 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 3, Sept, 2011, pp. 15-24 REVIEW ARTICLE Contraception in the Context of HIV/AIDS: A Review Chris O. Agboghoroma Department of Obstetrics & Gynaecology, National Hospital Abuja, Plot 132 central District (Phase 2) P. O. Box 5811 Garki, Abuja. Nigeria Tel: 08023342476 E-mail: agboschris@yahoo.com Code Number: rh11032 Abstract Over 50% of the 33.3 million HIV-positive persons are women within the reproductive age group. With increasing availability and use of highly active antiretroviral therapy (HAART), the prognosis, life expectancy and quality of life of infected persons has improved. HIV-positive women, like their uninfected counterparts, may desire to plan pregnancies, limit their families, or avoid pregnancy. The effective use of contraception by HIV-positive clients can contribute significantly to reduction in both sexual and vertical transmission of the virus. HIV-positive clients can use most of the available contraception methods including barrier, hormonal, intrauterine devices and sterilization. However, some antiretroviral drugs interact with hormonal contraceptives with potentials for reduction in efficacy. Dual protection with concomitant use of a more effective contraceptive method and male or female condom to prevent HIV and Sexually transmitted infections (STIs) is the standard. It is necessary to make provision for contraceptive service as part of comprehensive care for the HIV-positive client. (Afr J Reprod Health 2011; 15[3]: 15-24). Résumé Plus de 5o% des 33.5 millions des gens s éropositives sont des femmes qui sont encore en âge de procréer. Grace à la disponibilité croissante et de l'emploi de la thérapie antirétrovirale active élevée(TAAE), la pronostic, l'espérance de vie et la qualité de vie des gens atteints s'est améliorée. Les femmes séropositives, comme leurs homologues non atteints, peuvent désirer planifier des grossesses, limiter le nombre d'enfants ou éviter la grossesse. L'emploi efficace de la contraception par les clientes séropositives peut contribuer de manière significative à la réduction dans la transmission verticale du virus. Les clientes peuvent se profiter des méthodes de la contraception disponible y compris la barrière, l'hormonal, les dispositifs utérins et la stérilisation. Néanmoins, certains médicaments antirétroviraux réagissent avec des hormono-contraceptifs qui ont la capacité de réduire l'efficacité. La double protection avec l'usage concomitant d'une méthode contraceptive plus efficace ainsi que le préservatif pour homme ou pour femme pour prévenir le VIH et les maladies sexuellement transmissibles(MST) demeure la norme. Il faut prévoir un service contraceptif comme faisant partie des soins compréhensif pour les clientes séropositives. Key words:AIDS, HIV, contraception, family planning, highly active antiretroviral therapy (HAART), condom
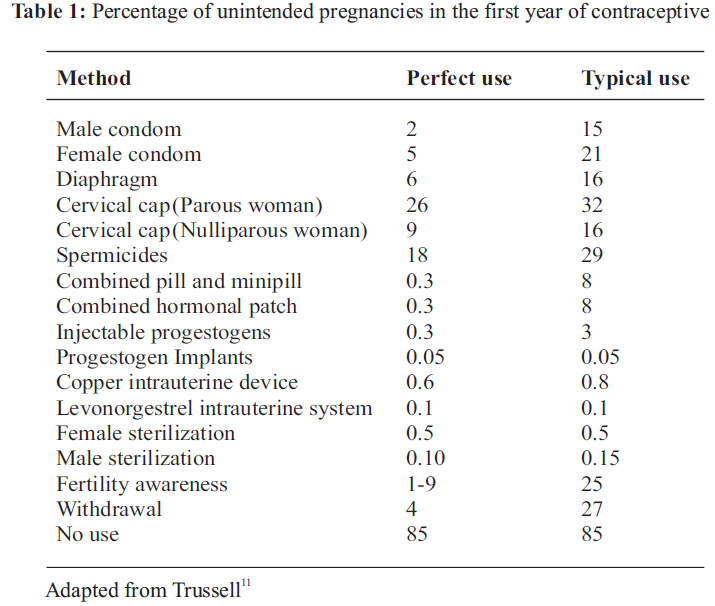
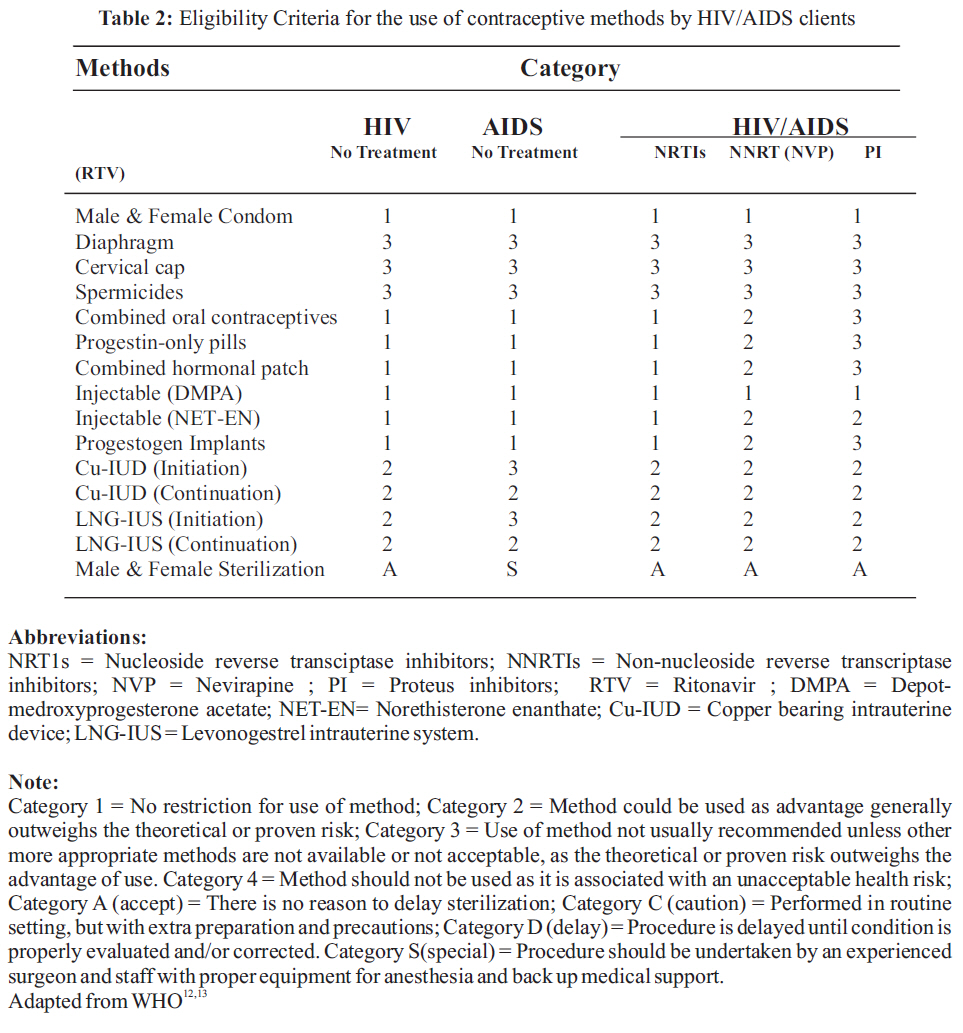
Introduction One major consensus at the International Conference on Population and Development (ICPD) in 1994 was the rights of women to decide freely on matters related to their sexuality, including sexual and reproductive health, free of coercion, discrimination and violence, and the need to improve access to services so that couples and individuals can decide freely the number, spacing and timing of their children1 . HIV positive clients are also entitled to these rights. The increasing availability and use of highly active retroviral therapy (HAART) has improved the prognosis, life expectancy and quality of life of people living with HIV.2 As a result of the global campaign for HIV testing and counseling an increasing number of people who are HIV infected now know their status. It is imperative that their reproductive health needs including family planning is addressed. This will not only satisfy their innate desire but can have far reaching positive effects on their health and reduction in the burden of HIV in the society through the prevention of unintended pregnancies and HIV spread. Family planning services should be provided as part of comprehensive reproductive health care for the HIV-positive client.3 This article identifies the link between contraception use and the control of HIV/AIDS. It also reviews the methods of contraception, their usefulness and applications in the context of HIV/AIDS. Contraceptive use and HIV/AIDS Prevention The use of contraception had been advocated on three major grounds -demography (population control), health (women and children) and human (women) rights. In recent times the use of contraception has been identified as a potent instrument in the control of HIV/AIDS in women and children. According to UNAIDS, 4 as at 2009 there were 33.3 million persons living with HIV/AIDS and over 50% of the infected adults were women who acquired the infection predominantly through heterosexual route. Children (under 15 years) account for 2.5 million of the infected population and majority (90%) were acquired through mother-to-child transmission route. Over 90% of the yearly 420,000 new infections in children occur in Africa. The World Health Organization (WHO) and United Nations agencies in 2002 recommended a four -pronged strategy to address the issue of paediatric HIV/AIDS.5 The first strategy deals with prevention of HIV infection especially in young women. The second strategy supports the prevention of unintended pregnancy in HIV positive women. The third strategy focuses on the reduction of HIV transmission from an infected woman to her child. The fourth strategy promotes treatment, care and support for the HIV infected woman, her partner and children. Much attention has however been placed on the third strategy which include use of antiretroviral drugs, safe delivery practices and avoidance of breastfeeding. In advanced countries with developed health systems and infrastructure, application of these interventions have led to reduction of mother-to-child transmission (MTCT) risk from over 30% to less than 2%.6 There is concern however, that in sub-Saharan Africa with poor health infrastructure, limitations in coverage, low use of services and drug efficacy, implementation of these interventions will be difficult and the impact on reduction of paediatric HIV/AIDS will be minimal. In a cost-effectiveness analysis of Prevention of Mother-to -Child Transmission (PMTCT) programmes in eight African countries, the authors7 found that using the third strategy alone will reduce HIV infections in infants by between 2% and 12% only. Comparable investments in programmes to improve contraception use have great potential for reduction in the number of pediatric infections. In sub-Saharan Africa where the prevalence and burden of HIV/AIDS is high, contraceptive prevalence rate (CPR) is also low. A recent United Nations report showed that the CPR for sub-Saharan Africa in 2010 was 28% compared with the global average of 62%.8 It has been estimated that an increase in CPR in sub-Saharan Africa with corresponding reduction in primary HIV infections and unintended pregnancies in HIV infected women has potential to decrease the proportion of infants infected with HIV by 35 - 55%.9 Hence the provision of appropriate contraceptive information, counseling and services will play a significant role in reducing the burden of HIV and AIDS in Africa. Contraceptive Counseling for Couples Living with HIV/AIDS HIV-positive women should be given information and counseling (including efficacy and side effects) on all methods of contraception and supported in making an informed choice. Couple counseling is preferred to enlist the support and cooperation of both partners in decision making. There is also the need to educate women whose partners failed to come for couple counseling, on how to approach and secure their support. Medical, sexual and drug history are necessary part of routine assessment. The means of transmission of HIV and other STIs should be explained to clients. Screening for STIs and treatment should be offered as necessary. Counseling should also emphasize the need to adhere to antiretroviral therapy and the chosen contraceptive method(s). The final decision on contraceptive method should take into consideration the following -stage of HIV infection, CD4 count, type of antiretroviral medication, personal preference, pill burden and adherence, concomitant disease like hepatitis B and C, osteoporosis and culture. HIV-positive women should be advised to use dual protection 10 which entails the simultaneous use of barrier method (condom) to reduce the risk of STIs/viral infection or super-infection and a more effective contraception such as hormonal, intrauterine device or sterilization. Modern Methods of Contraception in HIV Clients The modern methods of contraception include -barrier methods, hormonal methods, intrauterine devices and surgical methods. With exception of the surgical methods which are permanent, the other methods are temporary and reversible. The effectiveness and safety profile of the various methods varies. The percentage of unintended pregnancies in the first year of contraceptive - perfect use (theoretical failure rate) and typical use for the various methods as reported by Trussell 11 is included as Table 1. The World Health Organization (WHO) currently assigns categories (category 1 - 4 for nonpermanent methods and category A, C, D and S for surgical methods) to the various contraceptive methods based on safety criteria.12,13 This enables the determination of the suitability of method(s) for a given medical situation. Table 2 shows the categories of the various contraceptive methods in relation to HIV/AIDS status and use of antiretroviral drugs. Barrier methods The barrier methods include the male and female condoms, diaphragm and cervical cap. Their contraceptive effectiveness is low, hence additional methods of contraception is needed when they are used. There is no known drug interaction between antiretroviral drugs and barrier methods. Male condom The use of a condom has become very important as it serves a dual purpose of contraception and prevention of STIs and sexual transmission of HIV. 14 However, its main drawback is that it requires male participation which may be difficult to negotiate especially in power imbalanced relationship. Condoms are user dependent and can only be used at the time of coitus. Condom may be made of latex, polyurethane (thin, soft, pliable plastic) or natural animal membranes (e.g. Lamb caecum). Polyurethane condoms are more likely to slip and break than latex condoms because they do not adhere to the penis. Natural animal membranes do not provide same level of protection as synthetic products. Condoms can vary in thickness from 0.03mm to 0.09mm and may contain benzocaine to delay ejaculation. The transmission of HIV from a man to a woman is more efficient than from a woman to a man due partly to the large surface area of vaginal mucosa exposed to the virus. The theoretical risk of HIV transmission from an infected male to an uninfected female partner is 0.1 -0.3% per act of intercourse and that of an infected female to an uninfected male partner is 0.03 - 0.09% per act of intercourse, provided the couples are in monogamous relationship, are not engaged in any other risky activities, and absence of genital injury/infections.15 Male condom use offers a high degree of protection against sexual transmission of HIV and STIs. Apart from abstinence, the condom is the only recommended method of reducing sexual transmission of HIV.16 In sero-concordant couples where both partners are HIV-positive, condom use may be necessary not only to prevent pregnancy and STIs but also to prevent HIV drug resistant super infection. In sero-discordant couples, where one partner is HIV-positive and the other negative, consistent condom use provides about 80% -95% protection.15, 17, 18 The effectiveness of the condom is dependent on its correct and consistent use. Condom accidents are reported in 1-2% of users.19 The unintended pregnancy rate with male condom use is relatively high hence additional contraception (dual contraception) should be used to prevent pregnancy. The use of antiretroviral drugs for post-exposure prophylaxis following sexual exposure (PEPSE) may become necessary in sero-discordant relationship in condom accidents.20 Couples who opt to use male condom as their only means of contraception should also be made aware of emergency contraception. Female condom The female condom is a female -initiated barrier method which can serve as contraception and prevention of STIs and HIV. It is made of polyurethane sheath, with a flexible ring at either end. The inner ring at the closed end is inserted into the vagina, and the outer ring is placed over the perineum. The female condom is 17cm (about 6.5inches) long, similar in length to an unrolled male condom. It has also been shown to be effective in preventing HIV transmission. It can be worn up to eight hours prior to sexual intercourse. As its use is under the control of the female, it presents an advantage in settings where the female may not be in a position to negotiate male condom use. The unintended pregnancy rate with female condom use is high (higher than with a male condom) hence additional contraception (dual contraception) should be used to prevent pregnancy. Spermicide Available spermicides include nonoxynol 9 (N-9), octoxynol-9and benzalkonium chloride. The most common spermicide preparations contain N-9 which acts by damaging the sperm cell membrane. It is available in different formulations as foam, cream, gel, and suppositories. It may be used alone or with a condom or diaphragm. It does not reduce pregnancy rates when compared to non-spermicidally lubricated condoms. It offers no protection against STIs and HIV. It causes epithelial irritation and when used repeatedly can result in ulceration thereby facilitating STIs and HIV transmission.21, 22 The use of N-9 is therefore not recommended. Re-infection with a different strain of HIV may be facilitated by the use of N-9. There are on-going efforts to identify safe spermicides (microbicides) that can serve as both contraception and STIs/HIV prevention. Diaphragms and cervical caps The diaphragm and cervical caps are contraceptive methods that cover mainly the cervix leaving most of the vaginal epithelium uncovered and exposed to semen. Its recommended use with nonoxyno l-9 which can cause vaginal mucosa irritation and ulceration makes the use of the diaphragm and cervical cap unsafe and therefore not recommended in the context of HIV/AIDS. Hormonal contraception Hormonal contraceptive methods include - combined oral contraceptive pill, combined contraceptive patch, progestogen-only pill, injectable progestogens and progestogen-only sub-dermal implants. They are very effective contraceptives. The effect of hormonal contraception on HIV progression is not fully known. Available evidence suggest no association between hormonal contraceptive use and changes in HIV RNA viral load and CD4 cell counts in HIV-positive women.23 There are also controversies as to the effect of hormonal contraceptives on HIV transmission. The available reports are inconsistent regarding whether there is increased risk in transmission. While some reports linked increased risk of HIV transmission with the use of hormonal contraception,24, 25 other studies, could not demonstrate such association.26 However, the efficacy of some hormonal contraceptives may be affected in certain situations. Some liver enzyme-inducing drugs including antiretroviral medications and antituberculous drug (rifampicin) that are commonly used by HIV-positive patients may interact with the steroids in hormonal methods with potential to decrease or increase the efficacy and safety of either of the drugs.27,28 Amongst the antiretroviral drugs, nucleoside reverse transcriptase inhibitors (NRTIs) generally do not interact with steroids, the non -nucleoside reverse transcriptase inhibitors (NNRTIs) -nevirapine reduces while efavirenz increases steroid levels. The protease inhibitors (PIs) -ritonavir, nelfinavir reduce while atazanavir, amprenavir and indinavir increase contraceptive steroid levels. Although the clinical significance of the interactions is yet to be fully elucidated, the impact of ritonavir on steroids is considered significant hence the recommendation to avoid hormonal contraceptives in clients using ritonavir- based HAART. In addition, hormonal contraceptives dose in women on some antiretroviral drugs may need to be increased or alternative contraception provided. 13 There is no restriction on the use of any of the hormonal methods for women who are HIV-positive and are antiretroviral naïve. In order to prevent sexual transmission of HIV, condom use is recommended in addition to any hormonal contraception. Combined oral contraceptive pill (COCP) Ethinylestradiol (EE) is the oestrogen commonly used in combined oral contraception (COC). The progestogens may include norethisterone, levonorgestrel, desogestrel, gestodene, norgestimate and drospirenone. In current practice the low-dose COCs containing 20 -35 µg EE is preferred to the older COCs which contains 50 µg EE or more. The COC acts mainly by inhibiting ovulation through its effect on the hypothalamic-pituitary-ovarian axis, it also affects the cervical mucus and endometrium. In order to ensure the desired efficacy some authorities recommend a COC with at least 30 - 50µg EE in HIV-positive women who are using liverenzyme-inducing drugs and wish to start or continue the COC.13,15 The use of other methods not affected by liver enzyme-inducing drugs is an option of care. In addition to the potential effects of liver enzymeinducing drugs, other factors that may affect the efficacy and safety of COCP in HIV- positive clients include antiretroviral associated gastrointestinal side effects, acute or chronic liver damage from hepatitis B and C co-infections and alcohol consumption. The increased pill burden may also serve as a disincentive affecting adherence in women who are on HAART. The condom is also recommended to compensate for any potential decreases in contraceptive efficacy. Combined contraceptive patch This is a transdermal patch that delivers 20 µg EE and 150µg norelgestromin daily. It is applied weekly for 3 weeks followed by a 7-day patch-free interval. The reported efficacy is similar to COCP but compliance with its use is better.15 Like the COCP, liver-enzymeinducing drugs may affect their effectiveness. Hence additional contraception such as condom is recommended. Progestogen-only pill (POPs) The POP is an alternative in women who cannot use oestrogen containing pills. The traditional POPs contain levonorgestrel, norethisterone or ethynodiol diacetate and act mainly by cervical mucus thickening and endometrial atrophy. The newer desogestrel POP acts mainly by inhibition of ovulation. The occurrence of menstrual irregularity with its use is a major disadvantage in HIV-positive patients. Some antiretroviral drugs also affect its efficacy; hence when used there will be a need for an additional method of contraception such as a condom which can serve a dual purpose of contraception and STI / HIV prevention. Injectable progestogens The two injectable progesterone-only contraception are depo-medroxyprogesterone acetate (DMPA) and norethisterone enantate (NET-EN) given at 12 and 8 weekly intervals respectively. DMPA is not affected by liver enzyme-inducing drugs and hence may be used in patients on various combination of HAART without the loss of its effectiveness and can be given at the same interval as in uninfected women. The amenorrhea that may result in up to 35% of clients is beneficial in reducing the problem of anaemia and HIV spread. HIV infection and use of some antiretroviral drugs have been associated with increased bone loss.15 Prolonged use of DMPA tends to reduce bone density, special precaution including bone density scan prior to initiation of DMPA is therefore necessary in women at high risk of low bone density.29 Though the use of progestogen -only injectable may be safe and effective in reducing unintended pregnancy, it is advised that dual contraception should be practiced to reduce the risk of STIs and HIV transmission. Progestogen-only sub-dermal implants The two main progestin hormonal implants contain etonogestrel and levonorgestrel. The etonogestrel implant acts by inhibiting ovulation. Like other progestin-based contraceptives, it also creates hostile, thick, cervical mucus and atrophy of the endometrium. It is very effective, non-user dependent and fully reversible. Implanon ® contains 68mg of etonogestrel contained in one rod and may be used for 3 years following insertion. Jadelle® contains 75mg of levonorgestrel in 2 rods and may be used for up to 5 years. They have the non contraceptive advantage of inducing amenorrhea with implications of reducing anemia and HIV transmission through reduction in viral shedding. As with most of the other hormonal contraception, some antiretroviral drugs interact with the steroids with potential to reduce their efficacy. The use of additional (dual contraception) method or a different contraceptive method may become necessary in HIV positive clients on HAART. Intra-uterine devices The two main types of intrauterine device (IUD) currently in use are the copper-bearing intrauterine device (Cu-IUD) and steroid-based levonorgestrel intrauterine system (LNG-IUS) Copper-bearing intrauterine device (Cu-IUD) The Cu-IUD acts by preventing fertilization and implantation and may remain effective for 5 -10 years. It is an effective method of contraception. Although it does not increase overall ectopic pregnancy rates but when pregnancy occurs it is more likely to be an ectopic. There were initial concerns on theoretical risk and potential for pelvic infections in HIV-positive clients who use IUD. However, following recent research findings of no significant difference in the rate of complications between HIVpositive and HIV- negative women using the IUD, 30 WHO removed restrictions to use of IUD by HIV positive clients.12 There is also no evidence of increased transmission of HIV to partners when an IUD is in-situ. Under the current WHO guidelines, most HIV infected women generally can initiate and use IUDs and users who become infected with HIV may continue using the device. However, IUD insertions are not recommended in AIDS patients who have not commenced or are not responding to antiretroviral treatment, as their reduced immune state makes them more vulnerable to pelvic inflammatory disease. HIV infected IUD users who develop AIDS may generally continue using the device. The main disadvantage with the use of Cu-IUD is an increase in the duration of menstrual bleeding with implications for HIV transmission and anemia in those who are already prone to anemia due to menorrhagia from uterine fibroids. Cu-IUD may therefore be used in HIV-positive women after risk assessment and exclusion of baseline cervical infections. The concomitant use of condom is recommended to prevent HIV and other sexually transmitted diseases. Levonorgestrel intrauterine system (LNG-IUS) The LNG-IUS releases 20 µg of levonorgestrel per day into the uterine cavity and remain effective for 5 years. It acts mainly on the endometrium preventing implantation. It also causes cervical mucus thickening. Its effectiveness is comparable to the Cu-IUD. Although the effect of HAART on this method is not fully known, its recommended use in the HIVpositive is as with the Cu-IUD. One advantage of its use is the reduction in menstrual blood loss with potential for reduction in sexual transmission in HIV and prevention of anemia. The concomitant use of the condom for dual contraception is recommended. Male and female sterilization In the early stage of the HIV epidemic when mortality associated with the condition and vertical transmission rates were high, female sterilization was considered the preferred method of family planning. However with the availability and use of HAART and successful implementation of strategies for PMTCT, female sterilization is no longer justifiable except on clients' choice after appropriate counseling. Sterilization is a safe, highly effective and permanent method of contraception especially for couples who have completed their family. Female sterilization (tubal ligation) does not affect HIV transmission. Similarly male sterilization (vasectomy) does not prevent HIV transmission as the virus may be present in the semen fraction from seminar vesicle and prostate. The use of condom is recommended for clients who have undergone sterilization to ensure dual protection. Other Methods Emergency Contraception Emergency contraception is designed to prevent conception after unprotected sexual intercourse (UPSI) or after the failure of another contraceptive method such as condom slippage or breakage. The original method as described by Yuzpe 31 involves the use of combination oral pills given within 72 hours of intercourse, and the dosage repeated in 12hrs. The major side effect is the occurrence of nausea and vomiting due to the high content of oestrogen (each of the 4 tablets containing 50µg EE). Efforts to reduce the side effects, improve compliance and efficacy has led to the current recommendation of the levonorgestrel 1.5mg single dose taken within 72 hours after an unprotected sexual intercourse. Pregnancy risk is reduced by at least 75% if properly used. When there are no contraindications and in appropriate patients, Cu-IUD may also be used as an emergency contraception within 5 days of UPSI or contraception failure to prevent pregnancy. Due to concern of the effect of liver enzyme-inducing drugs on LNG, clients on HAART are counseled to use the Cu-IUD that does not have such effect. When this is not feasible or acceptable, doubling the dose of LNG to 3.0mg has been recommended.15 Fertility awareness-based (natural family planning) methods The fertility awareness, periodic abstinence or natural family planning methods include the rhythm or calendar method, cervical mucus method, symptothermal method and hormone monitoring methods. The goal is to avoid having unprotected vaginal intercourse during the most fertile period of a woman's menstrual cycle. The period of maximal fertility begins 5 days before the day of ovulation and ends the day after ovulation. These methods require abstaining from sex or using barrier methods only during the fertile days of the menstrual cycle in order to prevent pregnancy. The fertility awareness methods and the withdrawal method are traditional methods of family planning and are associated with high contraceptive failure rate. As unprotected sexual intercourse occurs, the partners remain exposed to STIs and HIV. In the context of HIV prevention, they are therefore not recommended. Conclusion The control of the spread of HIV in both adults and children is a major reproductive health challenge. Most of the available contraceptive methods can be used by the HIV-positive clients. The effective use of contraception in the HIV positive population has potential in reducing the incidence of paediatric HIV. With the exception of spermicides (nonoxynol-9), there is no evidence to suggest that the available contraceptive methods facilitate the acquisition and transmission of HIV. They also do not affect progression of HIV disease. The effectiveness of some of the contraceptive methods however, may be affected by liver enzyme-inducing agents including some antiretroviral and antituberculous drugs that the HIV-positive client may be using. With appropriate counseling, review of medication, medical history and clinical assessment, the HIV-positive clients can be offered an appropriate and effective contraception. Efforts should be made to promote dual protection. REFERENCES
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11032t1.jpg] [rh11032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}