 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 131-146 ORIGINAL RESEARCH ARTICLES Regional patterns and correlates of HIV voluntary counselling and testing among youths in Nigeria Chukwuemeka E. Nwachukwu1 , Clifford Odimegwu2 1Dept of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, South Africa 2Programme in Demography and Population Studies, School of Social Sciences University of the Witwatersrand, South Africa. Code Number: rh11026 Abstract Prevalence of Voluntary Counselling and Testing (VCT) for HIV among young people in Nigeria is low with implications on the epidemic control. Using the 2003 Nigerian National Demographic and Health Survey, we examined the regional prevalence, pattern and correlates of VCT for HIV among youths aged 15 to 24 in Nigeria. Analysis was based on 3573 (out of 11,050) observations using logistic regression model to estimate the effects of identified predictors of volunteering for HIV testing. Results show that national prevalence of VCT is low (2.6%) with regional variations. Generally, the critical factors associated with VCT uptake are age, sex, education, wealth index and risk perception with North (sex, education, religion, occupation and risk perception) and South (age and education) variance. It is recommended that Nigerian HIV programmers should introduce evidence based youth programmes to increase the uptake of VCT with differing approaches across the regions. Résumé La pr évalence du Conseil et du Testing Volontaire (CTV) pour les jeunes gens au nigérian est base, ayant des implications pour le contrôle de l'épidémie. En nous servant de l'Enquête Nationale sur la Démographie et la Santé de 2003, nous avons examiné la prévalence régionale, les mod138les de corrélats du CTV pour le VIH chez les jeunes gens âgés de 15 à 24 ans au Nigéria. L'analyse a été basée sur 3573 (sur 11050) observations à l'aide d'un modèle de la régression logistique afin d'estimer les effets des indices identifiés pour se présenter pour le test du VIH. Les résultats ont montré que la prévalence nationale du CTV est basse (2,6%) avec des variations régionales. En général, les facteurs critiques qui sont liés à l'acceptation du CTV sont l'âge, le genre, l'éducation, l'indice de la richesse et la perception de risque avec la variance du nord (le genre, l'éducation, la religion, l'occupation et la perception de risque) et du sud (l'âge et l'éducation). Nous préconisons que les programmes nigérians du VIH introduisent des programmes des jeunes qui sont basés sur l'expérimentation afin d'augmenter l'acceptation du CTV fondées sur des approches différentes à travers les régions. Key words: Voluntary counselling and testing HIV/AIDS, Nigeria youths Introduction Human Immune-deficiency Virus (HIV) with resultant Acquired Immune Deficiency Syndrome (AIDS) is a global pandemic, reported in almost all the countries of the world. As at 2009, about 67% (22.5 million) of the infected people and 72% of the burden of death and 58% of new infections globally is in the sub-Saharan Africa1 . Incidence of HIV in the sub-Saharan Africa is highest among youths aged 1524 and who are also vulnerable to unsafe sex and sexual abuse. It is therefore important to target this group of people in HIV prevention and care strategies especially in developing countries. Various strategies to control HIV, especially among young people have been propagated. These include campaigns on safe sex, regular use of condom and Voluntary Counselling and Testing (VCT)2 . Knowledge of an individual's HIV status can potentially change sexual behavior through Counselling, early treatment, care and support. Nigeria is an African country with a serious HIV problem. Factors identified to have contributed to the spread of HIV in Nigeria are: low access to information and education on sexual health, stigma and discrimination, poor healthcare services, harmful marriage practices and sex work2 . People therefore ignorantly engage in risky sexual behaviors, shy away from using healthcare services to know their HIV status and in some cases; such services may not even be available and/or affordable. Nigeria is the most populous black nation with an estimated official population of 140 million3 as at 2006 and about 3.3 million people living with HIV/AIDS1. Despite its low adult HIV prevalence of 3.6%1, it ranks the third country in the world with the highest number of people living with HIV/AIDS. This has potential implications not just on Nigeria but also on the neighboring West African countries and the continent at large, if not controlled. The return of democracy in Nigeria in 1999 had opened doors to development of new strategies by government towards prevention, treatment, care and support for HIV/AIDS. This is evident in the setting up of the National Action Committee on AIDS (NACA) with states and local government committees and opening centers for Voluntary Counselling and Testing (VCT). Uptake of voluntary Counselling and testing services among young people in Nigeria is low, estimated at 10%4. Efforts to improve uptake seems to be slow despite good knowledge of HIV among the population. This study on regional patterns and correlates of voluntary Counselling and testing used secondary data from the Nigerian National Demographic and Health Survey (NDHS) 2003 which includes information from such variables that demographically characterized young people aged 15-24 and their attitudes and knowledge towards HIV and voluntary Counselling and testing. The purpose of this paper is to explore the prevalence and pattern of VCT uptake among youths in Nigeria, exploring the differences across the geopolitical zones, religions, etc. This will help further programme planning, policy and implementations of HIV prevention programmes in Nigeria. Background Information of Study Population Nigeria is in the West African sub-region and lies latitudinal from 4016' -13053' north and longitudinally from 2040' - 14041' east5 with a total surface area of 923,768 square kilometers. It shares boundaries with the Republics of Niger, Chad, Cameroon and Benin to the north, north-east, east and west respectively. The Atlantic Ocean borders the south of the country. The country has a tropical climate with dry season characterized by cold, dry and dusty harmattan occurring from October to March and worse in the north while the wet season occurs from April to September5 . Rainfall is as high as 2,600 milliliters in southeast and south south, giving rise to a mangrove swamp forest and as low as 600 milliliters in the north with Sahel grassland vegetation. Agriculture is the main source of livelihood for the vast majority of rural dwellers. Diverse kinds of crops produced across the country were a major source of foreign exchange earnings before the discovery of crude oil, which is now the mainstay of the economy. The country's healthcare system is structured to recognize Primary Health Care (PHC) as the pivot on which efforts to improve health care delivery will be hinged. The PHC services include health education, provision of portable water and good sanitation, reproductive health, immunization, control of diseases including prevention of HIV/AIDS and provision of essential drugs. Comprehensive health care facilities have been therefore established in various parts of the country, predominantly in the rural areas to achieve these objectives. There are, however, widespread differences in health care delivery across the regions due to differential availability of resources and distribution of service providers. With respect to HIV/AIDS, the National Action Committee on AIDS (NACA) was established in February, 2000 to coordinate all HIV/AIDS activities in Nigeria6 . Its aims are, among others, to coordinate, monitor and evaluate the implementation of the strategic national plan for the control of HIV/AIDS and present control plans to the Presidential Council on AIDS (PCA) for policy purposes. Educational system and literacy levels in Nigeria have evolved over time in an effort to build a sustainable manpower and human resources for its developing economy. Every child was given the right to a free and compulsory primary education by the Universal Primary education formulated in 19765. This has been aggressively followed by the National Literacy Program for Adults and Nomadic Education for the benefit of families that are migrant cattle rearers and fishermen in riverine areas. As a result of the literacy policy of the present democratic government formulated in October 1999 and christened Universal Basic Education (UBE), education is presently free up to junior secondary school. Education facilities and teachers are, however, not equitably distributed across the regions in the country7 , which also reflects in enrolments and the declining quality of education in Nigeria. Problem Statement HIV voluntary Counselling and testing is an effective strategy in reducing the transmission rate of HIV especially among young people2, 8 . There are limited studies assessing the regional variations in the uptake of HIV testing in Nigeria. However, some studies have shown that despite high knowledge of HIV, VCT uptake is low 4, 9. The NDHS (2003) reported that only about 10% of Nigerian youths had ever been tested for HIV, but it does not provide information on regional variations. Understanding regional patterns and differentials in voluntary Counselling and testing is important for designing effective strategies to increase VCT uptake. For example, effective Counselling and testing for HIV will help in identifying those at risk and promote behavior change strategies which will minimize the spread of HIV and sustain good quality of life for infected individuals. Studies on Voluntary Counselling and Testing (VCT) for HIV in Nigeria have reported largely on a highly selective group of people and within localities such as in pregnant women and undergraduates4, 9, both in Oyo state (South West region). These studies do not reflect the true measure of VCT uptake in the country and provide a poor indicator of how youths are using VCT services. In other African countries such as Kenya and Uganda, VCT uptake among youths is high and serves as a potential tool for monitoring the progress of HIV control programs8 . Given Nigeria's ethnic diversities and cultural complexities, understanding the regional variations in VCT service utilization will help to design more specific programs to promote access and use of VCT services by young people. There is therefore the need to examine the prevalence, patterns and correlates of VCT uptake among youths in Nigeria. This study will provide valuable information to strengthen existing national HIV/AIDS control/prevention policies and programs on VCT in Nigeria. Literature Review Voluntary Counselling and Testing (VCT) is the process of providing Counselling to an individual to enable him/her to make an informed choice about being tested for HIV infection. This decision must be entirely the choice of the individual, and he/she must be assured that the process will be confidential 10. VCT is an emerging HIV prevention strategy in Nigeria. It is an entry point to medical, social, preventive and therapeutic interventions in the control of HIV/AIDS. It facilitates behavior change promotion through Counselling to those who test negative and provides an early cache for care, support, treatment and other social interventions for those who test positive2. Assessing the spread and prevalence of HIV voluntary Counselling and testing will help in developing programs that will create demand and increase the interest of young people to receive Counselling and get tested for HIV. For example, surveys conducted in many African countries like Ghana, Kenya and Burkina Faso in 2003 reported that only an average of 8% of young people (aged 15-24) who had had sex in the past 12 months had tested for HIV. Uptake was higher in males than in females, and this result was consistent in all the countries surveyed 11 . There are few epidemiological studies assessing the uptake and regional prevalence of HIV VCT in Nigeria. Literature search conducted in Medline through Pubmed and various journal portals in the health sciences library of the University of Witwatersrand yielded few studies on VCT in Nigeria. These are localized studies and do not reflect Nigeria's geo-cultural complexities. A study conducted in the South Western Nigeria9 among 804 women attending antenatal clinics showed that about 70% of respondents were ignorant of voluntary Counselling and testing, however, 89% of this expressed willingness to be tested after information on VCT was provided. Uptake of VCT among this group was 6.0% despite a high HIV knowledge (84%). Those who volunteered for VCT had more education (P<0.05) and higher HIV knowledge score than those who did not. Respondents who did not volunteer cited the fear of social stigmatization and rejection. Similarly, among male undergraduate students, Adewole et al reported a low uptake of 8.3%. Those who volunteered had higher knowledge scores for HIV (P=0.006), parents in the higher socioeconomic class (P<0.00001) and mothers who had completed secondary education (P=0.02). Another study among undergraduates reported an 11.9% VCT uptake12 . In this study, respondents' attitudes toward VCT were largely influenced by stigma and fear of discrimination. Opeyemi 13 reported psychosocial factors, consistent among both sexes as critical factors preventing in-school adolescents in Ibadan, Nigeria from volunteering for HIV testing. The only national study which provides a national rate for VCT uptake is the 2003 NDHS. The focus of the survey, however, was not on VCT. The report showed that an average of 10% of young people aged 15 to 24 (6% of women and 14% of men) had ever been tested and received the results of their HIV test 5. A hospital-based study in Northern Nigeria among patients aged between 24 and 45 showed a high uptake (88.3%), a result expected for ill patients 14. Illiyasu et al reported that reasons for avoiding VCT in Nigeria include fear of stigmatization and isolation and effect on marriage security15. On the other hand, Solomon et al reported possible reasons for seeking VCT in developing countries to include engagement in risk behaviors, developing suspicious symptoms, having a HIV-positive partner and following up on a previously negative test16. Studies in other countries show low VCT uptake. In Malawi, degraft-Johnson et al,17 reported a 9% uptake, and in Norway, Fylkesnes and Siziya reported an 11.8% uptake18 . A population survey in South Africa showed VCT uptake to be positively associated with age, education, socio-economic status, living close to the clinic and low perception of stigma19. The main reasons for seeking VCT included perceived risk of HIV infection and self reported decline in health status. A health facility based study in Uganda 20 conducted among pregnant women mostly aged 15 – 24 reported a 73% willingness to use VCT services. Utilization was however poor due to inability to afford the test, fear of knowing the result, stigma, attitudes of health workers and refusal of their partners to take an HIV test. Another household survey in Uganda among pregnant women aged 18 and above showed a 10% uptake of VCT, largely hindered by unavailability of VCT service centers, lack of Counselling and perceived lack of benefits to mothers and their infants21. Testing was associated with being a primigravida (OR 2.6, 95% CI 1.2–5.8), urban residence (OR 2.7, 95% CI 1.3–5.8) and experience of Counselling before and after testing (OR 6.2, 95% CI 2.9–13.2). The studies reporting on VCT in Nigeria lack detailed analysis and thus limit their utilization. Planning and implementation of HIV prevention strategies will also be impaired if data is not available to evaluate successes and deficiencies in the regional and national programs for HIV prevention, especially as VCT is an integral strategy linking prevention, care and support. This study, therefore, seeks to examine the regional prevalence, patterns and correlates of voluntary Counselling and testing for HIV among the Nigerian youths. Research Hypothesis The hypotheses to be tested are:
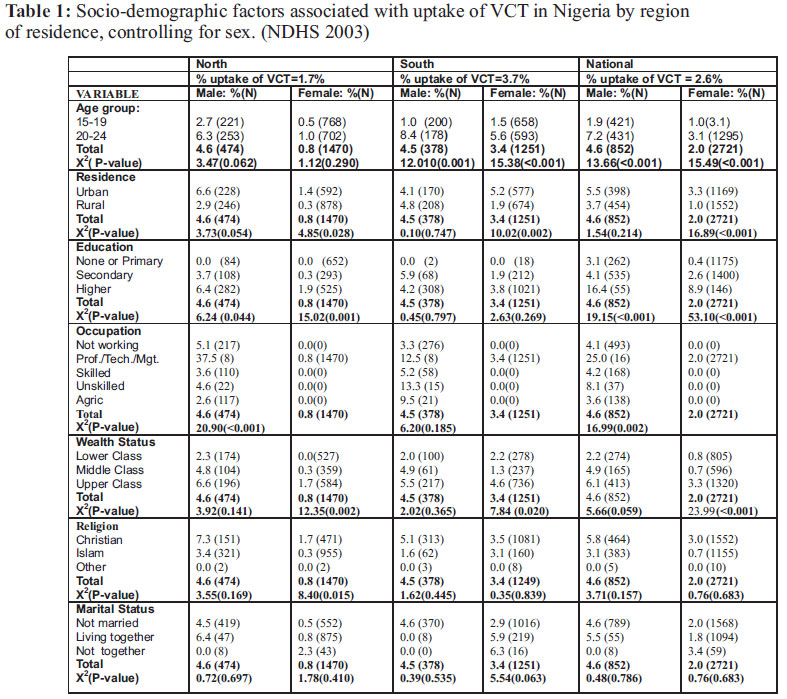
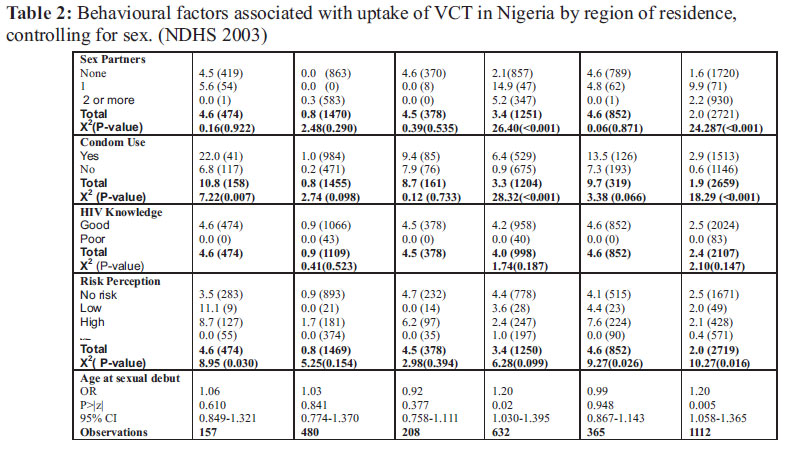
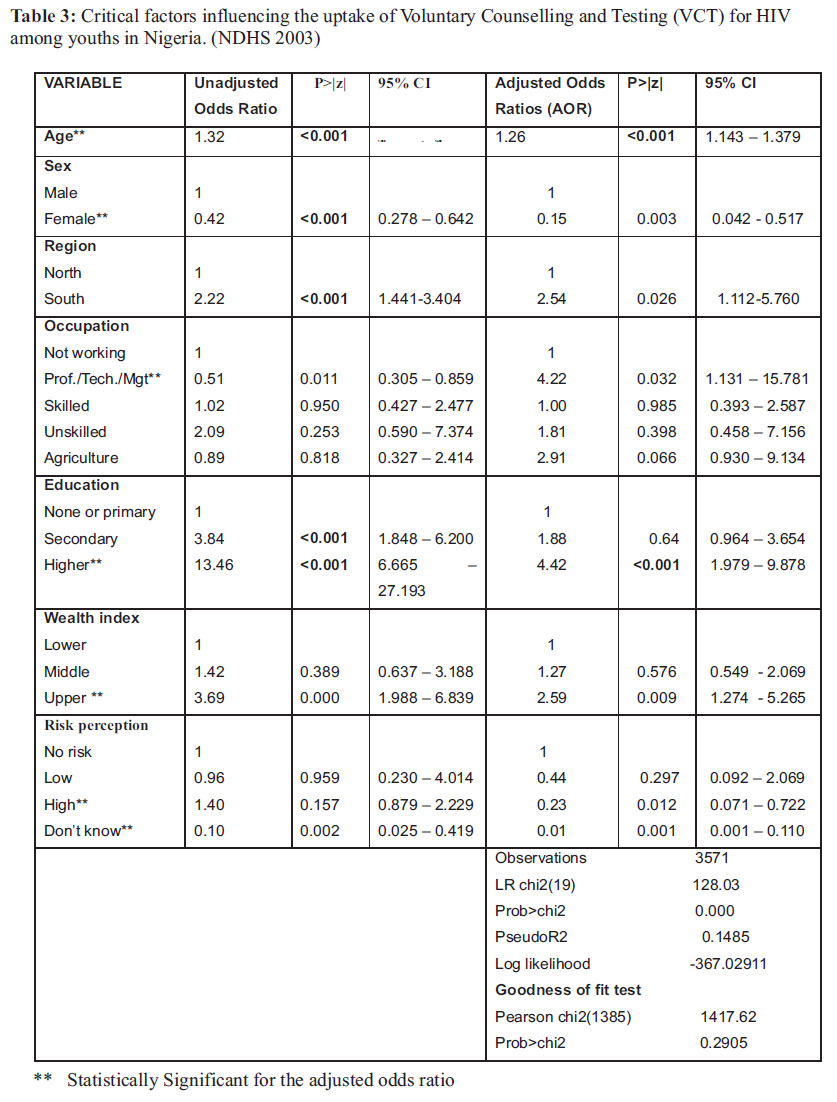
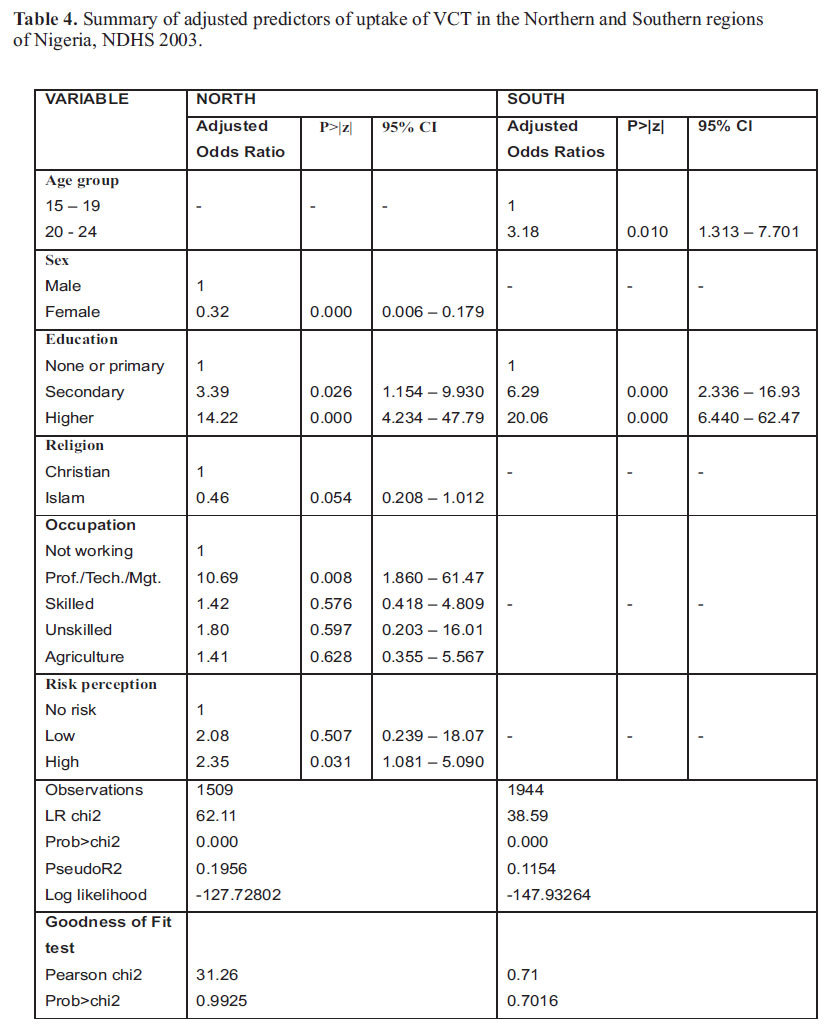
Methodology Study Design This study is a secondary data analysis using dataset from the Nigeria National Demographic and Health Survey (NDHS) of 2003. The 2003 NDHS is the third nationally representative survey in Nigeria, designed to collect data and provide information on various health issues such as fertility, family planning, maternal and child health, HIV/AIDS. This is to guide policy makers, health program managers and researchers in planning, implementation, monitoring and evaluation of population and health programs to improve health services in Nigeria. The full report of the 2003 NDHS contains the details of the methodology used in the survey, which is summarized below. The 2003 NDHS was sampled to provide estimates of population and various health indicators with urban and rural differentials for the six geopolitical zones and the country at large. The survey used a stratified, multi stage sampling method with the list of enumeration areas (EA) developed for the 1991 national population census in Nigeria as a sample frame. The EAs are grouped by states, local government areas (LGA) within a state and localities within LGAs. The EAs were first stratified by urban and rural areas with localities less than 20,000 in population constituting a rural area. The primary sampling units (PSU) were clusters defined as consisting of one or more EAs such that each cluster contained a minimum of fifty (50) households. In the sampling, three hundred and sixty five (365) clusters were first randomly selected, 165 in urban and 200 in rural areas. Then households were systematically selected for participation in the survey. A nationally representative probability sample of 7,864 households was eventually selected with estimates based on the response rate of the 1999 NDHS. This produced 11, 050 respondents as all eligible women aged 15 to 49 in every household and eligible men aged 15 to 59 in every third household were interviewed6. Response rate was 99% of households, 95% of eligible women and 91% of eligible men. Data for the 2003 NDHS was collected with questionnaires adapted from the model developed by the MEASURE DHS+ program during a technical workshop organized by the National Population Commission and attended by experts from governmental and non-governmental organizations and international donors. Three questionnaires – household, men and women questionnaires were translated into the three major languages (Igbo, Hausa and Yoruba) and pre-tested in November 2002. The household questionnaires contained information on household's dwellings and ownership of facilities but was mainly used to identify eligible men and women for individual interviews. The men and women questionnaires were then used to collected information from eligible men aged 15 to 59 in every third household and women aged 15 to 49 in every household respectively. Study Population The 2003 NDHS interviewed eligible men aged 15 to 59 and women aged 15 to 49 from sampled households in Nigeria. This study involved analysis of data from both male and female participants aged 15-24 in 2003, spread across the regions and who were interviewed in the 2003 NDHS. This sample was selected because the study is focused on youths and therefore extracted data on all respondents aged 15-24. Sample Size The 2003 NDHS sampling targeted 7,864 households to interview about 11,050 people, 8,250 women aged 15 to 49 and 2,800 men aged 15-59. A total of 7,985 women and 2,572 men were identified on the households for interview but 7,586 women and 2,340 men were successfully interviewed giving a total sample size of 9,927. Young people aged 15 to 24 make up 36% of men aged 15 to 59 and 41% of women aged 15 to 49 from the Nigerian census of 199122 . Therefore the effective sample size for this study will be approximately 4,000, calculated from the total sample in the NDHS. This corresponds with the sample size of 4,107 found in the dataset. Data Source Written permission was obtained from ORC Macro (who provided technical support to the survey), through the MEASURES DHS+ project, to use the data from the 2003 Nigerian demographic and health survey. Data was then downloaded from the measuresdhs dataset site in the rectangular file format and opened with the Statistical Package for Social Scientists (SPSS) version 10, which was its original software store. A set of twenty six (26) identical variables was selected from the files containing the men and women data and saved in Microsoft excel from Microsoft Office 2000. The datasets were merged, the variables renamed and sex variable added in excel as well as selection of a subset of respondents aged 15 to 24 according to the objectives of this study resulting to four thousand one hundred and seven (4107) observations. It was then transferred from excel to Stata Release 9.0 for analysis. However, the derived outcome variable, voluntary Counselling and testing (VCT) appeared in 3573 observations. This is the number of respondents who responded to the question if they have ever been tested for HIV. Five hundred and thirty four (534) observations from the explanatory variables were therefore excluded to account for this difference and other variables with incomplete responses. Ethical Consideration The study analyzed secondary data whose report is already published and data available in the public domain with no link to individuals. It therefore has no risk of undue disclosure and other ethical considerations. The protocol was also presented to the university of the Witwatersrand ethics committee, which gave unconditional approval for the study (protocol number: m060917). Data Analysis: The data was analyzed using STATA 9. This software was preferred because the researcher is more familiar with it and feels that it is easier to manipulate than other common software. To make analysis and interpretation simpler and more meaningful, some variables were regrouped from their original categories in the dataset. Some of those are: Region regrouped into North (North East, North Central and North West) and South (South East, South South and South West); Marital status was also regrouped into never married, living together (comprising of married and living together to reflect any form of union) and not living together (comprising widowed, divorced and not living together). Wealth index was constructed from information on surveyed households' ownership of assets such as television, radio, bicycle, car and characteristics of the dwelling such as source of drinking water, sanitation facilities, type of materials used on the roof and floor, etc. Each asset was then assigned a weight (factor score) generated through principal component analysis and standardized23. The scores for each asset were summed for each household and the individuals were classified according to their households. The sample was then divided into quintiles from one (lowest) to five (highest)6 . For the purpose of this study, wealth index was re-categorized into lower (comprising classes poorest and poorer), middle and Higher (comprising richer and richest). Number of sexual partners, which was originally a continuous variable, was also categorized into none, 1, 2+. This grouping made it easier to compare the influence of increasing number of partners to those not having partners and their uptake of voluntary Counselling and testing (VCT) for HIV. Data were analyzed at three levels, including stratification by sex to explore the effect of the difference in the sample size between males and females. The first was the univariate analysis of the baseline demographic and socio-economic characteristics of participants and prevalence rates of HIV VCT according to their region of residence. These were tabulated in proportions to show national figures and regional differences. Continuous variables were presented as means and standard deviation. There was then a bivariate analysis to examine all the explanatory variables for significant association with uptake of VCT for HIV using cross tabulations and univariate logistic regressions. Finally, multiple regression analyses were done by automatic stepwise selection of the variables associated with uptake of VCT. The data was first set to be a survey data in STATA, to account for possible inter cluster differences due to the sampling method used in the survey. Logistic regression model was then fitted using the selected variables, exploring for interaction among the variables. This was used to determine which variables are significantly associated with uptake of VCT as well as adjusting for potential confounders and presented as adjusted odds ratios with corresponding p-values and 95% confidence intervals. Logistic regression model was chosen because the outcome variable is binary (VCT -yes or no). A logistic regression model gives the probability that the outcome occurs as an exponential function of the independent variables. The basic logistic regression equation for the independent variables is thus: Logit (p) = + 1X1 + 2X2 + …+ iXi , where logit (p) is the log of the odds that the dependent variable is 1, is intercept and 1, 2, … I are the regression coefficients24 . Each analysis was done at national level and later controlled by the regions, north and south. Results A total of 3573 respondents aged 15-24 were included in the analysis. Tables 1 and 2 show variations in the socio-demographic and behavioural characteristics of the respondents by their region of residence. Regional distributions of the respondents are: 1944 (54.4%) North and 1629 (45.6%) South. Fifty two percent of the respondents were 15 – 19 years old while 58% were aged 20 – 24 years which are the average figures for all the regions. There are 76% percent of female respondents and 24% of males. This is because the NDHS purposively sampled more women than men to get enough information on reproductive and child health issues. Also 56 percent were interviewed in the rural areas while 44 percent are urban dwellers. There is a higher percentage of Moslems in the Northern regions with Christians dominating the South. A large percentage of the respondents are working as professionals or in the technical/management positions (77%) while about 14% are not working. More than half of the respondents (66%) are not married while 32% are either married or are living with a partner. There is a higher percentage of those who are married and /or living together in the Northern region than in the South. Educational level of respondents varies by regions also. A good fraction of the respondents occupy the high wealth index class (49%) with 30% in the low class and 21% in the middle class. Only 2.6% of all respondents had ever volunteered for HIV Counselling and testing. Uptake is higher in the South (3.7%) than the North (1.7%). However the 2003 NDHS reported a prevalence of HIV testing of 10% among Nigerian youths. This is inclusive of those who tested voluntarily, those to whom testing was offered and they accepted and those who for one reason or the other required HIV testing. There is more uptake of VCT in the Southern than in the Northern Nigeria. The result also show that males (7.2%) were more likely to volunteer for HIV Counselling and Testing than females of the same age group (3.1%) which is consistent in all the zones. Expectedly, urban dwellers had higher VCT uptake (males=5.5%) than rural dwellers (males=3.7%); a result also consistent among females and within the zones. There is a higher uptake of VCT with increasing education of the respondents, those in the professional occupational group and among the upper wealth class. Christians (males=5.8%) and those who used condoms in their last sexual act before the survey (males=13.5%) were also more likely to uptake VCT compared to Moslems (males=3.1%) and those who did not use condom (males=7.3%) respectively. This same result is also seen among those who have good knowledge of HIV and those who reported high risk perception for HIV infection. Multivariate Analysis In order to identify critical factors influencing the uptake of VCT for HIV among Nigerian youths, all the variables found to be associated with it were used in an automatic stepwise selection analysis. Variables selected were age, sex, region, occupation, education, wealth index and risk-perception though it varied when stratified by region and sex (Table 3). The regions were stratified into the northern and southern regions for the purpose of this multivariate analysis. This was done to retain a reasonable sample size in each stratum, so as to be able to fit a model. Critical predictors of VCT uptake among youths in the northern Nigeria are sex, education, religion, occupation and self-perception of risk for HIV while predictors in the southern Nigeria are age group and education (Table 4). Age, region, occupation, wealth index and age at sexual debut were selected as predictors of VCT uptake in males though the last two were not significant at 95% confidence interval while region, education, residence, wealth index and risk perception were selected for the females and residence was not significant at 95% confidence interval. These were used in the multivariate logistic regression to predict and determine the strength of association between the variables and voluntary Counselling and testing for HIV. Table 3 below shows the unadjusted and adjusted odds ratio, 95% confidence intervals and associated pvalues of the critical factors influencing the uptake of VCT in the study population. From the tables, as age increases, respondents are more likely to access VCT (AOR = 2.9, CI = 1.73 – 4.8) and females in the study were less likely to go for VCT (AOR = 0.15, CI = 0.04 – 0.51) relative to their male counterparts. In the regions, uptake of VCT is less likely in all the regions compared to the North Central region. Adjusted odds ratios and confidence interval for the regions are: North East (0.58; 0.23 – 1.44), North West (0.09; 0.03 – 0.31), South East (0.26; 0.08 – 0.92), South South (0.08; 0.01 – 0.48) and South West (0.02; 0.002 – 0.22) which are not significant for North East and borderline significant for South East. Youths who are employed are more likely to go for voluntary testing for HIV than those not working. The higher the level of education, the more likely the uptake of VCT. Respondents with higher education were much more likely to access VCT (AOR = 21.0, CI = 7.50 – 61.50) compared to those with no education. The likelihood of uptake of VCT increases with increasing wealth index. Respondents in the middle (AOR = 1.28, CI = 0.55 – 2.98) and upper class (AOR = 2.43, CI = 1.19 – 4.95) of wealth index were more likely to access VCT relative to those in the lower class. For the respondents' self perception of HIV risk, those with low (AOR = 2.0, CI = 0.55 – 2.98) and high (AOR = 2.43, CI = 1.44 – 14.67) perception of risk are more likely to go for VCT than those with perception of no risk for HIV. Discussion The results show a low national and regional prevalence in uptake of voluntary Counselling and testing (VCT) for HIV in the sub-population used in the analysis. This is probably due to lack of spread of VCT dedicated centers in the country, low awareness of VCT services, perceived high cost of HIV tests and fear of the consequences of the result. The 2003 NDHS did not report regional variations in the uptake of VCT for HIV or HIV testing in Nigeria, and existing literature in the databases searched did not yield any results on these variations, therefore the basis for comparing this and previous studies in Nigeria is lacking. The 2003 NDHS reported that about 10% (14% of males and 6% of females) of youths aged 15 – 24 in Nigeria had ever been tested for HIV. The figure differs from the result of this study (2.6%) because it measured HIV testing in many circumstances – those who volunteered, those who were offered the test and they accepted and those who were required to do the test for any reason whatsoever. This differs from a survey in South Africa 25 reported that 20% of young people aged 15-24 had ever been tested for HIV with females being more likely to be tested than males (25% versus 15% respectively, P-value <0.01). In this study, more males (4.6%) than female (2%) youths in Nigeria had volunteered for HIV Counselling and testing unlike the South African survey that reported the reverse 25. This supports the hypothesis that males are more likely to volunteer for HIV Counselling and testing in Nigeria compared to females. This may be explained by the fact that men are more open about their sexual behavior and do not need permission from anybody to decide on testing while women will often need the consent of their parents and spouses or partners. Women may also decline information on their testing status for fear of stigma, discrimination and marriage insecurity. Respondents aged 20-24 were more likely to volunteer for HIV testing compared with those aged 15-19 (4.11% versus 1.19%, P-value <0.001). This result is consistent in both sexes and in the six regions. The logistic regression results further confirm that those in the higher age group are more likely to go for VCT. This is similar to reported results from studies in Nigeria and other sub-Saharan African countries. For instance, Adewole4 reported that males of higher age groups responded more to voluntary HIV testing and Pettifor25 showed 12% and 29% of those aged 15-19 and 20-24 respectively volunteering for HIV testing. This age disparity may be due to the likelihood that younger youths have had a shorter sexual experience and are less informed on sexual issues than older youths. In traditional African societies, sex is often learnt about from peers and in schools rather than from family members. In this study more urban dwellers (3.8%) than rural dwellers (1.65%) had voluntarily tested for HIV (Pvalue <0.001). This is similar that data reported from a Ugandan antenatal study21 where urban dwellers were 2.7 times more likely to volunteer for HIV status testing than their rural counterparts. It is known that more information and education campaigns on HIV occur in urban areas, and myths about HIV/AIDS are prevalent in rural areas. Also, the National Action Committee on AIDS (NACA) reports that most ARV centers and by implication, VCT centers in Nigeria are in the urban areas. Regarding education, 11% of youths educated above secondary school volunteered for HIV testing compared to 3% and 1% of those who had secondary and primary or no education respectively (Pvalue<0.001). Logistic regression results also confirmed those with higher education as being 4.4 times more likely to volunteer for HIV testing than those with primary school or no education. This could be because youths with higher education are more aware of HIV and the risks it portends, have better sexual negotiation skills and could be more health conscious. These respondents could more likely be professionals, in the upper wealth index and therefore can afford unsolicited HIV testing to be assured of their status. The study by Adeneye10 among pregnant women also showed that those with post secondary education were more willing to be tested for HIV (93%) than those with no education (77%) (P-value <0.05). These results suggest that more HIV prevention strategies should be directed on rural and less educated populations. This study also showed increasing likelihood to volunteer for HIV testing with increasing wealth status. Males more than females in the upper wealth class (3.98%) were more likely to have volunteered for HIV testing than those in the middle (1.58%) and lower (1.11%) classes in all the categories and regions (p-value<0.001). A similar trend was also reported in NDHS (2003) where respondents in the highest wealth quintile (26.3%) were more likely to have been tested for HIV than those in the middle (6.85%) and lowest quintiles (4.45%). This may result from those in the higher wealth class being able to afford an HIV test, access testing centers as most of these are in urban areas, utilize private HIV testing services and have more exposure to relevant information for decisionmaking. A higher percentage of Christians (3.62%) had voluntarily tested for HIV compared to Moslems (1.3%) (p-value <0.0001). The males in both religions showed more likelihood to volunteer for HIV testing than females (Christians – 5.82% versus 2.96%; Moslems – 3.13% versus 0.69%). Daniel and Oladapo (2006) reported Christianity as an independent predictor of acceptance of prenatal HIV testing in Nigeria compared to other religious groups. The most likely explanation is the higher tendency for attaining education and the greater distribution of educational institutions in the Christian dominated parts of the country8. It was also found that youths who had changed a sexual partner once within the 12 months preceding the survey (7.52%) were more likely to have gone for voluntary testing for HIV compared to those with no sexual partners (2.51%) and those with 3 or more sexual partners (2.15%) within the same period. This trend is not statistically significant among males: 4.84%, 4.56% and 0.00% (p=0.971), but was not significant among females (p=0.001) where those with 3 or more partners had higher uptake than those with no partners. It is surprising that those with no sexual partners were found to be slightly more likely to have accessed VCT than those with 3 or more partners though stratifying by sex revealed that this occurred among males and is the reverse in the females. Compared to women, men tend to be predisposed to having multiple sexual partners without perceiving themselves to be at risk of HIV infection. This tendency can be described as that of men to handle relationships better than women and so can manage multiple relationships better. The concern here is that these young men are exposing themselves to higher risks for HIV and will more likely ignorantly infect their numerous partners which will further worsen the HIV prevalence in Nigeria, especially within this age group studied. Regarding condom use, young people who used condom in their last sexual activity before the survey were more likely (3.72%) to have gone for voluntary HIV testing than those who did not use condom (1.57%) (P-value <0.001). This trend is consistent across most of the regions where males who used condom had higher uptake of VCT than female. Using condom may define youths who are more HIV-aware and are determined to protect themselves and thus seek to know their status routinely. It may also be due to lack of confidence on the protective efficacy of condom. Respondents who perceived themselves at high risk for HIV were more likely to go for VCT (3.99%) compared to those with no risk perception (2.88%) and those with low risk perception (2.78%) (P-value <0.001). The highest VCT uptake in females, however, was surprisingly found in those with no risk perception for HIV (2.51%) against 2.1% and 2.04% in the high and low risk perception group respectively. Daniel and Oladapo26 reported selfperception of no risk as an identified predictor of VCT uptake among pregnant women in Nigeria. This is not surprising because majority of pregnant women are married and/or in monogamous relationship and so tends to perceive themselves not to be at risk of HIV infection. Marital status and HIV knowledge score of respondents were found not to be significantly associated with uptake of VCT. This is contrary to the report by Daniel and Oladapo26 that being married is positively associated with volunteering for HIV testing. This report is however based on pregnant women presenting to the clinic for antenatal care and who understand the potential of HIV testing for reducing mother-to-child transmission, and believe that being married confers some level of protection. Only a percentage of respondents with good HIV knowledge (3.09%) had volunteered for HIV testing while none of those with poor knowledge had volunteered. This study also confirmed that even with good HIV knowledge, which should have been a driving force towards people ascertaining their HIV status and receiving Counselling based on their status, VCT uptake is still low in Nigeria. This study found age, sex, region, education, occupation, wealth status and self-perception of risk for HIV to be the critical predictors of uptake of voluntary Counselling and testing (VCT) among youths in Nigeria (Table 4). There are slight differences in the predictors of VCT when stratified by sex. Factors significantly predicting uptake of VCT in males in the multivariate analysis are age, region and occupation while that of females are region, education, wealth status and risk perception. Adewole and Lawoyin5 identified age (for males) while Iliyasu15 and Daniel and Oladapo26 identified education and risk perception respectively for females as factors influencing VCT uptake in Nigeria. None of the identified studies assessed uptake of voluntary HIV testing in both gender so that existing data about VCT in Nigeria is segregated by sex. Comparisons with this study, which assessed VCT in Nigeria in both gender, should therefore be carefully interpreted and applied in terms of programs implementations. The Nigerian studies reported on other variables affecting VCT uptake but which are not discussed because they were not found in the dataset used. Some of those variables are stigma, experience of Counselling, influence of partners, fear of discrimination and marriage security. This is of one of the limitations of this study. This study also lacked qualitative data to further probe specific responses of interest to the study and provide contextual insights into the findings. Conclusion The study supports the hypothesis that voluntary HIV testing is associated with region of residence and that socio-economic status, measured by wealth status and gender differences affects uptake of voluntary HIV testing. These findings provide evidence and a basis for designing appropriate national programs in urban and rural areas designed to meet the needs of male and female youths. Also, youths will benefit from mass HIV prevention campaigns to bridge information gap, proper training of health workers to become youth friendly and subsidized or free VCT services to improve access and utilization. Recommendations For policy and planning, the Presidential Council on AIDS (PCA) in Nigeria needs to enact policies that prioritize the response to HIV/AIDS control to that of prevention rather than the current emphasis on antiretroviral therapy. This will be achieved by empowering state and local governments to conduct large-scale prevention programs and incorporate HIV prevention strategies into the educational curriculum, especially at the primary and secondary school levels. The current policy on Universal Basic Education for free education up to junior secondary is limiting. Free and compulsory education until completion of senior secondary school will accelerate the rate of acquiring HIV related information, reduce unemployment and increase the wealth status of the youths; all of these contribute to better HIV prevention outcomes. Designated VCT centers should be established in all government health facilities and by nongovernmental organizations and trained staff deployed to manage them in order to provide more accessible, affordable and effective VCT services. This is irrespective of whether the centers are offering anti-retroviral treatment (ART) or no. Voluntary Counselling and testing for HIV taking place in centers not offering ART will reduce stigma, offer more privacy and can serve as units of first contact in HIV prevention for young people. VCT providers should also be trained in Counselling and skills in working with youths who may have peculiar problems, different from that of adults. Most HIV testing in Nigeria is presently not accompanied by detailed Counselling because of lack of trained staff to do so. There is also a need to consider establishing and increasing the number of youth-friendly VCT services to provide privacy, confidentially and protect young people seeking VCT form stigma and discrimination. Apart from including VCT awareness in school curricula, outreach activities to schools and youth organizations should be carried out routinely as a way of expanding programs on information, education and communication (IEC) on risk behaviors, safe sex practices and the importance of knowing ones HIV status. In terms of research, this study revealed an important gap in research regarding uptake of VCT in Nigeria. It showed a very low uptake of VCT (2.6%) among young people in Nigeria, consistent in all the regions of the federation. There is need for a nationally representative primary study to determine regional correlates of VCT uptake in Nigeria, exploring all possible variables for young males and females. This should combine both qualitative and quantitative study designs to explore reasons and opinions on why young people are shying away from being voluntarily tested for HIV. The Ugandan HIV/AIDS control experience showed that even though about 70% of the youths were willing to be voluntarily tested for HIV, only 12% had been so tested 27. The result of such study can be used in the planning and implementation of programs to scale up VCT services and uptake, especially as the social context varies in the various geo-political zones. Further research should be carried out to find out why those who had multiple sexual partners were the least likely to have volunteered for VCT. Such study should explore such variables as age, sex, stigma, sex work and polygamy. The regional differences in VCT uptake should also be explored, looking at the variations in the southern and northern regions. The study can independently assess whether the predictors of VCT uptake observed at the national level and in the different sex groups hold true for the various regions. This will shed more light on the different social, cultural and religious factors that could influence VCT uptake and their impact on the lifestyles of the people. Research will also be beneficial into the numbers of testing services for HIV that were accompanied by post and pre-test Counselling and the quality of the Counselling given. This will help in formulating policies and programs for effective VCT rollout, to effectively prevent the spread of HIV and improve access to treatment for infected individuals in Nigeria. ACKNOWLEDGEMENT This study was supported by ORC Macro and Measures DHS+, Calverton (Maryland), USA who generously granted permission for the use of the data. We acknowledge the support of the staff and students (2006 Class) of Epidemiology and Biostatistics Master's programme of the School of Public Health, University of Witwatersrand, Johannesburg, South Africa. Edmore Marinda, Ronnel Kellerman, Mary Kawonga Lindy Mataboge, Lawrence Mpinga, Hisham Elmadi and Rugola Mtandu are appreciated for their invaluable advice during the analysis process. REFERENCES
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11026t2.jpg] [rh11026t3.jpg] [rh11026t4.jpg] [rh11026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}