 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 4, Dec, 2011, pp. 42-50 Original Research Article Introducing misoprostol for the treatment of incomplete abortion in Nigeria Introduction de Misoprostol pour le traitement de l’avortement inachevé au Nigéria Talemoh Dah1, Akinsewa Akiode2, Paschal Awah*1, Tamara Fetters1, Mathew Okoh2, Innocent Ujah3 and Ejike Oji2 1Ipas, Chapel Hill, NC 27516; Code Number: rh11049 Abstract Despite legal restriction, induced abortions and resulting complications are common in Nigeria. Misoprostol administration for incomplete abortion was introduced in 3 Nigerian hospitals. The feasibility of the hospitals, patient and provider acceptability were assessed using questionnaire and interview guides administered to 205 women and 17 providers respectively. Amongst the women, 194 (95%) were satisfied and very satisfied with misoprostol, 176 (86%) would choose misoprostol again if another incomplete abortion occurred and 191 (93%) would recommend it to another woman in a similar situation. Providers were highly satisfied with misoprostol. The ease of use and ability to redirect surgical resources to more complicated issues were positive features cited by them. The providers agreed that integration of misoprostol was straightforward and required few resources. Therefore, misoprostol for incomplete abortion is safe, efficacious and acceptable to providers and patients. In remote areas of Nigeria with limited post-abortion care (PAC), misoprostol administration is an important potential PAC treatment modality. Features of misoprostol-low cost, room temperature stability, and ease of introduction-render it an important treatment option, particularly in low resource and rural settings (Afr J Reprod Health 2011; 15[4]: 42-50). Résumé Malgré la limitation judiciaire, les avortements provoqués et les implications éventuelles sont communs au Nigéria. L’administration de Misoprostol pour l’avortement inachevé a été introduite dans trois hôpitaux nigérians. Nous avons évalué la faisabilité des hôpitaux, l’acceptabilité des patientes et des dispensateurs é l’aide des questionnaires et des interviews auprès des 205 femmes et 17 dispensateurs respectivement. Parmi les femmes, 194 (95%) ont été satisfaites et très satisfaites de Misoprostol. 176 (86%) choisiraient Misoprostol encore si elles subissent un autre avortement inachevé et 191 (93%) le proposeraient aux autres femmes qui se trouvent dans une situation pareille. Les dispensateurs étaient hautement satisfaits de Misoprostol. La facilité de l’utilisation et la capacité de réorienter les ressources chirurgicales vers les problèmes plus compliqués constituent des qu’elles ont citées. Les dispensateurs étaient d’accord que l’intégration de Misoprostol est facile et ne demande que peu de ressources. En conséquence, Misoprostol n’est pas dangereux pour le traitement de l’avortement inachevé, il est efficace et acceptable aux dispensateurs et aux patientes. Dans les régions rurales isolées au Nigéria, qui ne disposent que très peu de soins du post-avortement (SPA) limités, l’administration de Misoprostol est une modalité de traitement du SPA potentiel important. Les caractéristiques de Misoprostol : bon marché, stabilité à la température ordinaire et la facilité de l’introduction, le rend une option de traitement importante, surtout dans les milieux é faibles revenus et dans les régions rurales (Afr J Reprod Health 2011; 15[4]: 42-50). Keywords: Misoprostol, Post-abortion care, Unsafe abortion, Maternal mortality, Nigeria IntroductionUnsafe abortion is a major public health problem that threatens the lives of women around the world, particularly in developing countries. Global data indicate that legal restrictions on abortion do little to affect abortion rates, but instead only serve to shift the balance of abortion procedures from those that are legal and safe, to those that are unsafe.1-2 This scenario is in evidence in Nigeria where, despite a restrictive abortion law, a 2006 study estimated that 760,000 pregnancies ended in abortion.3 A survey conducted from 2002-2003 in 33 hospitals across Nigeria found that of the 2,093 women admitted for abortion-related reasons, 36% had attempted to end their pregnancy, 24% of whom suffered serious complications.4 The same study estimated that at least 3,000 women die in Nigeria every year from unsafe abortion, likely an underestimate given that stigma, fear of legal reprisals and deaths outside of the hospital contribute to gross under-reporting of abortion related mortality.5 Post-abortion care (PAC) is an approach for reducing deaths and injuries from incomplete and unsafe abortions by removing the remaining products of conception from the uterus and treating associated complications, such as bleeding or infection. In Nigeria treatment of incomplete abortion, whether spontaneous or induced, often involves evacuation of the uterus with manual vacuum aspiration (MVA) or sharp curettage. Uterine evacuation with MVA, a highly effective technology and useful in low resource settings, is the standard of care for women with incomplete abortion and a uterine size of less than 12 weeks.6,7 However, in remote areas of Nigeria, the shortage of skilled health-care providers and equipment often limits women’s access to treatment with MVA.8 In some settings, mid-level providers face barriers to providing PAC, including restrictive facility policies and lack of training opportunities.8 Research has shown insufficient use of, inadequate access to and low availability of uterine evacuation services in Nigeria despite the great need.9 A growing body of evidence has demonstrated that medical treatment of incomplete abortion with misoprostol is an effective alternative to MVA or sharp curettage10-15Misoprostol, a prostaglandin-E1 analogue, is a safe and effective treatment for multiple obstetric and gynaecologic indications, including postpartum hemorrhage, induction of abortion and induction of labor, among others.16 Misoprostol’s ability to induce uterine contractions and to soften the cervix makes it similarly effective in emptying the uterus following incomplete abortion.16 In studies involving at least 100 women, misoprostol for incomplete abortion has demonstrated an average efficacy of 95%, with the highest success rate being 99% - rates comparable to treatment with MVA. 14,17-18 Misoprostol is relatively inexpensive, easy to administer and stable at room temperature; it requires few resources and can be administered by low- and mid-level providers without surgical skills.19 These features render misoprostol an important alternative to PAC with MVA, particularly in low-resource and remote areas. In light of this evidence, the World Health Organization has recently added misoprostol for managing incomplete abortion to its Model List of Essential Medicines.20 Though used for other obstetric indications in Nigeria, misoprostol had not been introduced into the country’s health-care system for treating incomplete abortion at the time of this research. In 2010 the National Council of Health began advocating for greater use of misoprostol for this purpose and in 2011directed that the guidelines on Misoprostol use at the community and facility levels be “widely disseminated”. The Federal Ministry of Health has now developed these guidelines which includes misoprostol for the treatment of incomplete abortion. However, little is known about the potential appeal of misoprostol to Nigerian women or providers. The Society of Gynaecology and Obstetrics of Nigeria (SOGON) and Ipas Nigeria piloted the use of misoprostol for incomplete abortion in three tertiary hospitals to demonstrate the safety, feasibility and acceptability of this treatment modality in the Nigerian health care system. Methods Overview To examine the feasibility and acceptability of introducing misoprostol for treatment of incomplete abortion in Nigeria, SOGON and Ipas Nigeria conducted a study examining the integration of misoprostol for uterine evacuation into existing PAC services at three tertiary hospitals in Nigeria. The study offered eligible women the opportunity to use misoprostol, as an alternative to MVA, to complete their incomplete abortion. Interviews with study participants and providers assessed their experience and satisfaction with the method. Study facilities Three tertiary care facilities in Nigeria were purposively selected to participate in the study, based on their role in providing PAC and PAC training, their geographic distribution and their interest: Murtala Mohammed Specialist Hospital (MMSH) located in Kano, Federal Medical Centre in Abeokuta, and Federal Medical Centre in Abakaliki. MMSH is one of the largest public hospitals in northern Nigeria and serves a predominantly Hausa population. It has the highest post-abortion caseload in the region, with approximately 2 000 PAC cases a year. The centres in Abeokuta and Abakaliki, located in southern Nigeria, serve smaller populations largely from the Yoruba and Igbo ethnic groups, respectively. These two hospitals use MVA for PAC, provided by physicians, residents, interns, midwives and nurses. At MMSH, services are managed and run by midwives, and more than 90% of PAC cases are treated by nurse midwives. Prior to training in misoprostol use and the study protocol, human and material needs necessary for successful introduction of misoprostol were assessed at each study site, the results of which have been previously made available.21 Prior to the introduction of the protocol, a total of 80 health care providers from these facilities, including physicians, residents and midlevel providers, were trained in both provision of misoprostol and the study protocol. These two-day trainings included values clarification exercises, an introduction to the study and study procedures, patient inclusion criteria (Table 1), follow-up procedures and adverse event reporting, pharmacology of misoprostol and its use for incomplete abortion and other gynaecological indications, counseling and clinical management, warning signs and management of complications, and post-abortion contraception, among other topics. Adequacy of training was confirmed with pre- and post-testing of trainees. Between 12 and 25 providers from each study center were trained; trainings were conducted in June and July 2009. Table 1: Criteria for participant inclusion in study
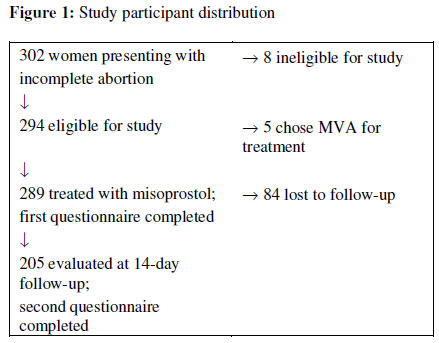
Study protocol Women aged 18 to 49 seeking treatment for incomplete abortion at the three participating hospitals were counseled regarding their available treatment options-either typical care using MVA for uterine evacuation, or a single dose of misoprostol (400 mcg sublingually). Although ultrasounds were available in these hospitals, during follow-up appointments physical examinations, questions about the mechanism of action of the misoprostol and ongoing pregnancy symptoms were used to assess completion of the abortion rather than ultrasound confirmations. If a woman failed any of the three tests and the provider was suspicious of an ongoing pregnancy ultrasound confirmation was employed. Women choosing misoprostol were invited to participate in the study. Informed consent was obtained from eligible women who agreed to participate. Participants were administered misoprostol, after which they were asked to wait at the facility for 30 minutes to allow the medication to be absorbed and to ensure no adverse reactions to the medication. During this waiting period, initial face-to-face study interviews were conducted using a questionnaire including quantitative and open-ended questions, after which women were discharged. Participants received a picture-based, take-home information sheet, translated into local languages, explaining expected effects of misoprostol, potential warning signs of complications, their provider’s telephone number to use if needed and a follow-up appointment 14 days from the initial drug administration. Women returned two weeks after misoprostol administration, at which time completion of pregnancy expulsion was confirmed by women’s self-report of symptoms of abortion and bimanual examination. Women with signs or symptoms of continuing pregnancy were referred for ultrasound examination, and those with retained products were treated with MVA evacuation of the uterus. At the time of the follow-up appointment, study participants were invited to participate in a second interview about their experience using misoprostol. Upon the initial visit and enrollment in the study, women were counseled about the need to return for their follow-up appointments to confirm a complete abortion and also told to return to the facility at any time if they felt extraordinary pain or bleeding. Although every effort was made to encourage compliance to this protocol, it is possible that some women could have had retained products of conception and returned after the study completed or sought care at a health facility outside of the enrollment sites. Two study facilities (Federal Medical Center of Abakaliki and Federal Medical Center of Abeokuta) typically charge clients a fee for PAC. In order to ensure that free services were not an enticement to join the study, fees for PAC for all eligible women during the data collection period were paid by the study. PAC services at Kano are free to all women. Data collection Women were interviewed twice as part of the study protocol. The first interview was conducted 30 minutes after administration of misoprostol, and consisted of socio-demographic questions and questions related to abortion technology choice and reproductive history. The second interview was conducted after the participant’s follow-up visit, and queried their experience with the use of misoprostol, including side effects, complications, satisfaction and quality of care received. Pain was measured using a 7-point visual analog scale using circles ranging in size from small (no pain) to large (intense pain) to quantify intensity. Open-ended questions asked participants to report the best and worst features of treatment with misoprostol. Treatment outcome, based on the provider’s assessment, was captured from the patient record at this time. Six midlevel health professionals (two per hospital) were trained as data collectors. Data collectors participated in the two-day clinical training, and completed additional training specific to the study protocol, patient flow, questionnaires and the informed consent process. Data collection took place from 8am to 9pm daily, including weekends, during the study period. In addition to data collection, the data collectors enrolled participants in the study, monitored participant follow-up, and contacted those participants lost to follow-up by telephone when possible. All participant data was collected between May and September 2009. Acceptability and satisfaction with implementation of misoprostol for incomplete abortion was evaluated among health care providers involved in counseling or provision of misoprostol treatment during the study period. Providers who counseled at least one study participant and who agreed to a recorded interview were eligible to participate. Semi-structured interviews were conducted in English, or in the provider’s preferred language (of Hausa, Igbo or Yoruba), by a consulting community health physician. Data management and analysis Participant data were managed using EpiInfo 2005, and were exported into SPSS version 16for analysis. Descriptive statistics are presented. Due to small numbers of participants from the Abakaliki and Abeokuta sites, subgroup analysis by site was not possible. Provider interviews were transcribed verbatim. Transcripts were coded by the lead social scientist using a standardized coding scheme agreed upon by the research team. Coded transcripts were reviewed by the researchers to ensure uniform application of the scheme; emergent themes were discussed by the researchers for analysis and interpretation. All disagreements between researchers were resolved by discussion. Ethical review The study protocol and associated materials were approved by the Allendale Institutional Review Board, based in Allendale Pennsylvania, USA, and by the Ethical Committee of the Federal Medical Centre in Abeokuta, the Federal Medical Centre in Abakaliki and by the Ethical Committee of the Kano State Health Management Board. Results Sociodemographic characteristics of participants Three hundred and two women presented to the three study sites with incomplete abortions during the study period; of those, 289 (98%) of the 294 women eligible for inclusion in the study chose treatment with misoprostol (Figure 1). The perception that using pills was easier than uterine evacuation with MVA was the most commonly reported reason for choosing treatment with misoprostol (Table 2). The majority of study participants were from the Kano site (N=273, 94%), with fewer participants in the Abakaliki (N=7, 2%) and Abeokuta (N=9, 3%) sites. All participants enrolled received misoprostol and completed the initial study interview; 205 women (70.9%) returned for their 14-day follow-up assessment, for a loss to follow-up of 29.1%. All participants who returned for follow-up agreed to a second study interview. Table 3 presents socio-demographic characteristics and reproductive histories of study participants. No significant demographic differences were found between those women who completed follow-up and those who did not return. Success of misoprostol treatment Of the 205 women who returned for follow-up, 13 (6%) with physical signs or symptoms of continuing pregnancy were referred for ultrasound exams; only four participants (2%) received uterine evacuation with MVA to complete the abortion process at the time of follow-up, as per the research protocol. Two hundred and one women (98%) had a complete evacuation of the uterus using misoprostol. No serious adverse events were reported during study follow-up, however one participant required blood transfusion outside of the two-week follow-up period. After additional investigation by the research team the bleeding was deemed to be unrelated to the woman’s treatment with misoprostol. Table 2: Participants’ reasons for choosing misoprostol instead of MVA (N=203)*
*Participants allowed to give more than one response. Table 3: Participant characteristics (N=289)
SD=standard
deviation Participant experience with misoprostol treatment One hundred and ninety-five women (95%) reported that they were satisfied or very satisfied with the care they received for their incomplete abortion; a similar proportion (86%) stated that they would choose misoprostol again if they needed it or would recommend it to a friend (93%) (Table 4). Few women (24, 11.7%) reported any ‘worst’ feature of misoprostol treatment; those who did cited prolonged or heavy bleeding (12, 5.9%) or prolonged lower abdominal pain (10, 4.9%) most commonly. Women’s reported mean duration of bleeding was seven days (SD=4.12). The mean reported pain was 2.76 (SD=1.59) on a scale from zero to seven. A list of all symptoms experienced by women is contained in Table 5. Table 4: Women’s reports of satisfaction and acceptability (N=205)
*Percentages may exceed 100% as participants could report up to two features. “Good provider-patient interaction” and “no surgery or instrumentation” were the most frequently reported best features of misoprostol use, at 35% and 30% respectively. Post-abortion family planning Fifty-five (27%) participants who returned for their follow-up stated that “they do no want to get pregnant soon.” Of this number, 40 (73%) said they were offered a contraceptive method; 20 at their first visit, 19 at their second visit and 1 at both visits. Nine women (14.7%) were not offered any method at all. Table 5: Symptoms experienced after misoprostol administration among women who returned for follow-up (N=205)*
*Percentages
exceed 100% as patients directed to report all symptoms experienced; Provider experience using misoprostol Of the 80 providers trained in the use of misoprostol, 19 were eligible for interview, having provided misoprostol to one or more clients during the study period. Seventeen eligible providers (11 nurse-midwives and 6 physicians) agreed to participate. These providers identified as Christian (58.8%) and Muslim (41.2%). The nurse-midwives were all female, the physicians were all male. All providers were satisfied with the use of misoprostol for PAC, and interested in continuing to use this modality both in study centres and their private practices. The most important perceived benefit of misoprostol was ease of use by patients and by providers. Most providers reported that although counseling for use of misoprostol takes time, it is less stressful and time-consuming than preparing for an MVA procedure, and allows use of scarce procedural resources for other, more complicated conditions; one provider found the level of counseling burdensome. Most providers believed that patients found misoprostol to be simple to use, non-invasive, convenient and less anxiety provoking than uterine evacuation with MVA, although one provider expressed concern that offering a choice of method (MVA or misoprostol) for incomplete abortion treatment could be confusing, particularly for less educated patients. Providers attributed the high lost to follow-up rate of the study in part to patient comfort with use of misoprostol and what to expect after taking the medication. One provider summarized the patients’ perspective as follows:
Given the limited material needs required for implementation of misoprostol use, providers assessed that it is more easily integrated into clinical care than MVA services:
To sustain its use, providers recommended that misoprostol be included on the health facility essential medicines list and made available for use. They reported that existing hospital infrastructure was adequate to deliver high quality PAC with misoprostol. Providers called for improvement in post-abortion family planning services. Although all providers reported offering PAC patients family planning on the initial day of consultation, immediate uptake rates were low. Many women deferred accepting a method until they could discuss contraception with their partners; unfortunately many of these women did not return for follow-up. Discussion This study illustrates the feasibility and acceptability of integrating misoprostol for the treatment of incomplete abortion into established PAC services in three tertiary care centres in Nigeria. Treatment with misoprostol was found to be safe and efficacious, and both patients and providers reported high levels of satisfaction with its use. Patients eligible to participate in the study overwhelmingly chose misoprostol over MVA for treatment of their incomplete abortion. In addition, the majority of patients reported that they would choose misoprostol again, and recommend its use to a friend. As has been reported previously,13-15, 22 pain and vaginal bleeding were the most commonly reported side-effects of misoprostol use, however this does not appear to have affected patient satisfaction. Providers expressed enthusiasm for the method, and reported that they would like to continue using misoprostol to treat incomplete abortion. Providers viewed administration of misoprostol as less time consuming than uterine evacuation with MVA and felt that the method was easy to introduce. It is possible that providers’ assessment of misoprostol as less time-intensive than MVA influenced their counseling, and thus contributed to the high proportion of women choosing misoprostol treatment. This possibility has been identified in other similar research and is difficult to control for. However, mock counseling sessions and role-plays conducted during training repeatedly emphasized the advantages of both methods, and the need to allow women to make an informed choice. Only one provider expressed concern that the additional counseling required for use of misoprostol was burdensome to hospital staff and potentially confusing for patients. This study adds to the growing body of evidence supporting the provision of misoprostol for PAC in remote or resource limited settings. Although the study was conducted in tertiary care centres, ultrasound was employed only when completion of abortion could not be confirmed by patient report and bimanual examination, and was utilized for only 13 women, four of whom required further intervention or aspiration of the uterus. The majority of study providers were nurse-midwives, establishing the ability of midlevel providers to successfully administer misoprostol for incomplete abortion. Over 98% of participants in the study were from the Kano area, and were treated in a ward run by midwives, with visiting gynecology consultants available when necessary. Further, these providers confirmed that few resources are required for implementation of misoprostol use - a reliable supply of the medication and adequate training in its use were perceived as the only necessary inputs. Future operational studies should evaluate implementation of misoprostol at secondary- and primary-care levels. This study is limited by a high lost to follow-up rate of nearly 29.1%, which could be unique to this study group or this method. The outcomes for those women who did not return for their scheduled follow-up are not definitively known, however it is plausible that women failed to follow-up because they felt confident that the abortion process was complete, as the study providers suggest in their interviews. Upon enrollment women were asked for their own cellphone number or one of a trusted friend or family member. For women who did not return at the time of their scheduled follow-up appointments, one to three return calls were made to encourage them to return to the facility and to ask about their experiences. Nearly all women who were reached by telephone replied that their treatment was successful, the abortion had been completed, and they did not feel a need to return to the hospitals for assessment even as data collectors continued to encourage them to return to the hospital for assessment. The feedbacks were recorded in the logbooks and included in the database. All women enrolled in the study were in the process of an incomplete abortion and were asked to return more than a week after treatment. Randomized clinical trials report efficacy rates of nearly 100% among women who were not assessed by ultrasound, returned seven days or more post-treatment; these studies report few to no adverse outcomes at the time of follow-up.18 Given the confirmed high rate of efficacy of misoprostol for incomplete abortion,10-15,17 a high incidence of retained tissue or complications among those women who did not return for follow-up is unlikely. Very few follow-up visits prove to be medically necessary for women undergoing misoprostol treatment;16 instead of routine follow-up, health systems implementing misoprostol for incomplete abortion can consider offering women a follow-up visit, and educating women about the symptoms of retained tissue and infection or ongoing pregnancy so they will know if a follow-up visit is necessary. Removing requirements for routine follow-up may help decrease strain on providers, health systems and patients. Such requirements need to be considered for any future standards and guidelines for the use of misoprostol for PAC in Nigeria. Post-abortion contraception is an important consideration in the implementation of any PAC services. In this study, although providers reported that they routinely offered post-abortion contraception to their patients, only three-quarters of women who stated that they did not want to get pregnant were offered a family planning method, and only one woman was offered family planning at her initial and follow-up visits. Fertility can return quickly after a pregnancy loss, and most contraceptive methods (with the exception of intrauterine devices and sterilization) can be offered at the time misoprostol is provided.16 Given the loss to follow-up rate of 29% in this study, and women’s ability to determine for themselves if treatment with misoprostol has been successful, ensuring that women who desire contraceptives are provided with their choice of method on the day of misoprostol use is crucial. Adequate training in post-abortion contraception and availability of family planning methods at a reasonable cost are necessary to prevent future unwanted pregnancies, and should be emphasized in all misoprostol implementation efforts. Although study centres were purposively chosen to evaluate the feasibility of misoprostol implementation in a variety of geographic areas and among different ethnic groups in Nigeria, the vast majority of study participants were drawn from the MMSH facility in Kano. This is likely related to this facility’s long standing history as a PAC provider, high PAC caseload (approximately 1,920 PAC cases per year) and the fact that this facility is well known in the state for providing PAC services free of charge, unlike the other hospitals included in this study which charge user fees. Although misoprostol treatment was successfully implemented in all three facilities, the small number of participants recruited from the Abakliki and Abeokuta centres limits the ability to draw conclusions about the areas and populations that these centres serve. It is worth noting, however, that all eligible participants in these two centers chose misoprostol over MVA for treatment. Cost of treatment for incomplete abortion is an important consideration for implementation of misoprostol use. Per agreements with each of the participating hospitals, women in this study were not charged for their PAC services. These agreements were implemented to ensure that cost was not a factor in patients’ choice of method. Fees for PAC with MVA or misoprostol should be affordable and standardized to ensure they do not influence a woman’s choice of treatment. Ideally, given that PAC services are often life-saving and can be emergent, such services would be provided to all women free of charge. In 2010 the National Council of Health approved community use of misoprostol for prevention of postpartum hemorrhage (PPH) and began advocacy for greater use of misoprostol for the treatment of incomplete abortion. In 2011 the National Council gave directions that guidelines on misoprostol use at the community and facility levels should be widely disseminated. Although a joint statement was issued in June 2010 by the Federal Ministry of Health and the Society for Gynecologists and Obstetricians recommending the use of misoprostol for the treatment of incomplete abortion, no specific mandate or protocols have been put forward. The use of misoprostol for the treatment of incomplete abortion has yet to be included in the National Reproductive Health Standards and Guidelines and the drug has yet to be included in the National Essential Drug List (NEDL) for any indication. Conclusions As Nigeria strives to meet Millennium Development Goal 5b-to reduce maternal mortality by 75% by 2015-misoprostol for PAC is an important treatment modality. In facilities where MVA is available, use of misoprostol can decrease demand on surgical services, and allow for more timely provision of PAC. Where MVA is unavailable, such as in remote and rural settings with limited or absent PAC services, uterine evacuation with misoprostol can decrease abortion related morbidity and mortality. Integrating misoprostol into the health system will initially require training of health care providers, increasing drug availability and government willingness and commitment to provide and promote guidelines for its use for incomplete abortion. In addition, adequate post-abortion contraceptive services are necessary to prevent future unwanted pregnancies, the root cause of unsafe abortion and abortion related mortality. Family planning counseling should be integrated into all PAC services, including those using misoprostol, and methods made immediately available at reasonable cost to those women who want them. Misoprostol treatment for incomplete abortion is safe, efficacious and acceptable, both to providers and patients. The features of misoprostol-low cost, stability at room temperature, and little capacity required for its introduction-render it an important treatment option in Nigeria. The use of misoprostol in the national guidelines should be extended to include incomplete abortion and it should also be included in the NEDL. Acknowledgements We would like to thank the Abakaliki, Abeokuta and Kano study site staff for their partnership and commitment to this research. Similarly, Society of Gynaecology and Obstetrics of Nigeria partners, Drs. Moses Alao, Bello Dikko and Perpetua Ibekwe, made this research possible. Countless people at Ipas contributed to the review and success of this training, research and final documents, including: Traci Baird, Janie Benson, Bill Powell, Rodolfo Gomez, Ramatu Daroda, Sarah Packer, Robyn Sneeringer, Ijeoma Ogbuagu, Bridget Okeke and Sikiratu Kailani. Finally, thanks to Dr. Emily Jackson who helped review this manuscript. This research was funded by Ipas. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11049f1.jpg] |
| |||||||||

{kind=link}