 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
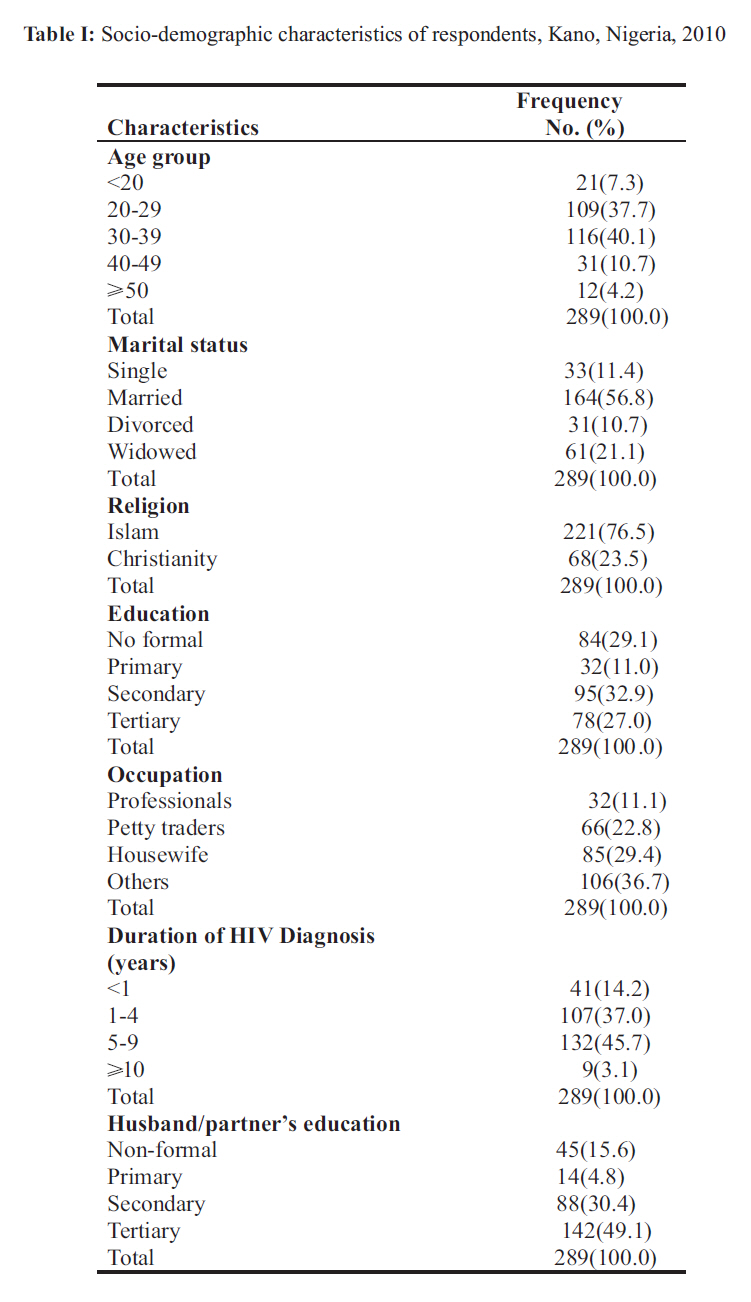
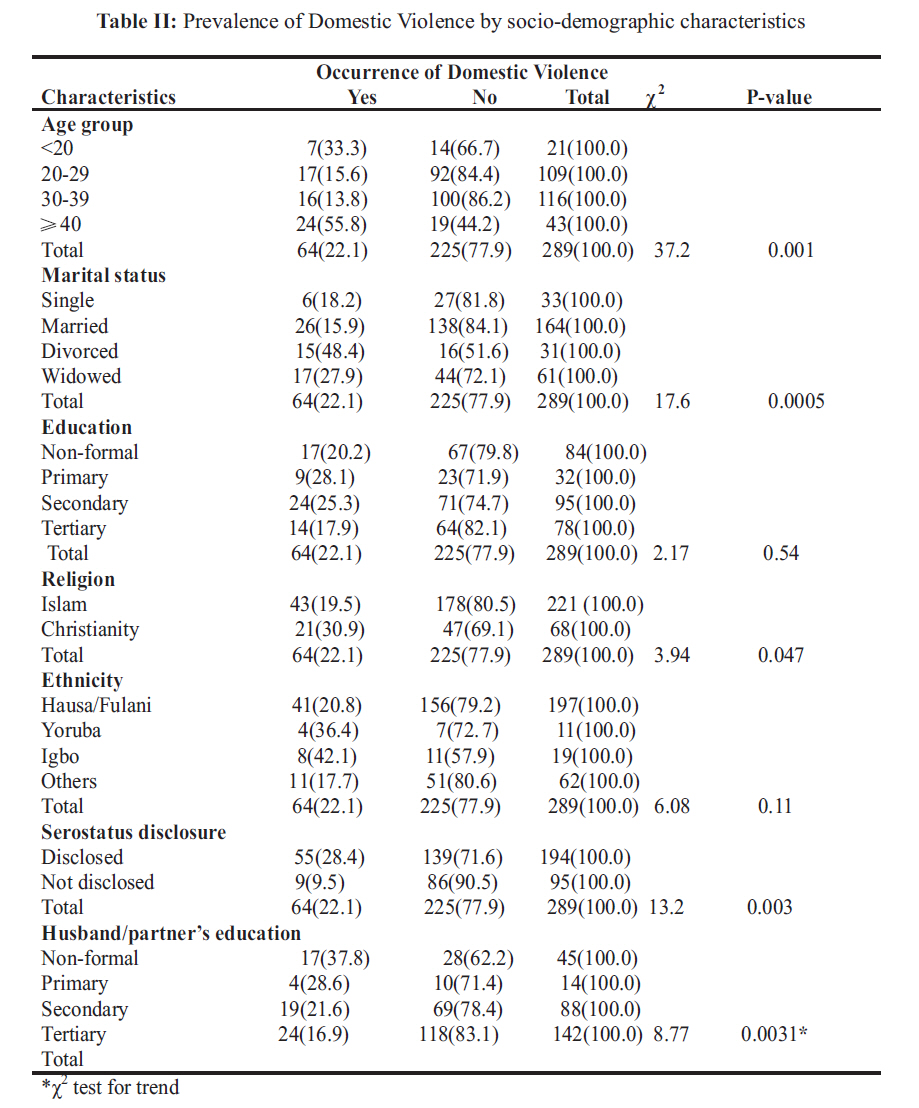
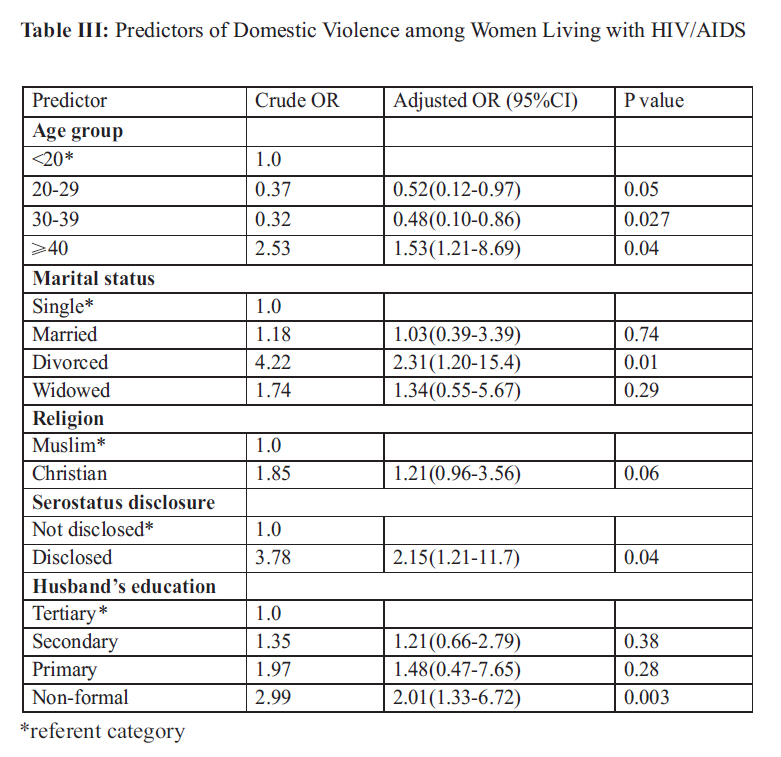
African Journal of Reproductive Health, Vol. 15, No. 3, Sept, 2011, pp. 43-53 ORIGINAL RESEARCH ARTICLES Domestic Violence among women living with HIV/AIDS in Kano, northern Nigeria 1 Zubairu Iliyasu, 1 Isa S Abubakar, 2 Musa Babashani, and 3 Hadiza S Galadanci 1Department of Community Medicine, Aminu Kano Teaching Hospital &Bayero University Kano, Nigeria. Code Number: rh11034 Abstract Despite the increased risk of domestic violence among women living with HIV/AIDS, its burden has not been adequately explored in many developing countries including Nigeria. Using interviewer administered questionnaires we assessed the prevalence and risk factors for domestic violence among 300 HIV seropositive women attending a teaching hospital in northern Nigeria. Participants have been diagnosed HIV positive for an average of 6.7 years; 66.3% were seroconcordant with their intimate partners while 16.3% were serodiscordant, the rest 17.4% did not know the partner's status; 67.1% had disclosed their status to their partners; and 64(22.1%) [95%CI (17.5% to 27.4%)] had experienced domestic violence following HIV diagnosis. Specifically, 30.0% (n=19) experienced physical violence (slapping, kicking and punching), 59.3% (n=38) reported verbal violence (insults, threats) and 10.7% (n=7) endured emotional violence. None was sexually assaulted. Predictors of domestic violence were the woman's age, marital status, disclosure and partner's educational status. This calls for urgent steps and strategies for prevention, protection and post-test counseling on disclosure to avert this human right infringement. (Afr J Reprod Health 2011; 15[3]: 43-53). Résumé Malgré le risque de la violence domestique qui s'accroit chez les femmes séropositives, on n'a pas encore suffisamment exploré son fardeau dans plusieurs pays en voie de développement y compris le Nigéria. A l'aide des questionnaires administrés par l'enquêteur, nous avons évalué la prévalence et les facteurs de risque de la violence familiale auprès de 300 femmes séropositives qui fréquentent un hôpital au nord du Nigéria. Les participantes ont été diagnostiquées comme étant séropositives depuis une période de 6,7 ans au moyen ; 66,3% étaient séroconcordantes avec leurs partenaires intimes, alors que 16,3% étaient séroconcordantes, le reste ne connaissais pas la condition de leurs partenaires ; 67,1% avaient révélé leur condition à leurs partenaires ; et 64(22,1%) [95%CI (17,5% jusqu'à27, 4%)] avaient vécu une violence familiale suite à un diagnostic du VIH. En particulier, 30,0%(n=19) ont vécu la violence physique (gifle, coups de pied et coups de poing), 59,3% (n=38) ont signalé la violence verbale (insultes, menaces) et ont toléré la violence émotionnelle. Nulle n'a été agressée sexuellement. Les indices de la violence familiale étaient l'âge de la femme, son état civil, la révélation et le niveau de scolarisation du partenaire. Ceci exige des démarches et des stratégies urgentes pour la prévention, la protection et le conseil d'après le test, suite à la révélation afin d'éviter la violation de ce droit de l'homme. Key words: Women, HIV/AIDS, Domestic Violence, Nigeria Introduction Women comprise about half of the 33.4 million people living with HIV/AIDS worldwide. 1 In sub-Saharan Africa, where the epidemic is worst, they make up an estimated 57% of adults living with HIV/AIDS, and three quarters of young people living with HIV/AIDS on the continent are young women.1 Domestic violence is defined as a pattern of abusive behaviors by one or both partners in an intimate relationship such as marriage, dating, family, friends or cohabitation.2 It has many forms including physical aggression (hitting, kicking, biting, shoving, restraining, throwing objects) or threats thereof. Other types include; sexual abuse, emotional abuse, controlling or domineering, intimidation, stalking, passive/covert abuse and economic deprivation.2 Over the past decade, the issue of domestic violence in developing countries has evolved from relative obscurity to a primary concern among researchers and policy makers who are interested in women's health and status.3 It has also become a central focus of the international human rights movement. There is also growing awareness of the links between domestic violence and HIV/AIDS.3-5 A major concern is that women who test for HIV and share test results with partners may be at increased risk of violence.6 Despite the growing interest about domestic violence, studies on the magnitude, precipitating factors and consequences for women and their families remains scarce in most developing countries including Nigeria. In the absence of such data, many policy makers have been reluctant to address the issue, given that it touches on what has traditionally been viewed as a highly personal and sensitive aspect of family life. The paucity of information has similarly impeded the formulation of sound and effective programs to address it, most notably in the area of prevention. In Nigeria, studies on domestic violence have been conducted among some groups of women considered at risk.7, 8 but none of these was conducted among women living with HIV/AIDS. These women represent a more vulnerable group for domestic violence and the impact on them is more severe both in terms of psychological, physical, and pathological consequences.1 Northern Nigeria has a distinct culture and tradition of early marriage, female seclusion ('Purdah'), low status and levels of female literacy and education. Others include practice of polygamy, desire for large families, strong cultural resistance to birth control and great sensitivity about providing reproductive health information or services to women and youth. Family disputes are not perceived as violations of civil rights and are therefore not expected to be reported to law enforcement agents. These factors may modulate the experiences of women living with HIV/AIDS in this region compared to their counterparts elsewhere. This is likely to affect the level of reporting, assertiveness and redress following violation of rights. This study was therefore conducted; to estimate the prevalence of domestic violence among women living with HIV/AIDS attending Aminu Kano Teaching Hospital, Kano Nigeria and to identify social and demographic characteristics of women experiencing violence. The information obtained could inform policy makers, human right groups, programmers and the judiciary about the magnitude of this problem and the need to implement strategies that would protect these women. Methodology Setting Established in 1988, the Aminu Kano Teaching Hospital is situated in Kano city, the commercial nerve centre of northern Nigeria with over 9 million people. 9 It is a 500-bed hospital which receives patients from within Kano, the neighbouring states of Jigawa, Katsina, Kaduna, Bauchi and Zamfara states. The majority of patients are indigenous Hausa Fulani, although the Igbo and Yoruba ethnic groups are well represented. Most of the people are farmers, traders, businessmen and civil servants. The hospital operates a multidisciplinary specialist clinic located at Prof. S.S. Wali centre for HIV/AIDS patients five days a week. Investigations and antiretroviral drugs are provided free of charge to all patients. Study participants The study population consisted of female HIV/AIDS patients attending Aminu Kano Teaching Hospital HIV/AIDS specialist clinic from the 1st to the 31st of May 2010. The systematic sampling technique was used. All women with HIV, who had made at least one visit to the ART unit, were included in the study. Those clients that were too ill to participate in an interview were excluded from the study. During recruitment, participants were given an explanation of the purpose of the study and asked if they would like to participate. They were assured of confidentiality. Upon approval, the informed consent process was described and participants were asked to read and sign the consent form after all questions were answered. Those without formal western education had the consent translated to them in the locally spoken Hausa language and they elected to thumbprint. Informed consent was secured from each participant. Participation in the study was voluntary and no incentives were provided. Ethical clearance was obtained from the Aminu Kano Teaching Hospital institutional review board. Support was provided to women interviewed through referral to services as needed. Study design The study was descriptive and cross-sectional in design. A sample size of 300 was obtained using the hypothesis method 10 and based on prevalence of domestic violence among women in a previous study.11 Our assumptions were a 95% confidence limit, a 5% margin of error and allowance made for 10% attrition rate. Study instrument and data collection A pre-tested structured interviewer-administered questionnaire containing open and closed ended questions was used. The questionnaire was adapted from one used in the Nigeria Demographic and Health Survey (2008).12 It was made up of the following moieties: questions on socio-demographic characteristics, length of time since HIV diagnosis, occurrence of domestic violence following HIV diagnosis, type of violence, consequences, response and support. Specifically, in order to measure domestic violence in this survey, women living with HIV/AIDS were asked questions adopted from the shortened Conflict Tactics Scale (CTS).13 They were asked the following questions: Does your husband/partner or any family member ever do any of the following things to you following your HIV diagnosis? (a) Verbally abused you? (b) Push you, shake you, or throw something at you? (c) Slap you? (d) Twist your arm or pull your hair? (e) Punch you with his fist or with something that could hurt you? (f) Kick you, drag you or beat you up? (g) Try to choke you or burn you on purpose? (h) Threaten or attack you with a knife, gun or any other weapon? (i) Physically force you to have intercourse with him even when you did not want to? (j) Hurt your feelings deliberately? Revalidation of the tool was done at Murtala Mohammed Specialist Hospital, Kano. Participants engaged in the latter exercise were invariably excluded from the study. All women fulfilling the inclusion criteria were interviewed during their exit from the anti-retroviral therapy (ART) units. Based on the average daily attendance at the clinic, a sampling interval was determined. The first respondent was determined by picking a random number between one and the sampling interval. Subsequent respondents were identified by adding the sampling interval to the preceding respondent's serial number. The interviews were continued until the required number of respondents was obtained. Four Hausa speaking female medical students specifically trained in the conduct of interviews collected data. The authors supervised the data collection process. Data analysis The data from the questionnaires were entered and analyzed using SPSS version 16 software.14 Odds ratios (95% confidence intervals) were used to determine the association of different factors with violence against women living with HIV/AIDS. Logistic regression analysis was used to assess the relative effect of determinants. Adjustment was made for predictor variables that were significantly related to the outcome variable at the bivariate level. AP<0.05 was considered statistically significant in all tests of significance. Results Socio-demographic characteristics Out of 300 respondents approached for the study, 289 agreed to participate giving a response rate of 96.3%. The age range of the respondents was 18 to 70 years with a mean age (±SD) of 31.4 (±7.74) years. Table I shows that majority of the respondents 221 (76.5%) were Muslims, most 197 (68.2%) of whom belong to the Hausa/Fulani ethnic group. Other respondents were Igbo (6.6%), Yoruba (3.8%) or members of other minor Nigerian tribes (Ebira, Kanuri and Igala) (21.4%). Only 11.3% were employed in the government civil service. Nearly a quarter (22.7%) were petty traders, 29.3% were housewives and the rest were students, businesswomen and seamstresses. About (11.0%) participants had primary school education, 59.9% had at least secondary school education while the rest (29.1%) had no formal education. Most respondents were married (56.8%), others were either widowed (21.1%), single (11.4%) or divorced (10.7%). Up to 40.7% of married respondents were in polygamous unions. Respondents had known they were HIV-positive for periods ranging from 3 months to 14 years with an average of 6.7 years. Of all respondents, (67.1%, n=194) had disclosed their HIV serostatus to their partner. Of those whose partners' have been tested, two-third had concordant partners (66.3%), while (16.3%) had discordant partners, the rest (17.4%) did not know their husband/partner's test result. There was no significant difference between sociodemographic characteristics of those that disclosed their serostatus to their partners compared to those who did not. Prevalence of Domestic Violence Of the 289 respondents, 64(22.1%) [95%CI (17.5% to 27.4%)] admitted having experienced domestic violence since being diagnosed HIV positive. Of those who experienced violence, 30.0% (n=19) experienced physical violence (slapping, kicking and punching), 59.3% (n=38) reported verbal violence (insults, threats) and 10.7% (n=7) endured emotional violence. However, there was an overlap in the types of violence experienced. For instance, nearly half (n=8) of women who experienced physical violence also reported verbal violence. Similarly, nearly all women who faced emotional violence (n=6) were also verbally insulted or threatened with divorce. There was no reported case of sexual violence. Table II shows that the experience of domestic violence varied by socio-demographic characteristics. By age, the prevalence was highest among women in the youngest (<20 years) and oldest (≥ 40 years) age brackets and lowest among those in the 30-39 age group. This difference was statistically significant (P=0.001). Non-Muslim women were more likely to have experienced domestic violence since HIV diagnosis compared to Muslim women (30.9% vs. 19.5% respectively, P=0.047). Divorced women had the highest (48.4%) experience of domestic violence, followed by widows (27.9%). By ethnicity, Hausa/Fulani women (20.8%) and those from other minor Nigerian tribes (17.7%) had the lowest experience of domestic violence following HIV positive diagnosis. In contrast, women from the other two major ethnic groups in the country, namely, Igbo and Yoruba were at increased risk of domestic violence as shown by a prevalence of 42.1% and 36.4% respectively. However, this variation by ethnicity was not statistically significant (P=0.11). Women that disclosed their HIV serostatus to their husbands/partners were more likely to experience domestic violence compared to those who have not (28.4% vs. 9.5% respectively, P=0.003). Furthermore, differences in experience of domestic violence by respondent's education were not statistically significant. In contrast, there was an inverse relationship between partner's educational level and the prevalence of domestic violence (P=0.0031). Abused women most times did not report at all (42.2%, n=27) or reported to their own family (20.3%, n=13), husband's family (14.1%, n=9), religious leaders (10.9%, n=7) or husband's friends (6.3%, n=4). Only (6.3%, n=4) reported to the police. The perpetrators of domestic violence include husbands (51.6%, n=33), boyfriends (18.8%, n=12), co-wives (14.1%, n=9), family member (9.4%, n=6) and others (6.3%, n=4). Predictors of domestic violence Table III shows that the respondent's age is associated with the risk of violence, with the oldest women having more than 50% increased risk compared to their youngest counterparts. Women in other age groups had less risk compared to the youngest age bracket. Divorced women had a more than two-fold increased risk of domestic violence compared to women who were single. Similarly, women who disclosed their serostatus to their husbands/partners had a more than two-fold increased risk of domestic violence compared to those that have not. Respondent's education had no significant effect on the occurrence of domestic violence. In contrast, the effect of husband/partner's education persisted after controlling for other determinants, where women whose husband/partner had non-formal education were at twice the risk of domestic violence compared to those with tertiary education. Religion was no longer a significant predictor of domestic violence after adjusting for the other confounders in the model. Discussion The prevalence of domestic violence observed among women living with HIV/AIDS in Kano (22%) was similar to the national figure reported among the general populace during the Nigeria Demographic and Health Survey (NDHS) (28%).12 It was however nearly double the figure (13.1%) for women in the north west zone of the country where Kano is located. Our findings were also similar to that reported among pregnant women in Zaria (28%)7 but much higher than that reported among the same group of women attending antenatal care in Jos (12.6%). 8 Furthermore, our prevalence is much lower than those reported from selected communities in eastern (78.8%)15 and western Nigeria (81%).11 In contrast, our finding was comparable with a report from South Africa (21.5%).15 The higher prevalence in our study population compared to the general populace from the same region could be due to the two fold increased risk women face when they disclosed their serostatus to their intimate partners. This has also been reported previously.21, 22 The much higher figures reported in studies from other parts of Nigeria may be due to socio-cultural differences as demonstrated by much higher figures for South South Nigeria (52.1%) during the NDHS. Selection factors and differences in methodology could also explain some of the variations. The absence of sexual violence among our respondents could be due to underreporting or may be due to fear of acquiring the infection through sexual route. The high proportion of married women in the sample and cultural factors may play a role here. The low proportion of women seeking treatment and counseling after episodes of domestic violence was similar to observations made by others.19 It was also similar to the findings among abused women in south west Nigeria.11 This may be due to lack of confidential counseling and treatment services for victims. This underscores the importance of providing skilled counselors and confidential treatment and support for victims. The negative consequences of abuse are known to extend beyond a woman's physical health; it affects her psychologically and may affect the welfare of her children.20 This underscores the importance of protecting these women and provision of confidential counseling and treatment services. The increased risk of violence following disclosure of HIV serostatus among women in this study has been earlier reported.21, 22 This is by no means a uniform experience as some women indicated a supportive attitude from their spouses and family following diagnosis. Our findings were similar to several other reports where majority of women who disclosed their status reported supportive reactions.22-24 The proportion of women indicating negative reactions from their partners in the present study was higher than the proportions reported in studies conducted in other African countries (10-25%).25-27 With this outcome, women are likely to be discouraged from disclosing their serostatus to their spouses. This non-disclosure may delay the adoption of safe sex and other preventive practices that could protect the partners and other members of the family including the unborn baby. This is an important consideration in the development of policies and programs for curbing the AIDS epidemic. A major reason for non-disclosure is fear of partner's reaction.28, 29 This can be due to lack of adequate information or knowledge about HIV/AIDS, which include mode of transmission, prevention and avoidance of stigmatization. Interestingly, there has been a rising trend in disclosure rates among couples in Africa. For instance in Tanzania, rate of disclosure increased from 27% to 64% in 5 years. Our finding is similar to the later figure. Factors that may contribute to this change over time include increased awareness and acceptability of HIV and HIV testing in the community, better counseling surrounding disclosure, and more communication between couples about HIV and HIV testing.30 The present study identified respondent's age, marital status, disclosure and partner's education as predictors of domestic violence among women living with HIV/AIDS. This concurs with earlier reports where the most important predictors of violence with a current partner were HIV status, women's age, women's education, marital status, partner's age, partner's concurrent relationship with other women, and the age gap between partners.30 Based on the aforementioned reasons, it is clear that the epidemics of HIV and violence cannot be separated and that joint efforts are required from human rights groups and HIV/AIDS advocates for achieving the desired goal. Without gender mainstreaming and appropriate legislation, interventions targeting domestic violence may not be effective. It is also important to address poverty among women and provide them and their partners with basic education to improve understanding and communication. Policymakers and health program managers should implement appropriate counseling and support for women subjected to violence. Such programs are likely to succeed when they are holistic and interdisciplinary.30 Population-based intervention efforts are needed to reduce the level of HIV and violence against women. These efforts should include programs for gender tolerance and improved communication with rapid conflict resolution. They should aim to change the way violence against women is tolerated in societies and ensure adequate representation of both sexes in the decision-making process. This should transcend all levels including family, public and private domains and all age groups. In this and previous studies, partners' education correlated well with lower prevalence of domestic violence.17, 18 This could be explained by the fact that educated individuals are more likely to have correct knowledge of the disease thereby reducing misconceptions that could precipitate violence.18 Furthermore, additional population-based research is needed to identify the mechanism through which violence increases women's risk for HIV and vice versa. Women need to have improved access to HIV/AIDS prevention methods they can control. This could reduce the risk they face when negotiating safe sex practices with an uncooperative partner. The promising outcome of vaginal microbicides, female condoms and antiretroviral drugs are examples. Counselors need to be tactful regarding partner notification and client-referral is less likely to result in violence compared to health care provider-referral.25 Further research is needed to identify alternative counseling strategies that would minimize or eliminate post-disclosure violence altogether. The varied experiences of women that are HIV positive illustrates the challenges that HIV/AIDS treatment and care programs have to help their clients and their intimate partners understand their condition, to maintain relationships and safe sex practices to ensure that the negative partner remains uninfected.30 This study had several limitations. Firstly, our respondents were a selected group of HIV positive women receiving care from a large urban teaching hospital. Their characteristics are different from those seeking treatment elsewhere or rural HIV positive women most of whom may not be aware of their serostatus until they become symptomatic. This calls for caution in extrapolating our findings to the whole population of women living with HIV/AIDS in northern Nigeria. Apart from cultural variations across the region which may explain some of the baseline occurrence of domestic violence before the superimposed effects of HIV diagnosis, events of violence in families before the respondent disclosed status to partner may also account for the occurrence of violence. Our study instrument was not designed to capture these making it harder to draw precise conclusions about the relation between disclosure and violence. Subsequent studies should elicit the occurrence of domestic violence before HIV diagnosis; frequency of violence, most recent episode and interval between disclosure and violence. Secondly, some women may not divulge private information such as domestic violence to interviewers. This could lead to underestimation of the burden of domestic violence. It is these same factors that prevent women from reporting such violence to law enforcement agents who may consider such cases as private domestic matters not worthy of prosecution. Finally, the lack of mention of sexual violence may also be due to underreporting for the same reason earlier alluded to. However, the provision of HIV/AIDS treatment and care at no cost to clients could reduce the selection bias and the use of female interviewers, assurance of confidentiality may have reduced the effects of these limitations on the outcome of our study. In conclusion, the high prevalence of domestic violence among HIV positive women in this study calls for concerted efforts at combating underlying factors predisposing to violence among this vulnerable group of women. The combined effects of socio-cultural factors, disadvantages early in life and limited opportunities compounds the situation of HIV positive women in northern Nigeria. Addressing the root causes of women's low status and HIV risk, namely, gender discrimination, poverty, limited economic and educational opportunity, lack of legal and human rights protections are essential for success. Both government and non-governmental organizations should make and implement policies, programs and services to effectively address the overlap between HIV/AIDS and violence against women; there is need for an increased allocation of financial and human resources by governments, donors, multilateral institutions and civil society in addressing the vexing issue of violence against women as part of the overall response to HIV/AIDS; Provide a legal framework in order to address, prevent and combat violence against women more effectively; Construct mutual responsibilities among groups involved in women's rights, sexual and reproductive rights, human rights and groups of people living with HIV/AIDS. There is also the need to conduct community based studies and include culturally acceptable questions that will be incorporated in national surveys such as the demographic and health survey to get the real picture. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11034t2.jpg] [rh11034t3.jpg] [rh11034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}