 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 4, Dec, 2011, pp. 33-41 Original Research Article Socio-demographic and maternal factors in anaemia in pregnancy at booking in Kano, northern Nigeria Facteurs sociodémographiques et maternels de l’anémie chez les femmes enceintes lors de l’inscription à Kano, au nord du Nigéria Nwizu EN1, Iliyasu Z2, Ibrahim SA3 and Galadanci HS3 1Department of Obstetrics and
Gynaecology, Federal Medical Centre, Azare, Bauchi State, Nigeria; Departments
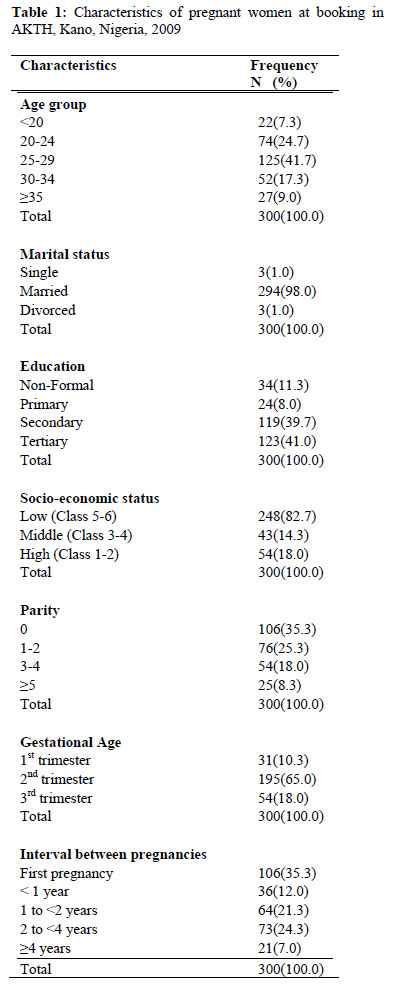
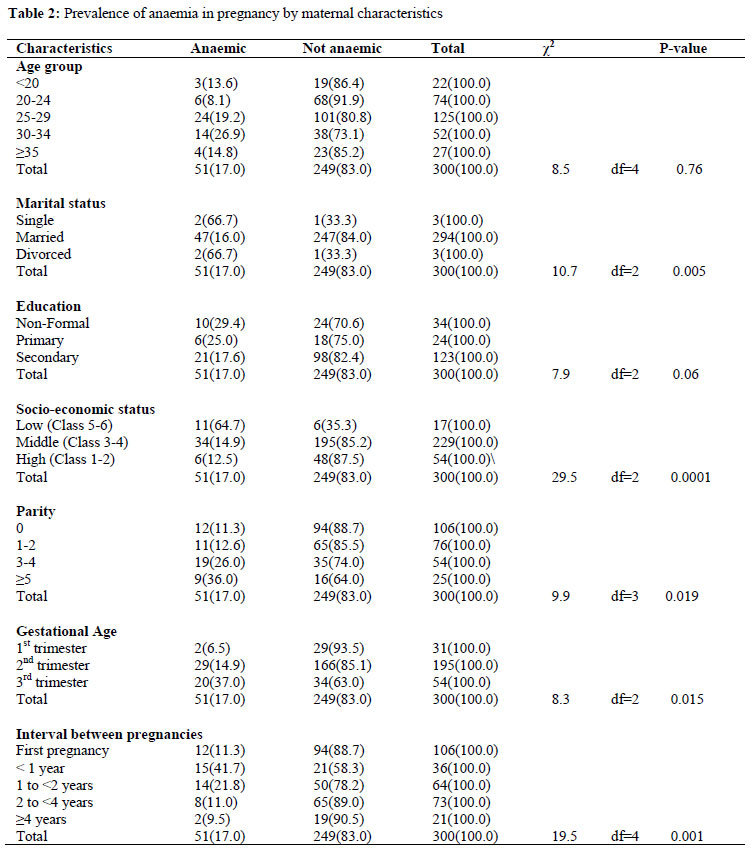
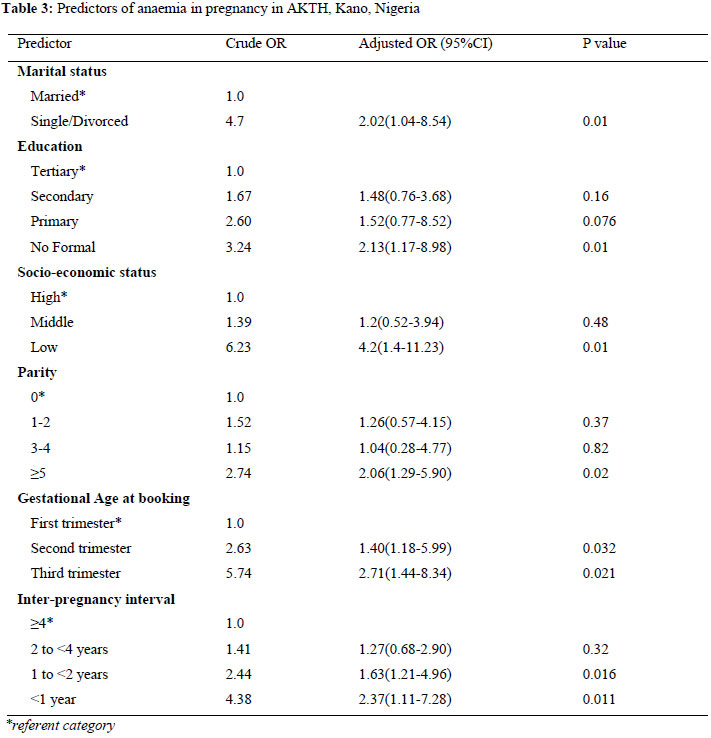
of Code Number: rh11048 Abstract Anaemia in pregnancy still causes significant maternal morbidity and mortality in the developing countries including Nigeria. The burden and underlying factors are varied even within countries. We studied the prevalence of anaemia at booking and underlying factors in a teaching hospital in northern Nigeria. Using the capillary technique and blood film, the packed cell volume (PCV) and red cell morphology of 300 pregnant women was determined. Additional information was obtained on socio-demographic characteristics, obstetric and past medical history using an interviewer administered questionnaire. Of the 300 pregnant women studied, 51 (17%) [95% Confidence Interval (CI)=12.9%-21.7%] were anaemic. Specifically, 12.7% and 4.3% of the women had mild and moderate anaemia respectively. Blood film of 74.5%, 15.7% and 11.8% anaemic women showed normochromic normocytic, haemolytic and microcytic hypochromic pictures respectively. Low educational attainment [Adjusted Odds Ratio (AOR)=2.13], being single or divorced [AOR=2.02], high parity [AOR=2.06], late booking [AOR=2.71] and short intervals between pregnancies [AOR=2.37] were significant predictors of anaemia in pregnancy. The high prevalence of anaemia in pregnancy related to low educational and economic status especially among women with background obstetric risk factors calls for vigilance, sustained health education and chemoprophylaxis for pregnant women (Afr J Reprod Health 2011; 15[4]: 33-41). Résumé L’anémie pendant la grossesse provoque toujours la morbidité et la mortalité significatives dans les pays en développement, y compris le Nigéria. Le fardeau et les facteurs sous—jacents sont variés même à l’intérieur des pays. Nous avons étudié la prévalence de l’anémie au moment de l’inscription et les facteurs sous-jacents dans un Centre Hospitalier Universitaire qui se trouve au nord du Nigéria. Nous avons déterminé le volume des hématies concentrés (VHC) et la morphologie du globule rouge chez 300 femmes enceintes à l’aide de la technique capillaire et des frottis de sang. Des informations supplémentaires ont été obtenues sur les caractéristiques ssocio-démographiques, les antécédents obstétriques et médicaux à l’aide d’un questionnaire administré par l’enquêteur. Sur les 300 femmes enquêtées, 51(17%) [95% Intervalle de Confiance (IC)= 12,9%-21,7%] étaient anémiques. En particulier, 12,7% et 4,3% des femmes souffraient de l’anémie peu grave et modérée respectivement. Le frottis de sang de 74,5%, 15,7% et 11,8% des femmes anémiques ont des images de normocytique normo chromique, hypo chromique microcytique respectivement. Un niveau d’instruction bas [Indice de la cote adapté (ICA)= 2,13] qu’il soit célibataire ou divorcé [ICA=2,02], une parité élevée [ICA=2,06], inscription tardive [ICA=2,7] et de courts intervalles entre des grossesses [ICA =2,37] étaient des indices significatifs de l’anémie pendant la grossesse. La haute prévalence de l’anémie pendant la grossesse qui est liée au niveau inférieur d’instruction et de situation économique surtout chez les femmes qui ont les antécédents des facteurs de risque obstétrique exigent la vigilance, une éducation de santé soutenue et la chémoprophylaxie pour les femmes enceintes (Afr J Reprod Health 2011; 15[4]: 33-41). Keywords: Anaemia, pregnancy, prevalence, risk factors, Kano Introduction Anaemia in pregnancy continues to be a common problem in many developing countries where poverty, ignorance and disease are still prevalent among the people. Worldwide, it is estimated that 58.27 million women are anaemic during pregnancy, of whom 55.75 million (95.7%) live in developing countries.1 Recent estimates suggest that up to 60% of pregnant women in developing countries including Nigeria may be anaemic, and nearly 7% of pregnant women are severely anaemic.2,3 Anaemia is reported to be significantly associated with maternal mortality in developing countries, where it is directly or indirectly responsible for 20-30% of all maternal deaths.1,2,4 The mean minimum acceptable haemoglobin level during pregnancy by WHO criteria is taken to be 11g/dL (PCV of 33%) in the first half of pregnancy and 10.5 g/dL in the second half of pregnancy. The World Health Organization further divide anaemia in pregnancy into: mild anaemia (haemoglobin 10-10.9g/dL), moderate anaemia (Hb 7.0-9.9g/dL) and severe anaemia (haemoglobin < 7g/dL).2 However, using this criteria may mean most women would be classified as anaemic in the developing countries including Nigeria. Therefore a pragmatic classification has been used in these settings where the cut off is adjusted downwards to 10g/dl.11 The aetiological factors for anaemia in pregnancy vary geographically. The reported principal causes in sub-Saharan Africa include nutritional deficiencies, malaria, other parasitic infestations and recently, infection with human immunodeficiency virus.5 Studies have shown that malaria is still a major problem among pregnant women in Nigeria and in other endemic areas.2,6,7 Knowledge of the different causes in a given community is essential for effective control of anaemia. It has been reported that a fall in haemoglobin concentration below 10g/dl cannot be explained by the physiological haemodilution of pregnancy alone, hence its use as a cut off point for diagnosis.8 In pregnancy, anaemia has a significant impact on the health of the foetus as well as that of the mother. The deleterious effects of anaemia in pregnancy include increased risk of maternal and foetal morbidity and mortality, preterm delivery, and low birth weight.8 There is a 500-fold increased risk of maternal, perinatal and infant mortality in pregnant women with severe anemia.4,9 An anaemic pregnant woman succumbs easily to obstetric haemorrhage and puerperal infection which are important causes of maternal mortality in developing countries. Severe anaemia is an important contributor to maternal death through the development of heart failure, particularly around the time of delivery.5 Prevention of anaemia would therefore help to reduce the high maternal mortality in developing countries including Nigeria. Several studies have been conducted on the prevalence and risk factors of anaemia in pregnancy in different parts of Nigeria.2,5,20,37. However, these studies are mainly reported from the south west or south east Nigeria. No recent studies have been conducted in Kano, a highly populous state whose capital city is the commercial nerve centre of northern Nigeria. Northern Nigeria is a socio-culturally distinct region contributing disproportionately to the high national maternal mortality figures. Some of the region’s socio-cultural practices may be inimical to the haematological status of women during pregnancy and puerperium. For instance, there is a cultural preference for early marriage and high parity especially among women with low educational status. Secondly, girls are discriminated against when it comes to opportunities for western education. Similarly, environmental conditions also favor malarial transmission and hookworm infestation. Furthermore, Low contraceptive uptake and short intervals between pregnancies also deplete maternal iron stores predisposing to maternal anemia in the subsequent pregnancy. On the positive side however, husbands are culturally expected to provide resources for high protein meals during the early puerperium. The aim of this study was to determine the prevalence, severity and socio-demographic factors associated with anaemia in pregnancy at the initial booking visit in Aminu Kano Teaching Hospital, Kano. The findings could be useful for health policy makers, clinicians and other health care providers towards reducing the contribution of anaemia towards maternal morbidity and mortality. Methods Setting/Study population The study was conducted among pregnant women attending antenatal care for the first time at Aminu Kano Teaching hospital, Kano, Nigeria. This hospital serves both, as a tertiary and referral health centre for Kano and its environs. Aminu Kano Teaching Hospital (AKTH) is a 500-bed hospital established in 1988. Located in Kano, the largest commercial centre of northern Nigeria with over 9 million people46, this hospital receives clients from within Kano and the neighboring states of Jigawa, Katsina, Kaduna, Bauchi and Zamfara states. Majority of the patients are indigenous Hausa and Fulani, although the Igbo and Yoruba ethnic groups also constitute a substantial proportion of the cliental. Most of the people are traders, farmers, businessmen and civil servants. Design The study was descriptive and cross-sectional. A sample size of 300 was obtained using the hypothesis testing method9 and based on the following assumptions: 95% confidence level, prevalence of anaemia in pregnancy from a previous study5 and a 5% margin of error. The calculated minimum sample size was inflated to account for anticipated subject non-response. Patients who did not give consent, were recently transfused, have haemoglobinopathies or who had chronic medical illness; had early pregnancy bleeding or antepartum haemorrhage were excluded from this study. A systematic sampling technique was used to recruit consenting pregnant women as they registered at the booking clinic. Each clinic day, the sampling interval was determined using the expected patient turnover based on previous records. The first patient is the one whose serial number was randomly selected from a random number table. Subsequent patients were obtained by adding the day’s sampling interval to the previous patient’s serial number. Patient recruitment was continued from 8th November 2008 to 14th January, 2009. Instrument description/Data collection Informed consent was obtained from prospective respondents prior to commencement of the interviews. The content of the consent form was translated into local language (Hausa). Literate respondents indicated acceptance by signing the consent form, while non-literate participants used a thumbprint. Approval for the study was obtained from the Institutional Review Board (IRB) at Aminu Kano Teaching Hospital, Nigeria. A pre-tested structured interviewer-administered questionnaire containing both open and closed-ended questions was used. The questionnaire was adapted from the survey tools used in a previous study.5 It was divided into four parts; the first section inquired about personal data including age, parity, occupation, ethnicity, religion and educational level. The socio economic status of the patient was assessed on the basis of husband’s and patient’s occupation using the single item (occupational) index of Warner’s social classification.47 The second part elicited information about obstetric history and past medical and surgical history. The third section inquired about the history of the current pregnancy. Gestational age was estimated by the Last Menstrual Period (LMP) and Symphisio-Fundal Height (SFH) measurement. Ultrasound scan was utilized for dating in cases of unsure date, first trimester cases or when there was discrepancy between LMP and SFH to rule out multiple gestations. Blood samples of 2.5mls were then collected from all participating clients from the antecubital vein, using plastic disposable syringe and placed in a specimen bottle containing EDTA anticoagulant for determination of PCV and red blood cell morphology. The capillary technique was used for the estimation of the PCV. After centrifugation with the micro-haematocrit centrifuge for 5 minutes of 3000rpm, the PCV was measured using a Hewkley micro haematocrit reader. For the purpose of this study, anaemia in pregnancy was defined as haematocrit of less than 30%.19 The severity of anaemia was classified as follows, mild (PCV 27% - 29%) moderate (PCV 19% - 26%) and severe (PCV below 19%).20 For the blood film, a small drop of blood was placed in the centre of the slide about 1-2cm from one end. A smooth slide was used as spreader at an angle of 450 to the slide. The film was then air dried and flooded with Leishman’s stain. After 2 minutes water was added and the film stained for 5-7 minutes. It was then washed in a stream of buffered water until it acquired pinkish tinge. The back of the slide was then wiped clean, dried and then examined. Data analysis Data was analyzed using SPSS version 16.48 Quantitative variables were summarized using appropriate measures of location and variability. Categorical variables were presented as frequencies and percentages. Bivariate analysis involved the use of the Chi-square test for assessing the significance of associations between anaemia in pregnancy and socio-demographic variables. Crude odds ratios (OR) were obtained using Stat calc. Multivariate logistic regression was used to compute adjusted ORs and to identify independent predictors of anaemia in pregnancy. The level of significance was set at P < 0.05. Results The age of the pregnant women ranged from 15 to 45 years, with a mean age ± standard deviation of 26.6±15.1 years. Modal age was 25 years. Majority of our clients were married (98%), the remaining few were either single or divorced. Nearly half of our booking clients (47.7%) had tertiary education while 11.3% had no formal education as shown in Table 1. The mean parity among the women studied was 2.0± 1.9. Modal parity was zero, with a range of 0-9. Mean gestational age at booking among the pregnant women studied was 21.9±6.8 weeks with a range of 9 weeks to 40 weeks. Prevalence and degree of anaemia There were 51 pregnant women with anaemia in pregnancy (PCV<30%) out of 300 clients giving a prevalence of 17% [95% Confidence Interval (CI) =12.9%-21.7%)]. The PCV ranged from 22% to 42% with an mean PCV of (32%±3.57%). Eighty three percent had normal packed cell volume while 12.7% and 4.3% had mild and moderate anaemia respectively. No client had severe anaemia at the booking clinic. However, when the WHO guideline (PCV<33%) was utilized the prevalence of anaemia increased to 41.7% [95%CI=36.0%-47.5%] (Table 2). Blood Film Appearance The red blood cell morphology of majority of the pregnant clients with anaemia were normochromic normocytic (74.5%), followed by features suggestive of haemolysis (15.7%) and microcytic hypochromic anaemia (11.8%). Macrocytic cells and dimorphic features were not seen in this study. Factors associated with anaemia at booking Anaemia was highest among pregnant women with no formal education (33.3%) and lowest among those with tertiary education (11.4%). The observed difference was statistically significant (χ2=7.9, df=4, p=0.006). Similarly, married women were less likely to be anaemic (16.0%) compared to those who were either single or divorced (66.7% each). This difference was also statistically significant (χ2=10.7, df=2, p=0.005). Furthermore, there was an increase in the prevalence of anaemia as one went down the socioeconomic ladder, being highest among women in the low socioeconomic category (61.1%). This trend was statistically significant (χ2trend=30.5, p=0.003) as shown in II. In addition, the proportion of anaemic pregnant women increased with increasing parity status, being highest among the grandmultiparous women (26.5%). The observed difference was also statistically significant (χ2 =9.9, df=3, p=0.019). Furthermore women who booked in the first trimester were less likely to be anaemic (6.5%) compared to those who booked in the second trimester (14.9%) or third trimester (27.9%) of pregnancy. The observed difference was statistically significant (χ2 =8.3, df=2, p=0.015). Similarly, birth interval significantly affected the development of anemia with prevalence of anaemia higher in those with less than a year’s interval between pregnancies (χ2=19.5, df=4, p=0.001). Pregnant women in the age bracket 20-24 years had the lowest prevalence of anaemia (8.1%) while those in 30-34 years age group had the highest prevalence (26.9%). However, this difference was not statistically significant (χ2=8.5, df=4, p=0.076). Similarly, Anaemia was more common in those who had recent febrile illness (17.9%) as against those who had no such history (15.9%). Anaemia was also found to be less prevalent among those who took antimalarials (15.4%) and haematinics (15.7%) recently against those who did not. However, these differences were not statistically significant. Predictors of Anaemia in pregnancy On bivariate analysis anaemia in pregnancy was significantly associated with educational status, marital status, socio-economic class, parity, inter-pregnancy interval and gestational age at booking. These factors remained significant predictors of anaemia in pregnancy after adjusting for confounding using multivariate analysis. Pregnant women with no formal education had more than twice the risk of anaemia compared to those with tertiary education. Similarly, single or divorced pregnant women had a two fold increased risk compared to those that were married. Women from low socio-economic class had a four fold rise in risk compared to those from high social class. Furthermore, high parity, short pregnancy intervals and late booking all increased the risk of anemia in pregnancy by more than two folds compared to women who were nulliparous, had long inter-pregnancy intervals and booked early respectively as shown in Table 3. The prevalence of anaemia in pregnancy in this study population was 17% (using PCV <30%) and 41.7% (using WHO minimum criteria of PCV <33%). This rate is higher than figures reported in previous studies (using PCV<33%) conducted in Lagos [35.3%]4, Enugu [33.7%]5, Ibadan [51.4%]2 and Benin city [20.7%]10 all in Nigeria. This prevalence is also low compared to figures obtained in some other African countries such as Malawi [57.1%]45 and a district hospital in South Africa [39.9%].19 However, our finding is in tandem with the WHO estimate that about 50.6% of pregnant women in tropical Africa and 30.5% in Nigeria are anaemic at booking.2,7,12 The high prevalence of anaemia at booking in this study may be due to the high proportion of grandmultiparous women in our study population as a result of early marriage, short intervals between pregnancies and cultural pressure for large family sizes. The absence of cases of severe anaemia among our study participants is comparable with the experience at LUTH, Lagos5 but contrasts with the findings in Enugu10 [1.1%] and Ibadan20 [11.8%]. The WHO also reports an expected range of 1 to 5%.22 Selection factors may be responsible for our low values as our hospital is a fee paying centre attracting clients mainly (94.3%) from the middle to higher socio-economic strata. Majority of the pregnant women (72.5%) with anaemia had a normocytic, normochromic red blood cell morphology with only 11.8% having features suggestive of iron deficiency. This is low compared to the findings of other workers.7, 61 The red blood cell morphology in this series might be due to the impact of haemodilution of pregnancy in the presence of low pre-pregnancy haemoglobin. Also a high therapeutic drive with regard to haematinics in this study population, may perhaps have contributed to this modified blood picture. The haemolytic feature (15.8%) is likely due to malaria infestation which is endemic in the study area and is a common cause of febrile illness among pregnant women due to increased susceptibility during pregnancy. This concurs with findings from previous studies in other parts of Nigeria indicating that malaria is still a major problem among our pregnant women.2,5,38 In this study, the proportion of pregnant women with anaemia was not inversely related to their age as seen in some studies from other parts of Nigeria.2,5 The age group 30-34 years had the highest prevalence of anaemia (26.9%) which agrees with the findings in studies done in Enugu and Benin city, 10,19 where it had been related to the effect of parity on increasing maternal age. The influence of age has often not been separated from the effect of parity and pre-pregnancy nutritional status. These have been identified as risk factors of anaemia among pregnant adolescents due to depleted iron stores that occurred during the adolescent growth spurt.4 However, majority of the booking pregnant women in this study who were adolescents were from middle and high socio-economic class, and this may account for a background good nutritional status in them. Some other studies from Africa have confirmed the findings of this study, that age alone is not a significant determinant of haemoglobin value in pregnancy.4,5 The prevalence of anaemia among booking pregnant women in this study was inversely related to their educational and socio-economic status. Anaemia was significantly higher among women with no formal education compared to women with formal education. Also women from the low socioeconomic class (64.7%) were significantly more affected by anaemia compared to those in higher socioeconomic classes. this corroborates with reports from other studies in other parts of Nigeria.5 Elsewhere in Africa, a report from Malawi, where a higher proportion of the population are impoverished and largely uneducated, the prevalence of anaemia was found to be as high as 90%.45 Women in low socioeconomic class, because of lack of education or financial constraints may not afford or have access to good maternal health services. They are therefore, more prone to the deleterious effects of poor nutrition, malaria, diarrheal diseases and chronic infections. It is these same women who may have background iron deficiency anaemia before pregnancy. The direct relationship between parity and anaemia observed in the current study concurs with an earlier report19 and this could be explained by repeated drain on the iron reserves with increasing parity. However, this result is at variance with the observation of other workers who reported highest prevalence of anaemia in primigravid patients5,45, and attributed these differences to increased susceptibility to malaria in the primigravida. Perhaps other factors such as occurrence of pregnancies in quick succession and overconfidence induced late booking, which is more common in multigravidae, and grandmultiparous women, may have contributed to this finding. The observed increased risk of anaemia among women who booked during second and third trimester of pregnancy is similar to the reports from several other studies.2,4,42 This could be explained by the expected decline in Haemoglobin level due to haemodilution, increasing fetal demand, underlying maternal infection and untreated anaemia in early pregnancy may also get worse with advancing pregnancy. It is also noteworthy that majority (83%) of the pregnant women booked for antenatal care during the second and third trimester. This is similar to reports from other studies2,4,5,19. Perhaps the advice about the time to register for antenatal care is mainly obtained from friends and relatives rather than from health personnel. This places the woman and the health care providers in a difficult situation due to the limited time for optimum correction of any observed anaemia. This is therefore, a wake up call for health care providers to use effective media for informing women and men in communities of the importance of early booking. The higher risk of anaemia among women with shorter pregnancy intervals in the present study is similar to the findings in a previous study.5 This short interval between pregnancies, delays the mother’s recovery from the effects of previous pregnancies thus increasing the risk of maternal depletion syndrome. Since the foetal demand is met first, the mother is left with further depleted iron stores and thus anaemia develops. It has been shown that the exhausted maternal iron stores at the end of one pregnancy takes almost two years to be replenished.34 Although not statistically significant, the association of anaemia with positive history of recent febrile illness in the index pregnancy could be due to the endemicity of malaria in the study area. Malaria is endemic in Nigeria and is a common cause of febrile illness among pregnant women. In addition, anaemia was less common in those women who had used antimalarial drugs or haematinics before booking visit than in those who had not used any of these medications. This corroborates the earlier findings of Fleming et al and Anorlu et al.5,38 The findings of the present study further supports the basis of anaemia prevention in sub-Saharan Africa, which is hinged on control of malaria and haematinic supplementation.5 However, innovative delivery systems need to be used to reach the high proportion of pregnant women who do not attend antenatal clinics. This study had several limitations; being a facility based study, the effect of selection bias limits the generalizability of our findings to the whole populace. Pregnant women utilizing our centre are more likely to be educated, of higher socioeconomic status than the typical pregnant woman in the community. Being a teaching hospital, our centre is also likely to attract women with problems during earlier pregnancies and those anticipating problems during the current pregnancy. Inexperienced primigravidae are also more likely to be attracted to such centers. Therefore our findings are valid for women booking at our centre and similar tertiary hospitals in the region. Our figures may underestimate the burden of anemia in pregnancy, since majority of women either attend antenatal care at primary health care centers, in general hospitals or do not attend at all. A multicentre study stratifying for these variations, a systematic analysis of the outcome or better still a sample of pregnant women obtained during the Demographic and Health Surveys (DHS) will be more representative of the populace. We therefore strongly suggest the study of a sub-sample of pregnant women during subsequent DHS to obtain a more accurate estimate of the prevalence of anemia in pregnancy. Secondly, this study did not explore all possible aetiologies of anemia. Hence, further laboratory evaluation for other underlying causes of anaemia especially infections such as HIV and hookworm infestation could be done in the future. Again, maternal and fetal outcome of anemic patients were not pursued. There is a need to do such studies also in the future. Conclusion This study has shown that anaemia in pregnancy is still prevalent even in selected population of pregnant women in an urban setting identifying high parity, late booking, short pregnancy intervals, low socio-economic and low educational status as risk factors. In the light of this, it is recommended that good antenatal care should be made available, accessible and affordable to all pregnant women through partnership between all tiers of government and non-governmental organizations. Due to the self selection of women who either experienced problems during previous pregnancies or anticipate problems in the present one, health care providers in our centre and similar centers need to be more vigilant during booking visits to identify cases and use it as a platform for health education with respect to the need for good nutrition and compliance with medication. More importantly, this would enhance early detection of anaemia and prompt treatment using haematinics considering the increasing risk of blood transfusion. They should also receive intermittent prophylactic treatment for malaria to clear asymptomatic or undetected malaria during antenatal period. Effective birth spacing among our women should be encouraged. Affordable contraceptive methods should be made available at all levels of health care. Late booking should be eliminated through appropriate health education and community mobilization. Husbands are very powerful in the decision-making process in this part of the world, so they need to be educated on the importance of providing permission, support and actual involvement in maternal health care including focused antenatal care and family planning. The media and civil society organizations could form strong allies in this regard. In the long term, education and improvement of the socioeconomic status of our women folk in the African sub-region by regional governments are the cornerstones to eliminating anaemia in pregnancy. Education will lead to increased awareness and better utilization of antenatal care and family planning services with all its attendant benefits. Economic empowerment as a result of education will improve the sanitary and nutritional behavior of the women, hence by extension the family and the community at large. Further studies in this direction can be done to ascertain the prevalence and pattern of anaemia at the community level. This would aid in planning appropriate health care services. The burden of anaemia is probably worse than reported, since the population studied is a low risk group compared to those who did not register or receive antenatal care at all and resident in the rural communities. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11048t1.jpg] [rh11048t2.jpg] [rh11048t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}