 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
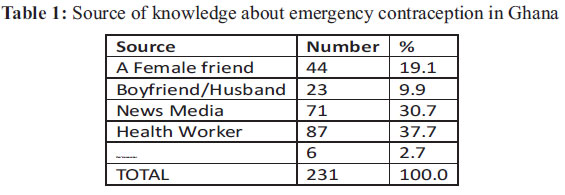
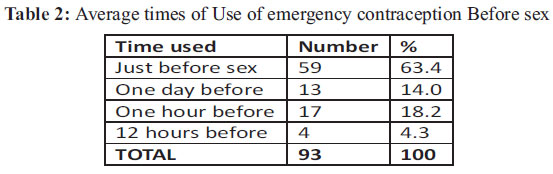
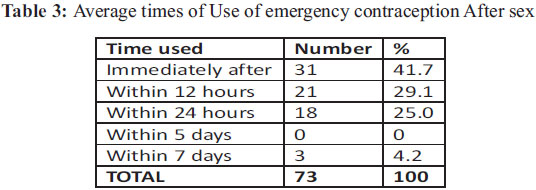
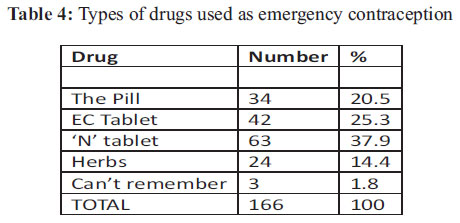
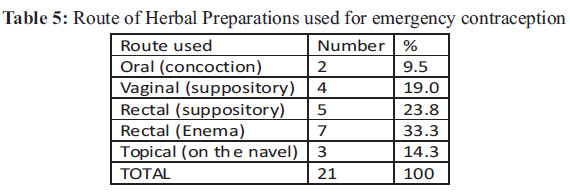
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 147-152 ORIGINAL RESEARCH ARTICLES Knowledge and Practices of Emergency Contraception among Ghanaian Women Baafuor Opoku1 , Fauster Kwaununu2 School of Medical Sciences, Kwame Nkrumah University of Science & Technology, Kumasi1 Komfo Anokye Teaching Hospital, Kumasi2 E-mail: baafuoropoku@yahoo.com Code Number: rh11027 Abstract The use of emergency contraceptives (EC) to prevent unwanted pregnancies when effective contraception has not been used is universally acknowledged. A study looked at the knowledge and practices of emergency contraception in 476 women in the reproductive age in Ghana. Knowledge and usage of EC applied to 57% and 41% of participants, respectively. Knowledge was independent of age (p=0.26), marital status (p=0.14) and level of education (p=0.21). Drugs (85.6%), herbal preparations (14.4%) and douching (43%) were used for emergency contraception. Drugs used included the combined Pill-24.0%, Postinor-28.5% and Norethisterone-43%. Only 44% correctly used drugs as EC. There is a high level of knowledge about EC as well as usage in the country. There is general misuse of norethisterone as EC. There is no knowledge in this study population that intrauterine device can be used as EC. Résumé On reconnait universellement l'emploi des contraceptions d'urgence (CU) pour pr évenir les grossesses non voulues quand la contraception efficace n'a pas été employée. L'étude a examiné la connaissance et les pratiques de la contraception d'urgence chez 476 femmes en âge gestationnel au Ghana. La connaissance et l'usage des CUs s'appliquaient à 57% et 41% des participantes respectivement. La connaissance n'avait rien à voir avec l'age (p=0,26), l'état civil (p=0,14) et le niveau d'instruction (p=0,21). Les méicaments (85,6%), les remèdes à base de plantes et la douche vaginale (43%) ont servi de contraception d'urgence. Parmi les médicaments employés étaient la pilule combinée -24%, Postinor 28,5% et Norethistérone -43%. Il n'y avait que 43% qui ont utilisé les médicaments comme CU. Il y a un haut niveau de connaissance à l'égard de CU aussi bien qu'à l'égard de l'usage dans le pays. Il y a partout un abus de Norethistérone comme CU. Dans cette population, il n'y a pas de connaissance que l'on peu utiliser le dispositif intra-utérin comme CU. Key words: emergency contraception, knowledge, practices, Ghana Introduction The contribution of contraception to reductions in maternal mortality and morbidity is universally acknowledged 1,2. Prevention of unwanted, as well as mistimed and unplanned pregnancies is afforded by the use of effective means of contraception. It is estimated that about 20% of all births are unwanted at the time of conception in Asia and Latin America 3. In Ghana 16% of births are unwanted, 40% are unplanned and 24% mistimed 4. Assuming that unwanted births carry the same risk to the health of the mother as wanted births, it is estimated that the global burden of disease attributable to unwanted births amounts to 4.6 million disability-adjusted life years [DALYs]5. Knowledge of any contraceptive method is almost universal in Ghana, with 98 percent of all women and 99 percent of all men knowing at least one method of contraception 4. However, while 47.4% of Ghanaian women have a history of contraceptive use only 20% are current users. Where women are not using contraception, contraception has failed (such as condom breakage and spillage) or not been used properly, the last resort to preventing an unwanted pregnancy is the use of emergency contraception (EC). Emergency contraception refers to any drug or device which when used after unprotected sexual intercourse, will prevent pregnancy 6. It is also known as 'postcoital contraception' and used to be called 'the morning-after contraception'. Emergency contraception works primarily by preventing or delaying the release of ova from the ovaries7. Documented use of EC in humans dates back to the 1960s when a young girl was given estrogen extract to prevent pregnancy after she was raped8. Two methods of conventional EC are used: hormonal drugs and the intra-uterine contraceptive device (IUD). Several drug regimens in various combinations have been described using either estrogen or progestogen, or both. The Yuzpe regimen 9 was described in 1974 and uses 100µg of ethinylestradiol plus either 1.0mg norgestrel or 0.5mg levonorgestrel, taken within 72 hours of the coital act and repeated at 12 hours. Containing a relatively high dose of estrogen, it is associated with nausea and vomiting. Its efficacy is around 75%10. Progestogen-only preparations are also used as EC. They employ two doses of 750µg of levonorgestrel taken 12 hours apart. They are more effective (85%) than the Yuzpe regimen and produce less side effects 6. A single dose of 1.5mg levonorgestrel also appears to be as effective as the two-dose regimen11 . The antiprogesterone, Mifepristone, also called RU 486, is the most promising hormonal EC. A single dose of either 10mg or 25mg given within up to 5 days of unprotected sex has been shown to be equally effective as levonorgestrel 11 . The Cu-T IUD is the most effective method of EC offering almost 100% protection12. It also has the added advantage of being still effective if inserted up to 5 days of unprotected sex. The Ministry of Health of Ghana introduced emergency contraception into its Reproductive Health Policy and Standards in 1996 13. Two tablets of Ovral, a combined oral contraceptive pill, each containing 50µg of estrogen and 250µg of levonorgestrel was adapted and used as the Yuzpe regimen. Since then several social marketing groups have helped promote the use of EC in the country. The Planned Parenthood Association of Ghana introduced 'Postinor-2', a dedicated progestin-only EC product onto the Ghanaian market a couple of years ago. Few studies have since been done on the knowledge, attitudes and use of EC in Ghana. Two of such studies were with university students14,15. A couple others have been done with health care providers and spermicidal users16,17 . The current study looked at the knowledge and practices of EC among women of reproductive age in the country. Material and Methods The study was conducted among women in the reproductive years randomly selected from two urban and three rural districts in three regions of Ghana. Selection was achieved by using Research Randomizer generated by Social Psychology Network (www.randomixer.org). In all, 467 women were recruited and enrolled. A questionnaire, that had been pretested, was either given to the participant or directly administered by trained interviewers depending on the respondent's ability to read and write and her wishes. One hundred and sixty-nine questionnaires were given out while 298 were directly administered. Where the respondent wished to self-administer the questionnaire, the meaning of “emergency contraception” was explained to mean any measures taken to prevent unwanted pregnancies following unprotected intercourse, before it was given out. Questionnaires given out were collected after 72 hours. Answers sought included basic demographic data, previous and current contraceptive practices, as well as social and sexual history. Women who were using a form of regular contraception were excluded from the study. The study was undertaken over a six-week period in February-March 2009. Data was transferred onto and analysed by Epi Info Ver 3.5.3. Ethical approval for the study was given by the Committee on Human Research, Publications and Ethics of the School of Medical Sciences, Kwame Nkrumah University of Science and Technology and Komfo Anokye Teaching Hospital, Kumasi. Results Results presented are for 402 participants as 65 of them either had a lot of item non-response or could not be traced to retrieve questionnaires given out. The mean age was 24.5 years (SD--7.2) and the mode 20.0 years. Sixty-four percent of respondents were nulliparous while 2.7% had at least five children. The mean parity was 0.7. Fifty-six percent had education up to the secondary level, 25.9% to the tertiary level and 5.5% had no education. Sixty-two percent were students, 28.9% were in employment, 3.5% were apprentices while 5.6% were unemployed. Sixty-seven percent were single, 20.4% were married and 10.0% were either cohabiting or divorced. Almost 89% had knowledge about contraceptives. Ever-use of any type of contraception was 49.0%. About 57% had knowledge about emergency contraception which at 95% confidence intervals was found to be independent of age (p=0.26), marital status (p=0.14) and level of education (p=0.21). Of these, 71% had used it before. This formed 41% of all participants. Methods used as emergency contraception were drugs (85.6%), herbal preparations (14.4%) and douching (43%). Douching was used either alone or in combination with the other two methods for contraception and also to 'feel clean'. Of those who used drugs, 56% used it before sex while 44% used it after sex. With regard to frequency of use, 21% had used it just once, 61.0% had used it between two and five times while 18% had used it six or more times. Table 1 shows their source of knowledge of EC. Tables 2 and 3 show times when drugs were used in relation to coital activity. Table 4 shows type of drugs and Table 5 routes of administration of herbal preparations used for emergency contraception, respectively. While a pharmacy/chemical shop was the major source of drugs for EC (63%), other sources included boyfriend/husband (17%), health facilities (12.7%) and friends (6.7%). Herbal preparations were bought in the market place (71%), obtained from friends (12.6%) or self-made (16.4%) by the women. Fifty-four percent of participants said they would maintain an unintended pregnancy, 26.9% would abort it, whilst 18.9% were undecided. With regards to using regular contraceptives, 52.9% said they would use it whilst 47.1% would not. Reasons for not using regular contraceptives were mainly myths surrounding fertility after usage. Discussion Awareness of contraceptives though high in this study population, is relatively lower than is quoted by the Demographic and Health Survey Report 4. Previous use of a contraceptive (49.0%) mirrored that found by the Survey Report (50.4%). Knowledge of emergency contraception was comparable to a study on university students, contrary to suggestions that it could be lower in less literate populations 14,15. Knowledge was also found to be independent of age and marital status. The finding that health workers were the main source of knowledge on EC is re-assuring as the mysteries and myths surrounding the use of contraception are expected to be addressed. The study by Baiden et al 14 found the major source of information on EC to be the media, whilst in South Africa 'friends' were the major source18 . Previous use of EC (41%) was higher in this population than the 4.2% found among university students in Ghana15 and 16% and 9.1% found in Kenya19 and South Africa18, respectively. The finding that 56% of previous users of EC used it before sex is worrisome and shows that though health workers were their major source of information about EC, understanding of how it works is still a problem. Forty-four percent correctly used EC after sex. This figure is relatively higher than that found by Baiden et al (11.3%) with university students14 . Of those who correctly used EC after sex, 95.8% did so within 24 hours. This is very encouraging as the sooner after unprotected sex EC is used, the more effective it is in preventing pregnancy7, 20. On the other hand the fact that none of the participants used EC between 24 hours and five days following unprotected sex is disturbing as the too narrow period of 24 hours used might prevent clients from using EC beyond 24 hours. Emergency contraceptive Pills have been proved to be effective even up to five days7, 20 . Almost 24.0% of participants had used the combined Pill as EC. This compares favorably with 26.3% found by Baiden et al 14. The dedicated EC tablet, Postinor-2 was used by 28.5% of participants. In 2002, only 1.5% of participants knew of this in Ghana14. If this is a real trend, then social marketing groups must be congratulated for having promoted its use over the past few years. Norethisterone is a progestagen used to induce withdrawal bleeding in secondary amenorrhea and also to manage abnormal uterine bleeding. It is also found in combination with estrogens as a combined Pill (eg Loestrin). Forty-three percent had used it in various dosages for EC probably because of its ability to induce withdrawal bleeding in anovulatory cycles. Whether it works as emergency contraceptive was not addressed in this study. None of the participants had heard of or used the intrauterine device as EC. In a study on health care providers, 28% knew of the IUD as EC17. In another study15 , 12.8% of university students in Ghana knew of the IUD as a form of EC. These findings are not encouraging and more education needs to be done. Herbal preparations were used by 14% of women as emergency contraception. The 'Neem' tree was mainly mentioned, used variously as enema or rectal and vaginal suppositories. Contraceptive properties of the neem tree have been evaluated by several studies 21,22,23 . Some women believe that using a vaginal douche immediately after sex will help prevent a pregnancy. In reality, douching may push sperm further into the uterus, thereby encouraging a pregnancy24. Vaginal douches as found in 43% of women in this study, should never be used as a method of birth control. Regularly using a douche on the other hand, has been associated with increased risk of pelvic inflammatory disease as well as ectopic pregnancy24. Moreover, since the vagina naturally cleanses itself, there is no need to douche for personal hygiene, as some of the reasons ascribed by women in the study. Conclusions There is a relatively high level of knowledge about EC as well as usage in the country. Knowledge on EC is not dependent on age, educational level or marital status. There is general misuse of norethisterone and dependence on douching as EC. There is no knowledge that intrauterine device can be used as EC. More education is needed on the correct timing of use of EC. With their ever-growing presence, the media should be encouraged to help disseminate information about EC to communities. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11027t2.jpg] [rh11027t4.jpg] [rh11027t1.jpg] [rh11027t3.jpg] [rh11027t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}