 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
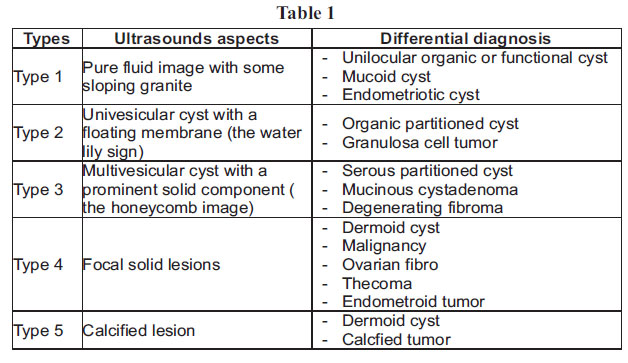
African Journal of Reproductive Health, Vol. 15, No. 2, June, 2011, pp. 165-168 CASE REPORT Primary Pelvic Hydatid Cyst An unusual cause of cystic adnexal image (mass) Yassir Ait Benkaddour Department of Obstetrics and Gynecology “A” Cadi Ayyad University, Marra Kesh, Morrocco E-mail: yaitbenkaddour@gmail.com Code Number: rh11030 Abstract Hydatid cyst is a parasitic human infection which is endemic in North Africa. It is more frequently localized in the liver and the lung. Involvement of others sites is usually secondary to these primary localizations. We report 2 exceptional cases of primary pelvic hydatid cyst diagnosed respectively in a 37-year-old and in a 48-year-old women. These cases will focus on the different characteristics of the infection, and the benefit of including epidemiologic arguments in using the diagnostical approach of adnexal masses. Résumé Le kyste hydatique est une infection humaine qui est endémique en Afrique du nord. I l est surtout localisé dans le foie et le poumon ; l'implication des autres foyers est souvent secondaire à ces localisations primaires. Nous rapportons deux cas de kyste hydatique pelvien primaire qui ont été diagnostiques respectivement chez les femmes âgées de 37 ans à 38 ans. Ces cas mettront l'accent sur les différentes caractéristiques de l'infection et les bénéfices qu'on peut tirer si l'on inclut des arguments épidémiologiques en faveur de l'emploi de l'approche diagnostique des masses annexielles. Key words: Hydatid cyst, Pelvic Ultrasonography INTRODUCTION: Hydatid disease, or echinococcosis, is a parasitic infection caused by the larval stage of the tapeworm Echinoccocus granulosus. This anthropozoonosis had long been endemic in the Mediterranean region, the Middle East, and South America 1, 2 . Morocco ranks amongst the countries most infested by this parasite and it has become a public health problem. Human are intermediate hosts, and develop cysts after ingesting the parasite's eggs. The definitive hosts are dogs, wolves, foxes and jackals passing their eggs of the parasite in their faeces. The cysts are mostly found in the liver (60%) and lung (15%)2, 3, but they can be located in any part of the body. Primary pelvic echinococcosis is exceptional even in endemic countries; it generates significant diagnostic difficulties as the symptoms are non specific. Imaging and specially ultrasonography (US) is the first line exam for diagnosis. It show pathognomonic signs of hydatid cyst and it's safe, non invasive, and relatively inexpensive. We report 2 cases of a primary and isolated pelvic hydatid cyst (HC) diagnosed post-operatively. CASE REPORT 1: A 37 -year-old, gravida 4, para 4 Moroccan woman, with no medical history was admitted to our hospital with chronic pelvic and abdominal pain that started one year earlier. The clinical examination didn't reveal any abdominal mass. The pelvic ultrasound showed a well-circumscribed hypoechoic mass in the left adnexal region, rounded, thin-walled and measuring 40 mm in diameter, with hyperechogenic components and signs of internal calcifications that suggested an ovarian dermoid cyst. Abdominal radiography however showed no calcification. The patient underwent surgery leading to the intra-operative discovery of a pinkish yellow cyst, thin-walled and measuring 4 cm. It was located on the lateral pelvic peritoneum near the bladder horn. The cyst was easily removed. Postoperative abdominal ultrasound and chest radiography didn't reveal any other location. Serological evaluation for hydatid disease was carried out with a negative result. The patient recovered uneventfully and was discharged on the 5th day post surgery. Pathologic examination revealed a hydatid cyst. At 24-month follow-up there were neither signs of recurrence nor other localizations of echinococcosis. CASE REPORT 2: A 48-year-old woman was admitted to our department, complaining of dragging pain in both iliac fossaes, dating from two months, with incontinence of urine on straining, occasional dysuria and feeling as if "something was coming down." There was no dyspareunia and no intermenstrual discharge. The menses were regular every 28 days and there was no dysmenorrheea. Physical examination revealed a mass on the right side of the uterus lying down to the pelvis, suggesting an ovarian tumor. Using ultrasonography, a uniloculated cystic mass, 15 x 10 x 5 cm in size with no internal echoes, was determined. By exploratory laparotomy, a 15 cm/ 10 cm / 7 cm in size cystic mass was found adhering to the right pelvic side wall and pushing the right ureter to the medial. The diagnosis of hydatidosis was suspected preoperatively and a complete cystectomy was performed in this patient without rupture, with precautionary measures such as placing gauzes soaked in hypertonic saline solution around the cyst. Before closing the abdomen the liver and others abdominal visceras were carefully palpated, however, no abnormalities could be detected. The abdomen was closed in layers without drainage. Pathology report confirmed the diagnosis of hydatid cyst. After surgery, the white-cell count was 15,000 per c.mm. (Polymorphs 75%, eosinophils 2%), and serologic evaluations for hydatid disease were positive. Postoperative abdominal CT did not find another cyst in the liver and a radiography of the chest taken before her discharge showed no abnormality. The patient was given Albendazole (orally 400 mg/day) therapy for 6 months after discharging from hospital on the 5th day. DISCUSSION: Pelvic echinococcosis caused by Echinoccocus Granulosus is rare with an incidence between 0.2 % and 2% 2. These cases are usually secondary to the accidental rupture of a liver hydatid cyst causing pelvic ecchinococcosis and often generating therapeutic difficulties. Primary pelvic location is exceptional and its diagnosis is difficult. Nearly 80% of all pelvic echinococcosis involve the genital area with the most frequent locations been the pelvic peritoneum, ovary and uterus 1,2,4,5. However, the cyst also can be localized in the fallopian tubes, anterior wall of the bladder or the broad ligament1. The pathophysiology of primary pelvic location is still not clearly established. Two theories have been suggested in the literature; firstly, the bloodstream pathway. Indeed, the cyst reaches the systemic circulation after avoiding the hepatic and pulmonary filters. Therefore, cysts can be located at any other point in the body. The kidney is the most common location of the urogenital tract representing 4-5% of visceral involvement, other localizations are the central nervous system (2%), spleen (2%), heart (0.5-2%), bone (0.9 to 2.5%), orbit, breast, diaphragm, testis, mediastinum, nasal cavity, thymus and pancreas (<1%)6. Secondly the heterological pathway which involve an intra-abdominal rupture of a hepatic cyst. Then, the released eggs and scolex bind in the Douglas, and continues their development. A secondary endothelialization excludes them from the peritoneal cavity. The intra-peritoneal cyst becomes extraperitoneal and suggestive of attachment to the pelvic cellular tissue. This failure leaves behind it a scar difficult to see. There is no evidence of the validity or the predominance of one of these theories. Echinococcosis is known as a disease of young adults, but in reality this condition can affect patients at any age. The infection may indeed occur during childhood but symptoms do not appear until adulthood 6. In fact, our two patients were respectively 37 and 48 years old. The hydatid disease is characterized by its slow evolution and its insidious allure. The symptoms of pelvic HC are not specific and may involve abdominal pain, swelling and pressure symptoms from neighboring organs. It also can stay asymptomatic for years. Other symptoms like menstrual irregularities and infertility have also been described6 , but there is no evidence of a relation with the cyst. We believe that fertility depends on the HC seat and pelvic damage degree (adhesions, rupture). A pelvic mass is not constantly found at examination. In our experience such as the patients mentioned above, following treatment patients are free of their earlier distressing symptoms. Ultrasonography is helpful for preoperative diagnosis; it shows the mass, specifies the location and examines its characteristics. Ahepatic ultrasound can be useful if there is an indication that the pelvic HC is secondary to the rupture of primary cyst in the liver, but it is difficult to suspect that the abdominal pain is caused by an echinococcal disease. Ultrasound features of pelvic HC are similar to hepatic HC5, 7, 8, 9 . The classification proposed by Gharbi 5, 7, can be adopted for other locations. Type I appears cystic and unilocular. Type II is a fluid filled with a floating membrane (the water lily sign)1,5,7. Type III has a typical honeycomb appearance1,5,7. Type IV is a heterogeneous mass, and Type V is a calcified lesion. However, if types II and III are specific to liver HC, there is no pathognomonic image for pelvic HC which is not suggestive of PHC at all. There are differential diagnoses for any type (table 1). Biological diagnosis is based on specific antigens, especially native Ag B which are recommended because tests using crude antigens are sensitive but not specific, therefore the enzyme-linked inmunosorbent assay (ELISA) system is a more specific antihydatid cyst antibody than countercurrent inmunoelectrophresis (CCIEP), while CCIEP is more sensitive in detecting antihydatid cyst antibody. A study showed that CCIEP could detect only 62 % of hydatid cases, whereas the pathology and ultrasound results were positive for 96.3% of cases11. We believe that diagnostic difficulties can be resolved by a systematic approach primary based on epidemiological evidence (country of origin, rural, contact with animals, personal or family history of hydatid disease), then ultrasound analysis guided by these elements would be easier and would specify the exact location and the characteristics of the mass. In case of doubt Computed Tomography can provide additional information because of its capability for better evaluation of the cystic masses, and better demonstration of their extension in the pelvic cavity as well as an excellent depiction of the visceral organs involvement. MRI may have some advantages over CT scanning in the evaluation of postsurgical residual lesions and recurrences8. Surgical intervention is the optimal treatment of the pelvic hydatid disease. Laparotomy avoids intraoperative rupture of the cyst. Surgery success depends on the location, adherence to adjacent organs, age and conditions of the patient. Some authors recommend using a scolicidal agent in the operating field to avoid dissemination in case of rupture. Mebendazole or Albendazole courses should be used as an adjunct to surgery when the resection is incomplete or as a treatment when surgery cannot be done1,2,9,10. Prognosis is usually favorable after treatment in primary and unique location, but more severe in disseminated disease. Fertility prognosis depends on HC seat and pelvic damage degree11. The prevention of hydatid disease relies mainly on general health education of the population, and on the organization of cattle slaughter. CONCLUSION The uniqueness of primary hydatid disease in gynecologic practice causes diagnostic problems. A comprehensive approach, including epidemiological, clinical and semiological analysis and ultrasound in any patient with a pelvic mass would help determine the diagnosis and an adapted therapeutic strategy. REFERENCES
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11030t1.jpg] |
| |||||||||

{kind=link}