 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
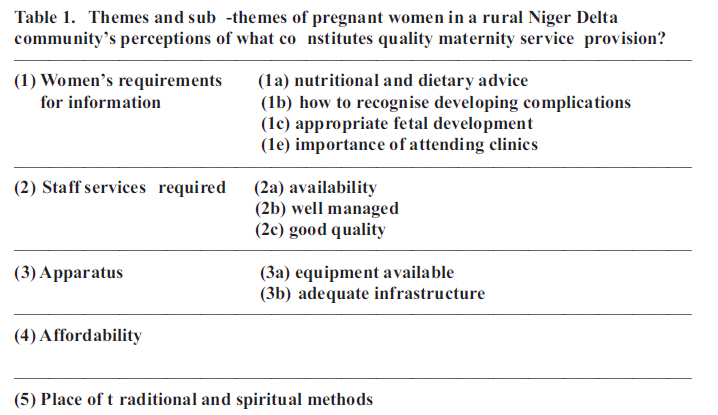
African Journal of Reproductive Health, Vol. 15, No. 3, Sept, 2011, pp. 63-77 ORIGINAL RESEARCH ARTICLES What are pregnant women in a rural Niger Delta community's perceptions of conventional maternity service provision? An exploratory qualitative study George Mnaemeka Igboanugo1, Caroline Hollins Martin2 1 General Practitioner, Casia Medical Services 15 Kigoma Street, Wuse, Zone 7, Abuja, Nigeria & School of Health, Glasgow Caledonian University, UK . Code Number: rh11036 Abstract At present there is under utilization of maternity service provision in Nigeria, with only a third of childbearing women electing to deliver in healthcare facilities. This is relevant since Nigeria's maternal mortality rate is second highest in the world and is estimated at 1,100 per 100,000 live births. To date, studies have sought cause and effect and have neglected the opinion of the people about what they perceive to be problematic and what they believe constitutes satisfactory maternity service provision. An exploratory qualitative study was carried out to identify pregnant women in a rural Niger Delta community's perceptions of conventional maternity service provision. Participants included 8 pregnant Niger Delta women from differing sub-groups within the homogeneous population. Semi-structured interviews were conducted to explore informants' views of what constitutes satisfactory maternity service provision, what comprises inadequate care, barriers that obstruct delivery of maternity care, and what promotes positive outcomes. Five major themes emerged from the data. These included: (1) Women's requirements for information; (1a) nutritional and dietary advice, (1b) how to recognise developing complications, (1c) appropriate fetal development, (1e) importance of attending clinics; (2) Staff services required: (2a) availability, (2b) well managed, and (2c) good quality; (3) Apparatus: (3a) equipment available, (3b) adequate infrastructure; (4) Affordability; (5) Place of traditional and spiritual methods. The interviewed childbearing Niger Delta women voiced several factors that they considered altered their satisfaction with maternity service provision. Finding out more about what causes satisfaction/dissatisfaction in childbearing women facilitates maternity care professionals to improve standards of care and allocate resources more effectively. Policy changes are driven by initiatives that reinforce strengths of current specification and recognise weaknesses. In addition, the WHO recommends that working towards improving health related culture is important. (Afr J Reprod Health 2011; 15[3]: 63-77). Résumé Al'heure actuelle, il y a une sous utilisation de services de gynécologie-obstétricaux au Nigeria, étant donné qu'un tiers des femmes en âge de procréer optent pour accoucher dans des établissements de santé. Les études antérieure ont recherché la cause et l'effet et ont négligé les opinions des femmes concernant ce qu'elles croient être la bonne prestation de services de gynécologie-obstétricaux. Nous avons mené une étude qualitative exploratrice pour identifier 8 femmes enceintes à partir des perceptions d'une communauté rurale du Niger Delta à l'égard de la prestation de services de gynécologie-obstétricaux conventionnels. Des interviews semi-structurés ont exploré les opinions des enquêtées sur ce qui constitue la prestation de services de gynécologie-obstétricaux satisfaisant, ce qui constitue les soins insuffisants, les obstacles qui entravent la prestation de soins de gynécologie-obstétricaux et ce qui avance les résultats positifs. Cinq thèmes importants ont émergé à partir des données : (i) Les besoins des femmes pour les renseignements ; 1a) le conseil nutritionnel et alimentaire, 1b) comment reconnaitre des complications qui se préparent, 1c) le développement approprié des fétus, 1e) la nécessité de fréquenter les cliniques, 2) bien gérer, 2c) la bonne qualité 3) appareil 3a) l'équipement disponible, 3b) l'infrastructure adéquate ; 4) s'ils sont abordables ; 5) la place des méthodes traditionnelles et spirituelles. Les femmes enquêtées ont mentionné plusieurs facteurs qui ont modifié leur satisfaction avec la prestation de service de gynécologie-obstétricaux. La recherche supplémentaire concernant les causes de la satisfaction ou du mécontentement rend facile la tâche des professionnels de soins de maternité leur permettant d'améliorer la qualité de soin et d'affecter des ressources plus efficacement. Key words: forced sex, Uganda, married, shame, sexual violence, HIV/AIDS Introduction According to recent estimations by the World Health Organisation,3 Nigeria's maternal mortality rate is second highest in the world (after India), and is estimated at 1,100 per 100,000 live births3,4. This equates to 54,000 Nigerian women dying each year from pregnancy related complications 5,6 , which represents 10% of global maternal deaths5,7. Due to poor documentation systems for registering births and deaths and for reporting cases of morbidity, these figures are approximations . 5 The aim of maternity service provision is to prevent mortality and morbidity1 , with success measured in terms of maternal and neonatal outcomes1,2. This process incorporates understanding of factors that influence and affect maternal health and is associated with utilization of proper facilities that improve maternal and neonatal health outcomes1 . Conventional maternal healthcare encompasses antenatal, intranatal and postnatal care, which incorporates physical examinations, early identification of high risk mothers, recognising danger signs to enable appropriate preventive action, screening measures and procedures that monitor pregnant woman from conception to 6 weeks post delivery1,5. The rationale underpinning this enquiry is the contemporary under utilization of maternity service provision in Nigeria, with only a third of childbearing women electing to deliver in healthcare facilities8-10. To date, studies have sought cause and effect and have neglected the opinion of the people about what they perceive to be problematic and what they believe constitutes satisfactory maternity service provision11 . To create further understandings, factors outside formal medical practice should be considered12. The rural population of Niger Delta accounts for 67–80% of Nigerians13 , with understandings of the people an essential component of designing, delivering and evaluating maternity service provision 14 . Underscored by this rationale, the research question asked; what are pregnant women in a rural Niger Delta community's perceptions of conventional maternity service provision? The objectives were to determine what pregnant women from the Niger Delta region understandings of what constitutes satisfactory maternity service provision, what comprises inadequate care, barriers that obstruct delivery of maternity care, and what promotes positive outcomes. This research intends to obtain more in depth knowledge on maternal health care based on perceptions from the focal subjects, pregnant women in the Niger Delta region. Findings may hopefully give better understanding on how to approach the more sensitive issues in maternal health care and pregnancy outcomes. Methods An exploratory qualitative study was conducted to obtain perceptions of pregnant Niger Delta women of conventional maternity service provision 15. This research focuses on answering a broadly stated question about individual viewpoints, which unlike deductive quantitative reasoning may generate many answers16. Developed conceptualizations will arise from actual narratives of the participants17. The exploratory nature of the method permits the researcher to focus more precisely on informant's concerns18. The approach utilises a naturalistic inquiry, with focus on perception rather than experience19. The importance of the qualitative method is to give voice to pregnant women, without manipulation or forced influence about a matter that directly concerns their welfare. Verbal expression of this description is fixed in text, where the meaning intended by the speaker can be located20. Ethical approval Ethical approval was obtained from Glasgow Caledonian University School of Health ethics committee (29 March 2010. Re: PMcQ/EI). Permission was also granted by the community leader and informant's doctor. Participant selection Within a qualitative method, sample size depends greatly on the testimonies of the individuals involved and the richness of the data 21. This means the number of research participants can be very low. Per se, the approach utilizes small sample sizes and acknowledges the limitation that findings cannot acceptably be generalized to the larger population21, 22 . The research aim required that an in-depth approach was adopted. A decision was therefore taken to limit the number of informants, with a view to undertaking greater depth of enquiry. Non probability random purposive sampling covered assorted sub-groups within the homogenous population16 , which increased the scope of the data obtained and enhanced the possibility of uncovering multiple realities 14 . Sampling criteria included age, parity, gestation, frequent use of maternal health services and being in a current state of sound health. Eight participants were considered an adequate sample size, since data was rich and had enough dimensions to answer the research question. The community leader distributed an information sheet and consent form to 38 pregnant women. From this number, 18 volunteers were divided into 3 groups based on age, parity and gestational age. Two participants were selected because of frequent usage of maternity service provision. The remaining 6 picked small pieces of paper bearing 'selected' out of a basin. The nominated women selected the location and date for their interview. The 8 volunteers were pregnant women who resided in the Niger Delta community, who had recently accessed maternity service provision. Included were 3 women in the first trimester of pregnancy, 3 in the second, and 2 in the third. Age range was 24-35 years; 2 were primigravidas and 6 multigravidas; 1 woman was in her second pregnancy, 4 in their third, and 1 in their fifth. All spoke English as their first language. Written consent was obtained and audio recordings were made available. Informants were afforded anonymity and confidentiality, and assured that nonparticipation would have no affect on their subsequent maternity service provision. Interviews Prior to interview the scope of maternal healthcare was defined. Six private semi-structured interviews were conducted within the participant's home and 2 in the health centre. Interviews explored informants' perceptions of: (1) what constitutes satisfactory maternity service provision, (2) what comprises inadequate care, (3) barriers that obstruct delivery of maternity care and (4) what promotes positive outcomes. The interviews were conducted face-to-face in a local health centre and were taped using a digital recorder. Procedures were informal and amorphous to permit greatest flow of information. In an unstructured format, the diverse untailored perceptions of pregnant Niger Delta women were unravelled 23. Questions were asked and prompts given. For example: Can you provide an example? How would you go about this? Could you elaborate on that? Participants could make as many (or as few) comments as they liked. The flexibility of unstructured interviews permitted the researcher to follow the lead of the interviewee, to reveal emergent themes and gain insights24. Processes were designed to enable the researcher to revisit the raw data time and again25. Data analysis Interviews were transcribed verbatim 26. All transcripts were read in entirety to assist engagement and generate interpretation from an initial sense of informants' stories. The rationale was to identify preliminary codes. The coding procedure was based on that developed by Charmaz27 , who suggests open coding line by line, which although rigorous helps to reduce researcher influence and bias. Short descriptive labels were allocated to sections of the text, following which labels expressing similar concepts were grouped together to form themes. Labels and themes were compared across scripts. The allocated codes enabled the researcher to summarise and synthesise the data. During the writing process, literature was used to support the allotted labels and their properties. The selected quotes reflect themes that unravel the unaffected perceptions of the interviewed pregnant Niger Delta women about what they perceive constitutes satisfactory maternity service provision19,21. Trustworthiness To establish trustworthiness of the study, three issues are considered important; credibility, transferability and dependability 28 . Inter-rater reliability was confirmed by the two researchers carrying out the data analysis to reduce the potential for researcher bias during theme development. The final category system produced was agreed by both researchers and accepted as being representative of the data. All data collected remained confidential and anonymity was imposed at the point of transcription. Researcher impartiality was clarified from outset, with biases or assumptions that may impact on inquiry established29. Findings and discussion Five major themes emerged from the data. Themes and sub-themes are outlined in Table 1: Findings are not intended to be representative or generaliseable. Due to their subjective nature, the aim is to make more explicit and open up for analysis areas of women's thinking about what they believe constitutes satisfactory maternity service provision. Findings and discussions are as follows: (1) Women's requirements for information The theme women's requirements for information consists of 4 sub-themes and is concerned with an expressed need for knowledge that would improve the informants' pregnancy outcomes. The 4 sub-themes included: (1a) Nutritional and dietary advice Three participants perceived that receiving nutritional information was an important aspect of maternity service provision. There was strong belief that a balanced diet led to successful outcomes, in keeping with the findings of Shah and Ohlsson:30 “There are a lot of nutrients that I have to give to the baby inside me, and most time they are not known. The only way for it to be made known for the mother, is if she goes for antenatal care and classes” (P7). “I feel antenatal is good because it helps for a first timer like me, because it helps me to know what to eat” (P4). The importance of diet was connected to various health and welfare issues: “Antenatal helps me to in my own way not to, you know over eat for the sake of the baby and my own sake, so that the delivery will be easier” (P4). Emphasis was placed on being provided with appropriate nutritional information by experts: “...and other people as well like the dieticians and nutritionists. Health professionals need to put hand on deck to make pregnant women deliver safely” (P1). Informants were correct in their assumptions, since evidence has shown that Multiple Micronutrient (MMN) deficiencies hamper fetal growth30,31 . Intrauterine Growth Retardation (IUGR) due to suboptimal maternal nutrition is considered to be the main cause of Low Birth Weight (LBW) infants in developing countries32. LBW infants (LBW = birth weight < 2500g) are at greater risk of neonatal mortality and morbidity33 and all its associated adverse health outcomes in adulthood34,35. LBW babies can develop suboptimal cognitive capacity36 and often present with behavioral problems during infancy and childhood36,37. (1b) How to recognise developing complications Health education may be deemed successful if it makes an impact on women's health seeking behaviours. Unless women's general health status is improved, and special attention is paid to their reproductive health problems, success in preventing negative pregnancy outcomes is limited. As long as women are powerless to actively participate in self-care, their health status cannot be improved. Six participants perceived that providing information about physical adaptations during pregnancy would improve pregnancy outcomes: “To explain what's going on in my body to me is the most important, and to advise me on the things to do and the things not to do. I think that is the most important thing” (P6). “To know what, at every point, at every stage of the pregnancy I know what I am to do” (P4). Knowing what to do was perceived by Participant 4 to be an important component of priming for delivery: “...to know how to prepare towards my delivery date and all that” (P4). The following participants perceived that being able to recognise deviations from normal was crucial: “They should teach you about things that may go wrong. So you guard against it, and they teach you signs okay that something is already wrong so you should see your doctor” (P1). “...and they should teach safe methods. Methods you can use to safeguard yourself in pregnancy” (P2). Participant 7 perceived that providing knowledge should not only be restricted to primigravidas: “This is my third pregnancy, but I am still learning new things in the antenatal classes” (P7). Participant 5 expressed that timing of information was salient: “They should just try to understand us and explain to us stage by stage” (P5). Providing information about signs of jeopardy enable a person to identify problems and seek help5 . An example of this is providing information on how to recognise “high blood pressure” or developing “pre-eclampsia”. Providing accurate information may help dispel the myriad of hazardous superstitions and false information handed down to women by relatives, spiritualists and traditional birth attendants38. (1c) Appropriate fetal development The 12-hour daily fetal movement count is a generally applicable method of monitoring fetal welfare during pregnancy and provides an inexpensive adjunct or even an alternative to more expensive placental function tests. Four participants attached importance to receiving education about how to recognise fetal well-being: “With antenatal you know, how your baby is faring...The way my baby is growing inside me” (P4). The following participants saw need for information that would help preserve fetal safety: “Another thing is when it comes to the provision of the baby, most mothers don't know” (P1). “They even teach you positions that will not affect you or the baby” (P2). Fitting fetal medicine in any given circumstance in developing countries requires an integrated and holistic program of interventions at various levels. Interventions must not only include health-related measures that have a direct bearing on neonatal outcomes, but several other ancillary measures of equal importance. Such measures may include improving opportunities for education and empowering women's capacity for decision-making. An appetite for knowledge about how to care for the neonate was expressed by the following participant: “Everything I learn about how to take care of my baby should be done in the antenatal classes” (P3). The relationship between maternal education and neonatal mortality is complex, with several studies demonstrating reduced rates of infant mortality in association with increased levels of maternal education39-41. (1d) Importance of attending clinics Antenatal care is important because it helps to maintain the mother in good health during pregnancy, informs the parents about pregnancy, labour and child care and, in particular, it provides a means of detecting complications with the pregnancy at an early stage when the problems are treatable. Nonattendance at outpatient appointments is a challenge for maternity service providers. Patients with treatable morbidity may fail to receive care from which they would benefit, and scarce resources are wasted. Responsibility for poor attendance at clinics was ascribed to providers and recipients. Four participants expressed a need to advertise ante and postnatal services: “There is no format. There is no means of remembering for the patient. To continue like giving the patient pressure or reminding the patient on the need and importance of antenatal care” (P1). There is scope to increase attendance and reduce nonattendance at outpatient appointments, but initiatives should be piloted in conjunction with robust evaluative frameworks. Two participants perceived that health care professionals and the government should pressurize women to attend clinics: “It is difficult for mothers to remember to attend antenatal care, because there is not much force put on the mothers” (P2). “I expected such pressure or such test to be. That is to come from the hospitals. The healthcare professionals themselves” (P1). Telephone and postal reminders may be one effective method of reminding women, particularly if received within a day of scheduled appointments. Postal reminders offering a reward for attendance, threatening sanctions for non-attendance, and providing information about the clinic maybe more effective than standard reminders. There is also an expressed need for promoting understandings about why attendance at clinics is crucial: “Fine, they can actually give them orientation on why they need to go to antenatal and postnatal care” (P5). “When you are being told the importance of coming back for a checkup. I think it will help us, because a lot of women may not have the understanding and will say, I am okay, I don't feel anything” (P6). In contrast, Participant 5 perceived that accountability for clinic attendance lay with women: “I find the publicity and all that is still left to the women. It's still...They still have to make up their minds to go to hospital” (P5). Marketing of purpose and reminding women of imminent appointments may constitute strategies that work towards improving mortality and morbidity figures. What is clear, is that these interviewees understood that non attendance for antenatal care can elevate risk of adverse pregnancy outcome42. (2) Staff services required The theme staff services required consists of 3 sub-themes. Patient dissatisfaction with service provision has been shown to hinge on institutional factors, such as procedures available, staff attitudes and long waiting times 43. The 3 identified sub-themes included: (2a) Availability Shortages of health care professionals can affect the workload of existing staff and pose a potential threat to the continuity and safety of childbearing women. In chorus, it becomes impossible to meet targets aimed at reducing waiting for consultations and treatment. Six participants perceived that lack of staff decreased the standard of maternity service provision: “Although we have few doctors to cater for so many women” (P8). “Because right now they are lacking nurses and doctors. That's why when you come to the OPD (Out Patients Department), sometimes you stay for the whole day waiting to see a doctor, because they don't have many doctors. So you queue! There might be up to 200-300 patients waiting for one or two doctors” (P1). Participant 3 perceived that scarcity of qualified staff was worst in rural areas: “The health sector in the Niger Delta is so poor. When you come to our hospitals, there are no doctors or nurses. No medical professionals and when you even come to the rural community, it is worst” (P3). The content of postnatal care traditionally is to promote and monitor physical and psychological health of the mother, to ensure establishment of successful infant feeding, monitor various aspects of infant health and foster development of good maternal-infant relationships. Three participants perceived deficiencies with postnatal service provision: “Now for the postnatal care, I would say that part is nonexistent” (P3). “There is not much attention in that aspect. I didn't get any attention in that aspect. They only think about the baby and not the mother. But it is very important to postnatally care for me as well” (P8). “I am really, whether we have anything like postnatal care because… really no these days, I don't think we have anything like postnatal care” (P6). Although the following woman's postnatal provision was substandard to WHO44 recommendations, she counter argued: “Postnatal exists for me...Mine was actually adequate, but I found out that I was only asked to come back once for check up. So I felt there was going to be more” (P7). Participant 9 proffered a solution that would improve staffing levels: “Federal government should take it up. Whereby such training and education is being funded. So that the health sector will have enough doctors and nurses” (P9). To conclude, these six interviewees perceived that raising numbers and quality of skilled practitioners education would, among other factors, curtail mortality and morbidity statistics45. (2b) Well managed An organization that provides health care, either through the government machinery or through private health care apparatus is a working mix of private and public health care. People choose private health care typically because they can afford it and can exercise choice. The interminable queues for orthodox care and desire for enhanced opinion often make private care the natural choice. Typically consumers are “topping up” for a service that is faster and of a quality that suits them. In this vein, Participant5 perceived that private care was superior quality to orthodox maternity service provision: “But the way the government hospitals are being run. That's why people go to private hospitals” (P5). Attitudes, beliefs and motivation guided the following participant's behaviour along a specific path to a directed goal: “The only place I have an issue with, is the organization. Most times, like in my first pregnancy, when I went to the teaching hospital we had to get out files and jump queues, just so that the doctor will see us” (P7). Participant 7 understood that women who experience prenatal stress have higher rates of adverse outcome. Examples of these include LBW and pre-term delivery46,47: “So one doctor will consult, then he would leave and another one will come and leave. So it was really clumsy and the stress was too much for the mothers” (P7). Providing proficient care from the client's standpoint is fundamental to the provision of many services and is a laudatory step forward in maternity service provision. Participant 2 had clear expectations of efficiency from service providers: “But when you want to go for antenatal, you expect to be given instant care. So that you can go home and rest” (P2). Including the childbearing women's voice is an integral part of health service evaluation. Deriving data from a combination of health care professionals and consumer voices broadens the pool of feedback available. Participant 7 proffered a solution to enhance proficiency of clinics: “I suggest a system should be put in place whereby there are more doctors at different points, with different batches of pregnant mothers, for everybody to be attended to” (P7). Failure to identify emergency cases and delays in referral yield mortality and morbidity48-50. Employing health care workers with technical ability at the levels recommended by the WHO51 , may work towards improving customer satisfaction with maternity service provision. (2c) Good quality Good communication skills contribute to the quality of the health care professional; being compassionate, kind and supportive (affective domain), knowledgeable (cognitive domain) and skilful (psychomotor) are imperative. Five participants criticised personal attributes of some service providers. Participants 5 and 6 perceived that on occasion staff expressed antagonistic attitudes: “You know antenatal care these days. In this part of the country where we are, they don't treat women well they do. They bully you. They insult you” (P5). Inhospitable attitudes of staff create social and psychological barriers that limit willingness of consumers to attend for care43,48,50,51,52 . Poor staff attitudes can cause women to decline orthodox care and instead labour at home or in spiritual houses:50 “Starting from the fact that the staff in the hospital are not making things easy. They are not making it to be what antenatal care should be. In the sense that they don't really take good care of the pregnant women. Rather they feel they are doing you a favour by coming to the hospital or something. You know things like this make some people go to these spiritualists and all that making them to feel like the hospital is a home for demons, because of the character of the workers. From the cleaners to the nurses and sometimes the doctors” (P5). Substantially high caseloads can result in long working weeks, high stress levels and a feeling of insufficient support from the employing trust. The following participants perceived that large case-loads encroached on individual time allotted to the women: “That the doctors won't have time to attend to the patients as desired, because they will be rushing to see all the other antenatal patients. Thereby giving the patients limited time and they won't be able to get the facts and the problem of the patient” (P1). “I think doctors and matrons and nurses that organise these antenatal classes should be able to give more time to their patients, even though they have other things to give them. But I feel that is very important” (P6). For health care professional themselves, a self perception of providing suboptimal care can cause anxiety, with managing occupational stress a significant part of promoting employee well-being53 : “They are venting out their own frustrations on the pregnant women” (M5). The internet empowers users with healthcare information of unprecedented timeliness, accuracy, depth and diversity. Qualities that make the internet a rich marketplace of information also make it an exceptional channel for potential dissatisfaction when desired facilities are unavailable. Participant 5 articulated experience of having accessed the internet for information about test provision in the west: “But in advanced countries they can even check whether the baby is okay or not. But here they just check, maybe it's only the heartbeat they check and that is it, and they just assume everything is okay. So I think we have not gotten to that stage yet. Examinations and all those things, we don't do enough of it” (P6). Clinical audit is a quality improvement process that seeks to improve patient care and outcomes through systematic review of care measured against explicit criteria. Where indicated changes are implemented at an individual, team, or service level and further monitoring is used to confirm improvement in healthcare delivery. Processes involve establishing a working party to produce standards for maternity service provision. To facilitate implementation each standard sets out specific audit indicators. All audit indicators are collated to assist self-assessment and action planning. The process of audit is measured against these standards. Thresholds should be set locally to prioritise those areas identified as most in need of improvement. Where high standards are not achieved, data from audit may provide evidence to support a business case for additional resources. The following participant perceived that benchmarks of care provision in Niger Delta were insufficient: “When it comes to standards of delivery. It is poor (P1). Participant 1 articulated views that might contribute towards improving satisfaction with service provision: “I feel more training should be given to the ones we already have. That is the doctors and the nurses that we already have” (P1). Effective interpersonal communication between the health care provider and childbearing woman is an important element for improving consumer satisfaction, treatment compliance, and ultimately health outcomes. Women who understand the nature of their condition and its management are more likely to believe the provider is concerned about their wellbeing. Participant 6 placed emphasis on improving the quality of communication skills of personnel: “I think it is the duty of the matron or the doctor to bring that person out to be able to express herself, and be able to tell the doctor and the midwife what she is exactly experiencing, and address whatever that person is going through. Especially when it is a first timer” (P6). In stark contrast, participants 7 and 4 expressed satisfaction with conventional maternal service provision: “Actually I am 80% or let's say 90% satisfied with antenatal care, especially in teaching hospitals” (P7). “Yes I am satisfied. So far so good with what they are doing in the hospital I am using” (P4). In summary, five informants perceived a need for pleasant highly trained staff with reduced workloads. An increase in funding and university contracts to enlarge student numbers may contribute towards improving consumer satisfaction with conventional maternity service provision in Niger Delta. (3)Apparatus The theme apparatus included equipment available and adequate infrastructure of facilities. The 2 sub-themes included: (3a) Equipment available A well-trained and supported workforce is essential for achieving satisfactory maternity service provision. A health centre with skilled workers cannot prevent maternal or child deaths without an adequate supply of specialized equipment. This is true not only of health-related goals, but of those related to education, economic opportunity, human rights and environmental conservation as well. Healthy societies can expand economically and socially, and provide education and opportunities for their people. Four of the participants perceived that equipment was lacking: “They don't have equipment to check for scans. They don't have anything to check for protein levels” (P5). “...and the facilities there. Even the labour beds. Even the baths there. Even the machines. Even the equipment. They lack some of them” (P1). Again 2 participants had accessed information on the internet about maternity service provision in other countries. Information retrieved facilitated understandings of what sophisticated services could potentially be made available: “Well I think it can be better in our area and our own society, because when I go through the internet and go through the kind of tests and examinations. You know, the things they do. I begin to wonder, because we don't do half those things here” (P6). “I don't think we have the equipment here because of what you read on the internet that they do in other countries” (P3). In effect, providing essential equipment and teaching healthcare professionals how to use it with effect, may enhance satisfaction with maternity service provision in Nigeria5,49,54. (3b) Adequate infrastructure Well designed hospital environments can have a real impact on patient satisfaction and welfare; the size and scale of the hospital building, its layout, lighting and landscape, together impact on the experiences of childbearing woman. During and after delivery women require to rest in comfort and privacy in rooms equipped with essential amenities. Three participants perceived inadequacies in infrastructure of the buildings in which maternity care was delivered: “There was not enough space in the labour room...and when you come to the rural communities it is worst. They don't have the facilities” (P1). “...and also more consultation. More consulting rooms. In the teaching hospital there were only two consulting rooms. There was this particular instance when there were only two consulting rooms and about 4 doctors” (P7). “So I think more consulting clinics within the hospital” (P3). The role of paramedics in obstetric care is crucial. Ambulances equipped with a full range of emergency equipment can expedite transfer to hospital. Participant 1 acknowledged the worth of such provision: “There are no ambulance services. There is no eh. There is no number to call for the ambulance ha ha ha. There is no ambulance services” (P1). In addition, lack of obstetric skills, equipment and resources hamper staff from providing lifesaving emergency obstetric procedures55. (4)Affordability Niger Delta region of Nigeria is characterized by widespread absolute poverty, which ultimately will affect the capacity of many women to pay for transport to health centres and uptake of tests. To meet the WHO 56 recommendation of a minimum of 4 prenatal clinic visits , 5there is a requirement for service provision and willingness of the consumer to attend. Three participants voiced that cost deterred some childbearing women from accessing essential care, in keeping with the findings of Katung57 and Ogunniyi et al50 :“You know that most of these women. They run away from these hospitals because of costs” (P5). “Because it is not everybody that could have the money or have the guts. They are scared of private clinics because of the money you spend over there” (P8). “Because most things that scare mothers away from such care or such opportunity, is maybe the money involved” (P1). Participant 1 perceived that monetary issues inhibited women from accessing essential examinations: “When it comes to the money involved, most patients might not go for the tests, because they don't have the money” (P1). Participant 5 viewed that antenatal provision was a money making enterprise: “Some pregnant women, they claim that they (service providers) are actually using it to make money” (P5). In stark contrast, participants viewed that paying for tests and care directly improved service provision: “The private hospital is cleaner because we pay. We are paying for it. It's not a government hospital where you don't pay so much. So you are left with just what they offer you” (P4). Absenteeism from outpatient appointments is an intractable problem. Not only does it impact on patient outcomes, as a consequence of missed opportunities for diagnosis and treatment, it also reduces efficiency of health care systems. The following participants perceived that providing a free service would boost attendance at clinics and contribute to saving lives in Niger Delta: “Making such facilities free, so that mothers can be able to attend even when they don't have the money” (P1). “When all these facilities are free you find that such care will be used” (P2). Participant 5 viewed that spiritual care provided in healing homes was an inadequate alternative to conventional care: “I would, that em, if they can make it free, why not? If they could make it free. Maybe most of these women that go to healing homes might not go to healing homes” (P5). Providing gratis maternity care to Niger Delta residents would facilitate attendance at clinics and contribute towards improving mortality and morbidity statistics. At present, the only free provision in Niger Delta is through churches and healing homes50. (5) Place of traditional and spiritual methods Besides personal medication, there are three outlets from which healthcare are provided in Niger Delta. These include modern medical establishments, native doctors, and spiritual healing homes. The three coexist in rural and urban Nigeria. Even in the large urban areas where western science-based medicine is believed to dominate, other means of healing still proliferate and draw a large patronage. Three participants viewed that orthodox government provision was safer than native doctors and spiritual healing homes: “These healing homes and all that and all these places. They don't have that equipment to check for scans. They don't have anything. They don't know what to check for blood. They don't know what is in your urine. They don't know all these ones” (P5). Participant 6 also viewed that healing homes lack appropriate equipment and thrive on superstition: “They don't have any machines to check and they are only working by experience. People have different experiences and different kind of pregnancies and different situations. You can't say because this person is always throwing up in the morning it's going to be a boy” (P6). The act of healing in spiritual churches can take several forms. For instance, patients may be asked to fast and pray, or be fasted and prayed for by their kinfolk. After a period of fasting, the patient is given a bath in a basin of “holy water" with added perfume, powder, blood, oil or incense. The bath is accompanied by a chain of rituals and prayers. Two participants claimed that staff in healing homes lack professional training: “They are not medically qualified you know. So many people have lost their lives and their babies through this process” (P5). “My opinion is that well, with the churches for example, will still need an expert. I don't know how they can do it. But even in the native way or whatever you still need an expert” (P6). Participant 8 recognised that many of the treatments prescribed in spiritual healing homes did not address their problem: “They said I wasn't pregnant while I was pregnant. So the massaging and the way I was really massaged. If not for Gods intervention I would have lost the pregnancy. So I highly discourage it” (P8). Individual parishioner's perceptions are underpinned by beliefs built around the spiritual healing homes and the place of them in their life, what healing materials are used, and what rituals are pursued. Expectations may reduce anxiety and render the patients receptive and responsive to some aspects of treatment. Participant 5 perceived that a fusion of orthodox and spiritual provision would better serve some women's needs: “These women that go to these homes and churches. I don't think they are wrong, but if they can do it alongside with these medical people, maybe it will help” (P5). Factors which influence women's choice of agency for treatment include; their quest for spiritual/traditional explanation, extent of pathology, accessibility of suggested alternatives, the circumstances surrounding becoming ill and non-response to treatment received elsewhere. Reasons for consulting spiritual and native healers include supernatural or spiritual aetiology, scepticism of modern medicine, firm faith in “spiritual healers” or “native doctors”, and cost and convenience of facilities. Holistic conceptual paradigms that embrace psychological, physical and social needs can be gainful when they respect individual beliefs and culture58 . Such considerations are a valuable supplement to evidence-based maternity service provision. Discussion From the data presented it is clear that the pregnant Niger Delta women have a good understanding of what constitutes quality maternity service provision. The majority of the interviewees recognized the relationship of fetal wellbeing and health to maternal and neonatal outcomes5 . Their opinions indicate an awareness of factors that both enhance and impede quality of service provision. Interviewees appeal for more knowledge about how to recognize early signs of complications, with acknowledgement that quality antenatal care is important for good outcomes and safe delivery of babies. Providing antenatal education that encourages avoidance of harmful traditional practices and how to identify problems that require immediate professional attention would work towards improving maternal and neonatal outcomes51. The WHO advocates a need for information provision before birth and stresses that interventions alone cannot address the main causes of maternal mortality3 . The interviewees recognise that maternity care in Niger Delta is currently below WHO standards. A reluctance was expressed by some to attend for vital intranatal care. Reasons provided included overcrowded labour rooms and inhospitable midwives. Attitudes of staff towards pregnant women was cited as the main reason for avoiding orthodox maternity care43,48,50,51,52, with many women instead opting to deliver at home or in spiritual houses50. Poor staff/patient ratios were perceived to create long delays in treatment, thus escalating risks of morbidity and mortality48, 49, 50. Cost was also cited as a key factor in women's failure to attend for care. There was an expressed need for further visits and more attention from midwives and doctors. The interviewed Niger Delta women voiced several factors they considered altered their satisfaction with maternity service provision. In summary these include:
Healthcare cannot be high quality unless a person is satisfied with the care they receive. For this reason women's expectations and experiences of maternity service provision are salient. For the health care professional, consumer and researcher, satisfaction with service incorporates diverse meaning and content. For instance, being treated with respect, having one's comfort considered, being listened to, receiving a particular type of pain relief, coping well during labour, feeling in control, being well prepared, receiving minimal obstetric injuries and/or achieving the desired delivery style and outcome. Every woman constructs childbirth expectations differently and appreciation varies. Finding out more about what causes satisfaction and dissatisfaction helps maternity care professionals to improve maternity care standards and allocate resources more effectively. Conclusion With advocacy, technical help and funding, strategies could be implemented to bring orthodox maternity service provision in line with WHO recommendations which advocate that care include : 3
Irrevocably, making attendance for maternity care compulsory and free of charge would benefit both women and neonates. Health ministers dedicated to improving consumer satisfaction with maternity service provision require to hear the voices of the people they represent. This entails overcoming 10. barriers and taking advantage of opportunities that work towards improving the environment and consumer satisfaction. Policy changes are driven by initiatives that reinforce strengths of current specification and recognise weaknesses. In addition, the WHO recommends that working towards 11. improving health related culture is important56. Acknowledgements We thank the Niger Deltan women for accepting to participate in the study. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11036t1.jpg] |
| |||||||||

{kind=link}