation and breaks are lost in the process. Conclusions Health providers and planners as well as politicians and donors need to recognize that the responsibility for reducing maternal deaths lies within the health system. Home deliveries and women arriving late at health facilities will continue in a context pervaded by poverty. Health professionals projecting their own incapability to the community is unjust and leave the central problems unsolved. Forcing more women into already overburdened health facilities that do not provide safe births is a hazardous and inefficient strategy. To reduce maternal deaths, health systems need to be strengthened so women can access emergency obstetric care in time. The quality of EmOC must be assured by sufficient supplies, staff, skills training, supervision and monitoring. The study demonstrates how the three delays model and the MDG5 does not satisfactorily identify and prioritize strategies to reduce maternal mortality. After 15 years as the implicit framework for research into delays in EmOC it seems time for a revised understanding of why women receive EmOC too late. This paper proposes a simplified actantial model with the health system as the point of departure. The focus should be shifted away from determinants of health care attendance in the community and into how to assure provision of good quality EmOC close to where women live. Future research should investigate how quality of care is assured and particularly explore the working conditions and working culture of health professionals and health planners. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11025f4.jpg] [rh11025f1.jpg] [rh11025f2.jpg] [rh11025t2.jpg] [rh11025t1.jpg] [rh11025f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}