 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
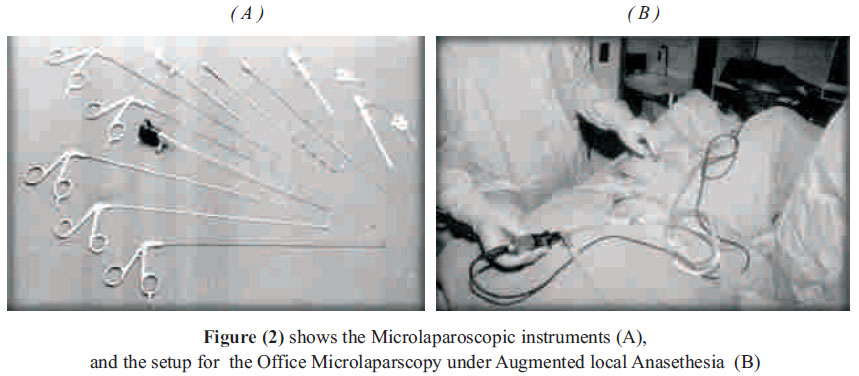
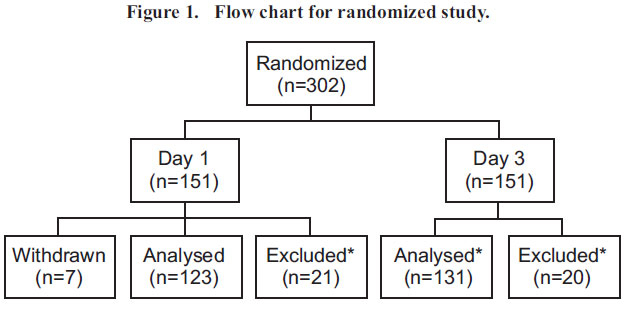
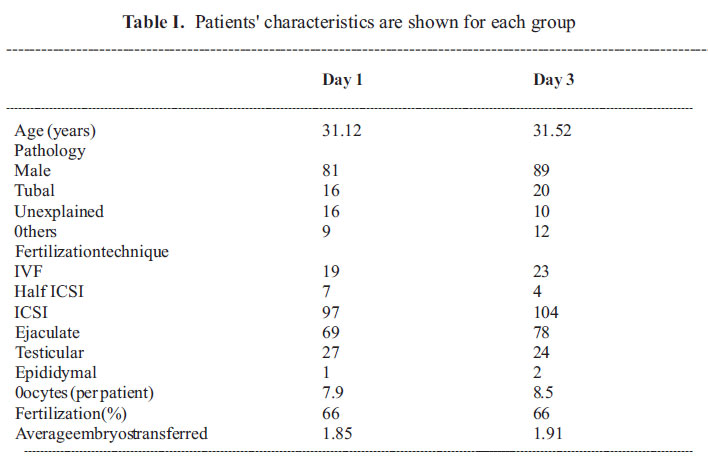
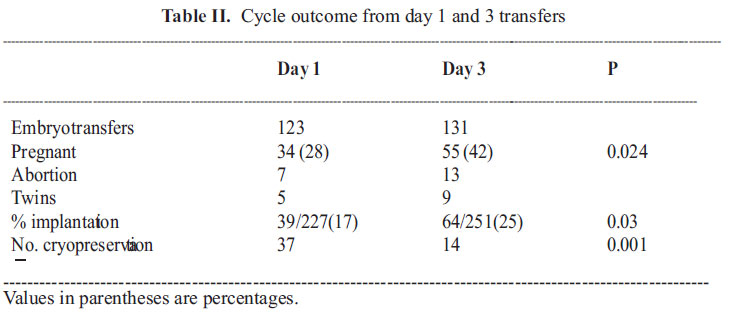
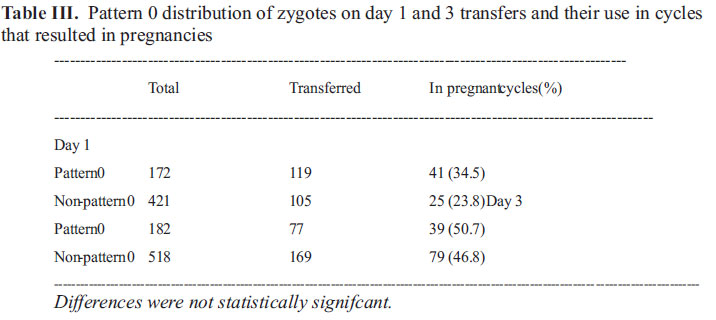
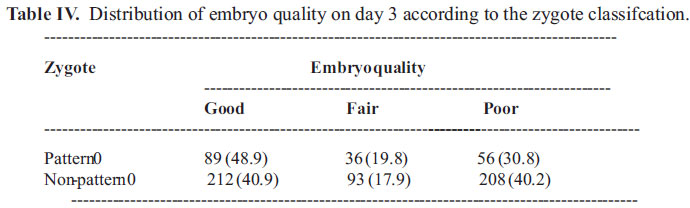
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 153-162 ORIGINAL RESEARCH ARTICLES Office Microlaparoscopic intrafallopian transfer of day one Zygote Versus day three embryo transfer after previous failed ICSI trials Emad M. Siam.PhD.MRCOG.MD. Corresponding author: Department of Obstetrics and Gynecology, College of Medicine, El-Minya University, Egypt. Tel.: +20862346586 Fax: +20862334456 Cellular: +20103480999 E-mail: eemsalah@yahoo.com The research work was carried out at the El-Minya University Hospital,a tertiary referral center in upper Egypt. Code Number: rh11028 Abstract The objective of the study was to investigate whether transferring zygotes on day 1 would result in similar pregnancy rates compared to transferring cleavage stage embryos on day 3 in a prospective randomized trial, using the office microlaparoscopic procedure. Patients undergoing IVF/ICSI treatments were randomized to either day 1 or day 3 transfers after previous failed ICSI trials due to failed implantation. The primary outcome measure was pregnancy rate. Pregnancy rates were higher in day 3 group (55/131, 42%) when compared to day 1 (34/123, 28%, P = 0.024). Similarly, implantation rates were higher in day 3 group (P= 0.03). There were more cycles with cryopreservation in the day 1 group (P < 0.001). Embryo quality on day 3 was similar between pattern 0 and nonpattern 0 zygotes. Day 3 embryo transfers result in better pregnancy and implantation rates compared to day 1 zygote transfers. Résumé Cette étude avait pour objectif d'examiner si le transfert des zygotes dès le premier jour aboutira aux taux de grossesse similaire par rapport au transfert des embryons du moment de segmentation le troisième jour dans un essai prospectif et randomisé à l'aide de la procédure micro-laparoscopique de bureau. Les patientes qui subissent des traitements de FIV/ISIC ont été randomisées en transferts du premier jour ou du troisième jour. Le taux de grossesse était plus élevé chez le groupe du troisième jour (55/131, 42%) par rapport au groupe du premier jour (34/123, 28%, P= 0,024). De la même manière, le taux d'implantation était plus élevé chez le groupe du troisième jour (P=0,03). Il y avait plus de cycles qui avaient la cryopréservation chez le groupe du premier jour (P<0,001). La qualité de l'embryon le troisième jour était pareille parmi les zygotes du modèle 0 et les zygotes 0 sans modèle. Les transferts des embryons du troisième jour aboutissent à de meilleurs taux de grossesse et d'implantation par rapport à des transferts des zygotes du premier jour. Key words: embryo transfer, pronuclear scoring, zygote Introduction The in vitro growth of human embryos might be supported up to blastocyst stage prior to transfer into its natural environment, the uterine cavity. During this period three distinct phases are noted, the pronuclear stage on day 1, the early cleavage stage on days 2 and 3 and the blastocyst stage on days 5 and 6 after oocyte retrieval. During these complex developments, embryologists have only microscopic observations to assess the quality of embryos. After more than two decades practice of assisted reproduction, the best day to transfer embryos to the uterus is still subject to debate. Although the general practice is to transfer at the cleavage stage on day 2 and 3, the concept of transferring embryos at blastocyst stage has gained popularity with the emergence of advanced sequential media 1. This strategy has been challenged by several prospective randomized trials2,3, and the top quality embryos can be selected with better implantation potential on day 3 4,5. It seems that the challenge lies in the selection of viable embryos regardless of the day of the transfer. The transfer at pronuclear stage could be justified since the basis for selection according to distinct morphological features of pronuclei has been proposed 6. It was demonstrated that embryos transferred at the zygote stage have the ability to implant and end in viable pregnancies 7,8. Improvement of the technology of the laparoscopic sets has helped to re-visit an outdated ART procedure, which is the intrafallopian transfer procedure of gametes or early developing zygotes, which have been replaced with the simpler intrauterine transfer procedure. Using the newly advanced fiber optic 2 mm microlaparoscopic sets has resuscitated those intrafallopian procedures, with a very short time procedure, without the need of anesthesia, and with a laparoscopic image developed almost similar to the one produced from the traditional 10 mm laparoscopic sets, and may be better10-14. It has also been shown that the morphology of pronuclear embryos is correlated to day 3 or 5 embryo morphology and/or pregnancy/implantation11-14 . The nuclear events are dynamic and happen during a certain time course15 . Although Scott and Smith performed pronuclear scoring at three different times (16 and 17, 22 and 22 and 26 h post insemination), Tesarik and Greco have suggested a successful use of a single static observation (12 -20 h post insemination or ICSI) of pronuclear morphology as a predictor of possible abnormal preimplantation development6-9. The objective of the present study was to asess the use of a new advanced microlaparoscopic set, with the fiber optic technology, in an office procedure without general anesthesia, as the first arm of the study, and to investigate the transfer of zygotes selected according to a single observation of pronuclear morphology, could result in similar pregnancy and implantation rates compared to those obtained by transferring embryos on day 3, as the second arm of the study. Materials and methods This study is a prospective randomized trial of day 1 versus day 3 embryo transfers, using a newly advanced fiber optic microlaparoscopic set in an office procedure. The day of oocyte retrieval was considered as day 0. The study was approved by El-Minya university Ethical Committee in July 2008. All couples undergoing oocyte retrieval between December 2008 and 0ctober 2009 were informed about the study and asked to sign consent if they wish to participate in the study on the first day of gonadotrophin injections. All couples included had previous failed ICSI and uterine emrbyo transfer due to failed implantation. Patients who consented were randomized to either 'day 1' or 'day 3' transfer by envelope withdrawal technique by the laboratory personnel 1 day before the oocyte retrieval. To guarantee uniform distribution over the time-period, a block of 14 envelopes (seven for each group) was placed in a box for withdrawal. Patients with no embryo transfer were excluded later from the study. IVF/ICSI Controlled ovarian hyperstimulation, oocyte retrieval, sperm preparation for IVF/ICSI and embryo culture and evaluation were performed as described previously16-18. Culture conditions were the same for both groups. Cumulus± oocyte complexes after retrieval from the follicular fluid were transferred into 100 ml IVF medium (Medi-Cult, Denmark) under mineral oil (Sigma, USA). They were incubated in 5% C02 in air with saturated humidity. All the fertilized oocytes were cultured individually in 20 ml Medi-Cult IVF medium under mineral oil until the time of the transfer. Embryos were graded as good, fair and poor. Good embryos were defined as embryos with <10% fragmentation and >4 blastomeres. Fair embryos had 10 -20% fragmentation and poor embryos were heavily fragmented (>30%). Pronuclear scoring Normal fertilization was confirmed by the presence of two pronuclei and two polar bodies 15 to 18 h following insemination or ICSI. Zygotes were evaluated according to criteria of Tesarik and Greco (1999). Each zygote was checked for the presence of a cytoplasmic halo, alignment and size of pronuclei, nucleolar precursor body (NPB) number and distribution pattern under an inverted microscope with a Hoffman modulation contrast system. All the information was recorded on a predesigned data sheet and then registered into a database (Microsoft Access). Zygotes were classified according to pattern 0 or non-pattern 0 (Tesarik et al., 2000). Briefly, pattern 0 zygotes had the following features: (i) the number of NPB between both pronuclei did not differ >3, (ii) NPB in both pronuclei were either polarized or scattered, (iii) in the polarized pronuclei, the number of NPB were <7, (iv) in the scattered pronuclei, the number of NPB was >7, (v) both pronuclei were similar size and Analysed* (n=131) Excluded* (n=20) aligned. Embryo transfer The microlaparoscopic system consists of a light source, a high speed pneumoperitoneum device, and a 1CCD video camera. The diameter of the fiber optic scope was 2.2 mm, and the grasping forceps, scissors, needle probes, biopsy forceps and irrigatoraspirator were also 2.2 mm in diameter (all equipment made by Olympus, Tokyo, Japan). In our unit, a maximum of two embryos is routinely transferred. For day 1 transfers, two pattern 0 zygotes, when available, were chosen to transfer on the same day. Maximum two pronuclear-stage zygotes were loaded into the catheter (delivery catheter, 35 cm; Cook). The instruments could be used by specially designed trocar (access needle; Ethicon, Cincinnati, OH, USA), 12-cm long and 2.5 mm in diameter metal sleeve that ?ts over the veress needle, all introduced after local infiltration anesthesia. If there is only one or no pattern 0 zygote available, non-pattern 0 zygotes were used. When there were at least four extra zygotes, they were cryopreserved. For day 3 transfers, embryos were cultured until day 3 on which the best two embryos were chosen for transfer according to day 3 embryo quality17. Cryopreservation was performed only when a patient had at least four good quality embryos with <10% fragmentation without any developmental block from day 2 to 3. The patient was placed in a lithotomy position. An Access Needle (Eticon, Tokyo, Japan) was inserted through a small incision created in the subumbilical region using the closed method, after been locally infiltrated with Xylocaine local anaethesia. Pneumoperitoneum was induced with carbon dioxide gas. Other Access Needles were then inserted into both sides of the hypogastric region under microlaparoscopy. Four ml/port of 0.25% bupibacaine was locally injected at the trocar insertion sites in advance. All the scopes and forceps used were from the microlaparoscopy set of 2.2mm in outer diameter (Olympus, Tokyo, Japan). Pre-medication consisting of 0.5 mg of atropine sulfate and 1 mg/kg of midazolam was given intramuscularly. One mg/kg of fentanyl followed by 1.5 mg/kg of ketamine was intravenously administered through a drip infusion line, according to the level of patient pain perception, and under meticulous follow up of the patient vital signs , especially the blood pressure and the central oxygen concentration. Patients in both groups were supplemented with progesterone (Prontogest 400 mg / day, IBSA Egypt) starting from day 3 following the oocyte retrieval. Pregnancies were diagnosed with Tandom Icon urine hCG test (Hybritech, USA), and upon positive urine tests, serum B-hCG levels were quantifed. The status of pregnancy was checked by ultrasound examinations 5 weeks after embryo transfer. Statistical analysis A total of 302 patients was recruited into the study. This number was calculated on the assumption that a 15% lower pregnancy rate compared with the established rate (35%) would be considered as failure for the zygote transfer group. The sample size for the 0.15 difference in proportion with a power of 80% and α of 0.05 requires ~151 patients in each group. Comparisons between groups were made by using γ2 -analysis. P < 0.05 was considered statistically signifcant. Results A total of 302 patients was included in the study. Seven patients, all in the day 1 group, withdrawn from the study. A total of 41 were excluded from the two groups due to suboptimal stimulation, hyperstimulation, no oocytes or sperm available, no fertilization of the oocytes or no division of the embryo. There were 123 and 131 embryo transfers in day 1 and 3 groups respectively (Figure 1). Patients' and cycle characteristics were similar between the two groups (Table I). Pregnancy and implantation rates were higher in the day 3 group (55/131, 42%: 64/251, 25%: P < 0.05: Table II) when compared to day 1 (34/123, 28%: 39/227, 17%: P < 0.05) respectively. The abortion and twinning rates were similar between both groups. There were more cycles with cryopreservation in the day 1 group (P < 0.001). There were 172/593 and 182/700 pattern 0 zygotes in the day 1 and 3 groups respectively.A total of 119 pattern 0 and 105 non-pattern 0 zygotes on day 1 were transferred. Among those, 41 (34.5%) pattern 0 and 25 (23.8) non-pattern 0 zygotes were in pregnant cycles (P = 0.11). 0n day 3, 77 and 169 embryos generated from pattern 0 and non-pattern 0 zygotes were transferred respectively. There were 39 (50.7%) pattern 0 and Differences were not statistically signifcant. There was no statistically signifcant difference in the distribution of patients. 79 (46.8%) non-pattern 0 zygotes in pregnant cycles (P = 0.66, Table III). Embryo quality on day 3 was compared to pronuclear morphology on day 1. There were 89 (48.9%) and 212 (40.9%) good quality embryos generated from pattern 0 and non-pattern 0 zygotes (P = 0.075, Table IV). Discussion The intrafallopian environment is the best place, housing both the sperms, the oocytes and the developing embryos, as nature is nature. This fact had been confirmed with several researches, analyzing this intrafallopian environment, so transfer of gametes and early developing zygotes would assimilate the nature, and would definitely have the best outcome. The obstacle against the intrafallopian transfer, was the necessity to intervene into the tube, either with a laparoscope or hysteroscope. The newly advanced technology has facilitated the use of laparoscope with the minimal intervention. There is no consensus as to what constitutes the optimal stage for embryos to be transferred to the uterus. Zygote transfers were performed in the early days of assisted reproduction18. Pyne et al. reported that pregnancy rate after zygote transfers was similar to day 2 embryo transfer during optimal laboratory conditions but superior under suboptimal conditions. The pronuclear embryo transfer resulted in ~40% pregnancy rate after selecting zygotes according to pronuclear morphology1-5. However, Chen et al, reported disappointing results for zygote transfer in a prospective randomized study, which was halted at an interim analysis3,5,18-20 . Similarly, Margreiter et al. showed that the lowest pregnancy rates were obtained with day 1 transfers. A recent prospective randomized study demonstrated the feasibility of zygote transfers in an unselected population undergoing assisted reproduction4-6. In the present study, zygote transfers resulted in significantly lower pregnancy rates compared to day 3 cleavage stage embryo transfers. Earlier studies did not mention any selection criteria for zygotes to be transferred while Hurst et al. gave a brief description of zygote selection. Day 1 transfers resulted in the lowest pregnancy rates when compared to day 2±3 or 4±5 transfers in a prospective randomized multicentre study22-25 . However, no detail was given as to how zygotes were selected for transfer. Scott and Smith described detailed criteria for zygote scoring in which the early cleavage was also assessed. Tesarik and Greco later described a single static observation of pronuclear stage morphology of implanted embryos, which was later used to select zygotes to transfer by Dale et al. and also by us in the current study19-22. The main difference between these two studies was the average number of zygotes and embryos that were transferred: 1.85 versus 3.2 on day 1 and 1.91 versus 3.6 on day 3 in our study and that by Dale et al. respectively. By transferring more zygotes, Dale et al. might have obtained similar pregnancy rates for day 1 and day 3 transfers. Although they have transferred more embryos, pregnancy rates were similar between the two studies for embryo transfer20-23. It has been earlier reported that decreasing the number of embryos did not change the pregnancy rate on day 3. This might indicate that zygote selection alone might not be suffcient to choose the most viable embryos26. In our study, zygotes were selected for transfer according to the pattern 0. Results were also separately analysed according to revised Z-scoring of Scott et al3,6,23. None of the scoring systems showed any correlation between the use of higher quality zygotes in transfers and pregnancy rates21,23. Although there are several reports relating pregnancies to pronuclear scoring also did not find any difference in pregnancy and implantation rates between the pattern 0 and non-pattern 0 groups in single embryo transfer patients20-23. We analysed the relationship between embryo quality on day 3 and pronuclear morphology of those embryos, and did not find any significant correlation. Similar to our data, Salumets et al. did not find any significant difference of embryo morphology and zygote scoring15-19. The suggested office microlaproscopic procedure has been accepted by almost all cases included, as it was a short time (7-15 minutes) procedure, with the least felt pain during the procedure, especially most cases had preferred to be awake during the procedure, to follow the transfer procedure step by step. The images produced from the fiber optic microlaparoscopic system was nearly similar to the images produce from the traditional 10 mm system, so all the operating team was happy with this simple interesting procedure. No intra or post-operative complications had developed during the procedure, and all candidates were happy with the procedure, and express their full agreement to repeat the procedure in the future10-15. The observation time might have played an important role on the grading of zygotes. The coalescence and polarization of NPB are dynamic events5,9,10. Timing of pronuclear formation is markedly varied between oocytes after ICSI2,3. This individual difference might be further substantiated in IVF since penetration of sperm through cumulus cells, zona pellucida and fusion might require at least an extra 4 h following insemination18-20 . It has been reported that four stages have been distinguished during pronuclear development and some of the zygotes never reach the fnal stage4,5. A single observation, as has been common practice, including this study, might not reveal the true status of zygote morphology because it cannot determine whether the nuclear development is in progress or arrested at any one of the four stages24-27. There were significantly more cycles with cryopreservation in the day 1 group. Our criterion is to freeze when there are at least four zygotes or embryos available. Embryos were only frozen if they were classified as good quality while zygotes were frozen regardless of their pronuclear morphology which resulted in more cryopreservation in the day 1 group. This is in contradiction to others who have reported a positive correlation with zygote morphology and cleavage stage embryo quality. The literature still remains inconclusive on this issue28-30. It has been proved that the office microlaparoscopic procedure under augmented local anesthesia, used for embryo transfer was a good reliable choice for embryo transfer, regarding easy, safe, reasonable time and the patients satisfaction with the procedure. It has also proved, that day 3 embryo transfers result in better pregnancy and implantation rates compared to day 1 zygote transfers. Pattern 0 zygotes had similar day 3 embryo quality and pregnancy outcome as compared to zygotes with non-pattern 0 morphology. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11028t4.jpg] [rh11028t3.jpg] [rh11028f1.jpg] [rh11028t1.jpg] [rh11028f2.jpg] [rh11028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}