 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
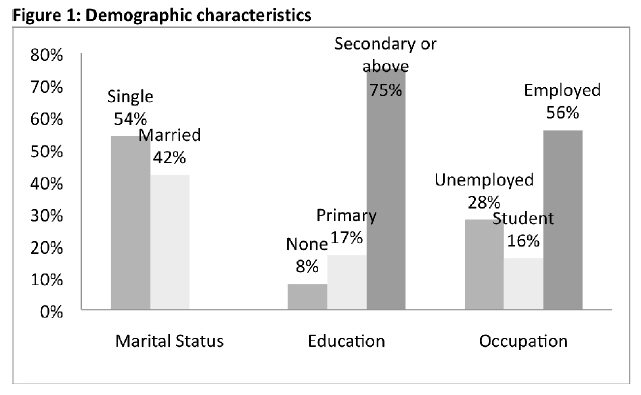
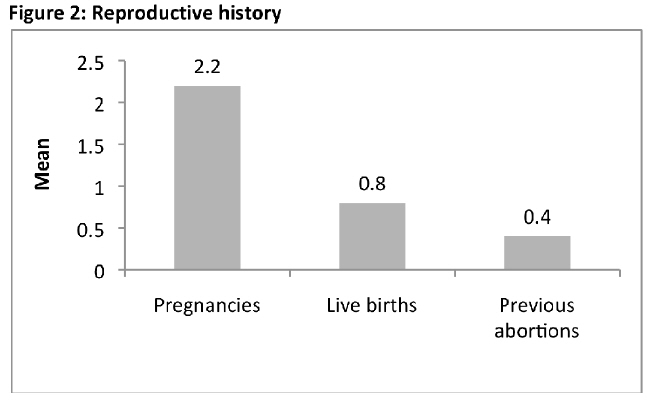
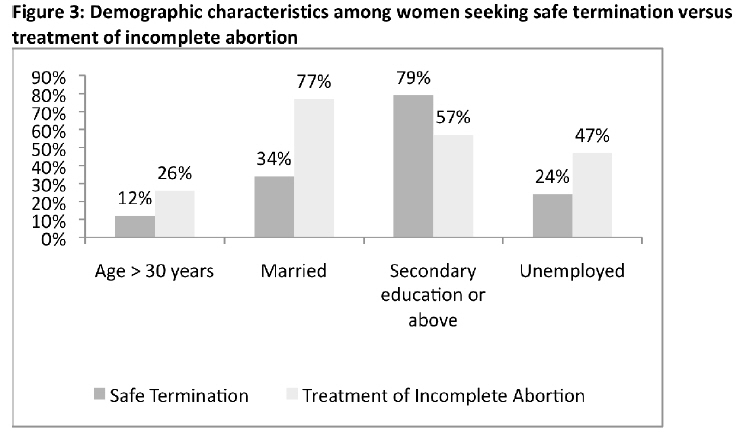
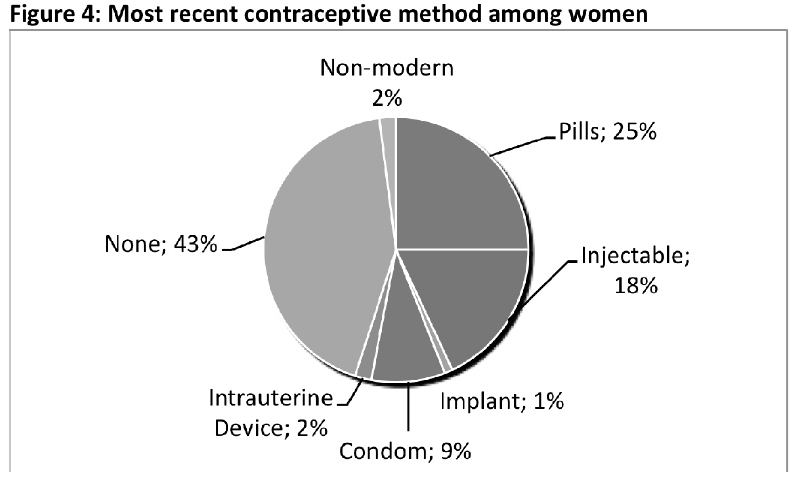
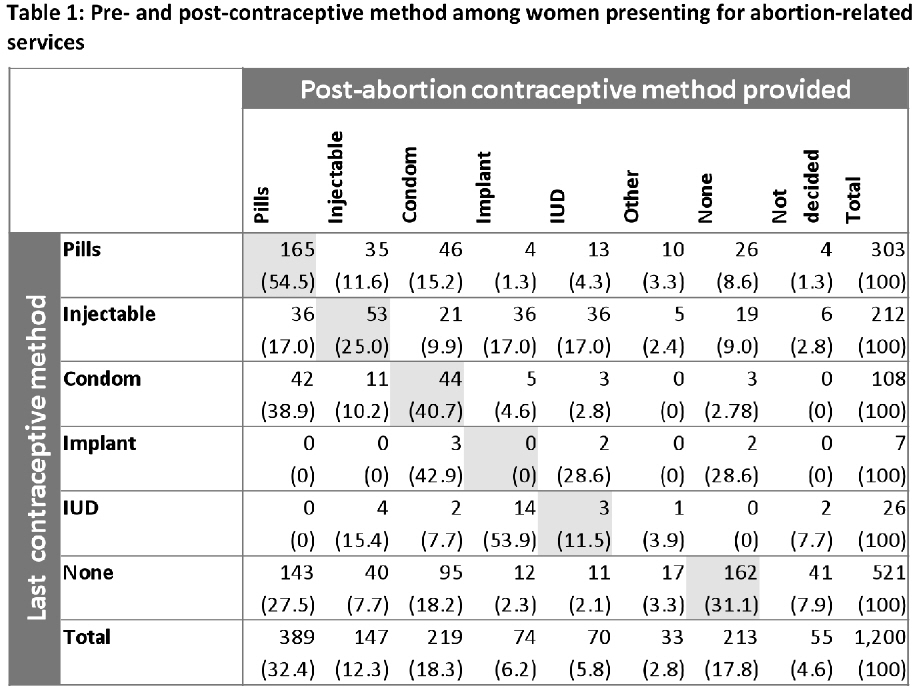
African Journal of Reproductive Health, Vol. 15, No. 3, Sept, 2011, pp. 55-62 ORIGINAL RESEARCH ARTICLES Factors Associated with Choice of Post-Abortion Contraception in Addis Ababa, Ethiopia Ndola Prata1 , Suzanne Bell1 , Martine Holston2 , Caitlin Gerdts1 , Yilma Melkamu3 1 Bixby Center for Population, Health, and Sustainability, University of California, Berkeley, USA Code Number: rh11035 Abstract The high demand for abortion related services in Addis Ababa, Ethiopia indicates a reliance on abortion to control fertility and highlights an opportunity to increase access to contraceptives and improve post-abortion care. We analyzed the medical records of 1,200 women seeking abortion related services. Logistic regression was used to determine factors associated with use of modern or long-acting contraceptive post-abortion. Multivariate results illustrate that women aged 40-44, students, employed women, receipt of services in private clinics, number of children, and number of previous abortions were significantly associated with the odds of adopting any modern contraceptive post-abortion. The odds of choosing a long-active contraceptive method were significantly and positively associated with being age 25-29, attaining secondary or higher education, and number of children. Improved services and information along with reliable access to modern and long-acting contraceptives can reduce the need to use abortion to control fertility among women in Addis. (Afr J Reprod Health 2011; 15[3]: 55-62). Résumé La demande augmentée des services relatifs à l'avortement à Addis Abéba, Ethiopie, montre une indépendance de l'avortement pour contrôler la fertilité et souligne une opportunité pour augmenter l'accès aux contraceptifs et améliorer les soins du post-avortement. Nous avons analysé les dossiers des 1200 femmes qui recherchaient des services liés à l'avortement. Nous nous sommes servis de la régression logistique pour déterminer les facteurs liés à l'utilisation du contraceptif du post-avortement modern ou à action prolongée. Des résultats ont montré que les femmes âgées de 40-44 ans, les étudiantes, les femmes employées, fréquentation des cliniques privées pour les services, nombre d'enfants et nombre d'avortements antérieurs, ont été significativement liés à la possibilité d'adopter n'importe quel contraceptif du post-abortion modern. La possibilité de choisir une méthode contraceptive à action prolongée a été considérablement et positivement liée au fait d'avoir 25-29 ans, ayant acquis l'éducation du niveau secondaire ou tertiaire et le nombre d'enfants. L'on peut réduire le besoin de contrôler la fertilité chez les femmes à Addis si les services et l'information ainsi que l'accès fiable aux contraceptifs modernes et à action prolongée sont améliorés. Key words: abortion, repeat abortion, post-abortion contraception, Ethiopia Introduction Ethiopia has one of the highest maternal mortality rates in the world. Approximately 590 women die due to pregnancy or pregnancy related causes per 100,000 live births1 , and more than half of these deaths are abortion-related . 2Following the revision of the criminal code in 2005 and the development of abortion series guidelines by the Ministry of Health, access to safe abortion has been gradually increasing. Unfortunately, services are not yet widely available throughout Ethiopia. Country-wide, the total fertility rate (TFR) in Ethiopia is still very high (5.4)3 , close to one third of births are either mistimed or unwanted, and there is a 34% unmet need for family planning3 . However, the capital city, Addis Ababa, has experienced rapid fertility decline and achieved below-replacement fertility (TFR 1.4)3 . In addition, one-third of married women in Addis Ababa are using a modern method of contraception compared to only 6% country-wide. Despite these improvements, the estimated abortion rate for Addis Ababa in 2008 was 49 abortions per 1,000 women of reproductive age, which is more than twice the national rate of 23 abortions per 1,000 women of reproductive age . 4This reflects a high demand for abortion-related services and points to its role in the fertility decline in Addis Ababa. The high abortion rate also highlights a need for increasing access to modern family planning, especially long acting methods, and the strengthening of post-abortion contraceptive services. Post-abortion contraceptive use varies widely depending on the quality of the post-abortion family planning and counseling services provided. High quality family planning counseling within post-abortion care (PAC) has been demonstrated to be effective in improving post-abortion contraceptive adoption5-9. Of particular interest is the proportion of clients who adopt long-acting methods of contraception, which have been shown to significantly reduce rates of unintended pregnancies and repeat abortion10-14. Adoption of any modern method is also important because although not as effective as long-acting methods, they are better at preventing unwanted pregnancies than non-modern methods or no method. Although abortion in Addis is safe, repeat abortion is still associated with negative subsequent health consequences (e.g. increased risk of subsequent placenta previa, ectopic pregnancy, preterm birth, and possibly subfertility and breast cancer), thus increasing modern and long-acting contraceptive utilization is optimal15. Studies investigating post-abortion contraception practices demonstrate that method adoption varies widely depending on individual demographics and context7,16-19 . In general, a larger proportion of women seeking safe abortion or post-abortion care in Africa are unmarried compared to Asia, where the majority of women tend to be married19. The purpose of this paper is to examine factors associated with choice of contraceptive, in particular modern and long-acting methods, after an abortion in Addis Ababa, Ethiopia. Methods We analyzed the medical service records of 1,200 women seeking abortion related services using data collected prospectively from October 2008 to February 2009 in four public and three private health facilities in Addis Ababa. This data was collected as part of an assessment of the characteristics of abortion seekers in Addis Ababa. Of the 1,200 patients, 82% were seen in private facilities. Ethical review for the study was provided by the Committee for the Protection of Human Subjects at the University of California, Berkeley (#2008-9-56). As part of the confidentiality agreement we made with participating facilities, we are not allowed to disclose the facility names. We assured participating facilities that the data would not be analyzed specifically by facility and that this information would not be disclosed. All data collected was extracted from patient records using a form prepared by the investigators. Informed consent to use the data without patient identifiers was requested by the provider prior to service provision. Investigators did not have direct contact with patients. However, researchers trained the providers to correctly gather the information requested in the forms, and reviewed the charts on an ongoing basis to ensure completeness of forms and data accuracy. Socio-demographic characteristics, reproductive history, type of service provided (treatment of incomplete abortion or pregnancy termination), and contraceptive history data were extracted from client records and assessed in this analysis. We examined last contraceptive method used and method of contraceptive adopted after the abortion service was provided. Univariate and bivariate analyses were conducted to determine the demographic characteristics of women seeking abortion services and their post-abortion contraception preferences. Logistic regression analysis was used to assess factors associated with choice of any modern or long-acting method of contraception post-abortion. For the purpose of this analysis, women were considered to be long-acting method adopters if they left the facility with one of the following methods of contraception: injectables, implants, or IUDs. To assess factors associated with the choice of a long-acting contraceptive method among women with history of contraceptive use, we stratified the multivariate analysis according to previous use of any contraceptive method, resulting in two groups of women, those who have ever used and those who have never used contraception. Results Examination of the socio -demographic characteristics revealed that overall, most of the 1,200 women seeking abortion-related care during the study period were young, well educated, and single (Figure 1). The mean age of women requesting services was 25, and 79% of women were ages 20 to 29; fewer than 5% of women were under 18 or over 36. Women were fairly well educated, with 75% of women having completed secondary education or above. As expected from previous research conducted in Africa, more women were single (52%) than married (44%). While women had an average of 2.2 pregnancies, the average number of live births was 0.8, indicating the role of abortion in fertility control (Figure 2). One-third of women had had a previous abortion (not shown), and the mean number of abortions among women who had had at least one previous abortion was 2.3 (not shown), including the abortion sought at the time of the study. Over half of the women had ever used family planning, and previous contraceptive utilization was lower among the younger women (not shown). Those who reported ever use had used contraceptive methods inconsistently. More women came to the health facilities seeking safe abortion (82%) than post-abortion care (18%), and almost all safe abortions occurred within the first trimester (96%) (not shown). Women seeking treatment for incomplete abortion were more likely to be older (26 vs. 25), married (77% vs. 34%), and less educated (57% reaching secondary or above vs. 79%) compared to women seeking safe abortion (Figure 3). Among the women presenting for abortion services, 363 (30%) sought a repeat abortion, which we defined as having more than one induced abortion (not shown). Only 57% were using a contraceptive method immediately prior to presenting for abortion-related services, 55% of which were a modern method. Of those using contraception, the majority were pill users (Figure 4). During post-abortion services, 86% of women adopted some method of contraception. The methods most commonly adopted were pills, injectables, and condoms. Table 1 details the last contraceptive method used prior to the index pregnancy for which abortion-related services were sought and the method women received post-abortion. Thirty-six percent of women left the facility after receiving abortion-related services with the same contraceptive method they had previously been using. Specifically, 55% of women who had previously been using pills left with pills, 25% of women who had previously been using injectables left with injectables, 41% of women who had previously been using condoms left with condoms, 12% of women who had previously been using implants left with implants, and 31% of women using no method continued to use no method. Multivariate analysis shows that being age 40-44 (OR=0.12, p=0.02), being a student or being employed (OR=2.45, p<0.01 and OR=1.55, p=0.02, respectively), receiving abortion services in a private clinic (OR=2.34, p=0.01), number of living children (OR=1.55, p<0.01), and number of previous abortions (OR=1.46, p=0.03) were all statistically significantly associated with the odds of adopting any modern method of contraception after abortion (not shown). Younger age groups, marital status, and education level were not statistically significantly associated with the odds of leaving the post-abortion care services with a modern family planning method. Among all women, the odds of adoption of a long-acting contraceptive method was significantly and positively associated with being age 25-29 (OR=3.03, p=0.03), having a level of education of secondary or higher (OR=2.82, p<0.01 and OR=2.26, p=0.03, respectively), and number of children (OR=2.14, p<0.01) (not shown). However, adoption of long acting contraception post-abortion was negatively associated with being unmarried (i.e. single, widowed, or divorced) (OR=0.46, p<0.01) and not having had a previous abortion (OR=0.66, p=0.02). When stratified by ever previous-use of contraceptives, among women that had never used contraceptives, those who lived outside Addis Ababa or abroad (OR=4.46, p<0.01 and OR=7.03, p=0.04, respectively) and those who had more children (OR=2.32, p<0.01) had significantly increased odds of adopting a long-acting method (not shown). In contrast, older women (40-44) (OR=0.03, p=0.04) and women using a private clinic (OR=0.16, p<0.01) had significantly reduced odds of adopting long acting methods (not shown). Factors associated with long-acting method adoption post-abortion among women with previous contraceptive experience differed significantly from those who had never used contraceptives. Among previous users of family planning, women who were educated (secondary or above) (OR=3.26, p=0.01 and OR=3.02, p=0.02, respectively) had significantly increased odds of adopting a long-acting post-abortion method, whereas not being married (OR=0.55, p=0.01) and having had a previous abortion (OR=0.55, p<0.01) were associated with decreased odds. Number of children (OR=2.07, p<0.01) was associated with increased odds of long acting method adoption among previous users, which was the only factor also significantly associated with long-acting method adoption among never users of family planning. Discussion Among all women surveyed, being a student, receiving services in a private clinic, ever having a previous abortion, and higher parity were all significantly associated with increased odds of adopting modern methods of family planning. More education was associated with increased odds of adopting long-acting methods (i.e. injectables, implants, and IUDs), while being unmarried, receiving services in a private institution and ever having had a previous abortion was associated with decreased odds of uptake. Among never-users of contraception, living outside of Addis and higher parity was associated with higher odds of uptake of long-acting methods, while older age and receiving services in a private institution were associated with lower odds of such uptake. Furthermore, among ever-users, being between the ages of 25-35, having higher than secondary education, and higher parity were associated with greater odds of uptake of long-acting methods of contraception, while receiving services in a private clinic and ever having had an abortion were associated with lower odds of uptake. This study's largest strength lies in the number of women for whom data was collected and the associated power to detect significant differences and trends among this group of women. Additionally, we had a wealth of data about each woman, which allowed us to investigate myriad relationships, to control for previously established confounders, and to stratify on important factors. Despite these strengths, the study did have limitations. Women were not followed prospectively once they received their method post-abortion, so we do not know the patterns of use or continuation. In addition, the data do not indicate the methods available to each woman at their respective facility, the PAC practices, and whether the method they reported adopting was chosen or simply prescribed. Thus method adoption could be a factor of method availability and provider bias, not simply women's preferences. The fact that many of the women (36%) adopted the same method post-abortion that they had been using previously indicates a missed opportunity to better meet women's contraceptive needs through family planning counseling. If a woman presents for abortion-related services and was currently using contraception, clinicians need to investigate why the method did not work for that woman and propose other, better-suited methods. Raising awareness of long-acting methods among both clinicians and patients through information and education campaigns can improve uptake of these methods, which have been demonstrated to reduce unintended pregnancies and repeat abortions. Results also present interesting insight into the private sector in Addis Ababa, Ethiopia. The odds of receiving modern contraception post-abortion was significantly higher in the private sector (2.3) compared to the public sector, but odds of receiving long-acting contraception were much lower in the private sector (0.4). This perhaps indicates provider bias against long-acting contraception due to lack of provider training, lack of method availability, the potential for decreased revenue in the future, and/or an unwillingness to talk to women about the full range of family planning options and their preferences. Further investigation of this finding should be conducted. Women in Addis Ababa require access to a full range of contraceptive methods, accurate information on family planning, and availability of effective 11. contraceptive methods and safe abortion services. Improved services and information along with reliable access to modern and long-acting contraception has the potential to reduce unwanted 12. pregnancies and the need to use abortion to control fertility among women in Addis Ababa, Ethiopia. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11035f4.jpg] [rh11035f3.jpg] [rh11035t1.jpg] [rh11035f1.jpg] [rh11035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}