 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
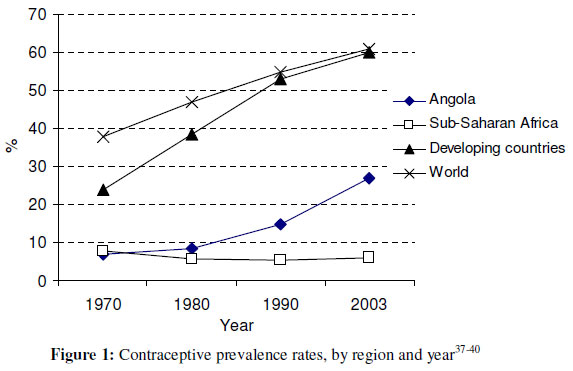
African Journal of Reproductive Health, Vol. 15, No. 4, Dec, 2011, pp. 68-77 Original Research Article Factors associated with contraceptive use in Angola Facteurs lies à l’utilisation des contraceptives en Angola Martha Decker1 and Norman A Constantine2 Philip R Lee Institute for Health Policy Studies, University of California, San Francisco, USA; 2Department of Community Health and Human Development, University of California, Berkeley, USA *For correspondence: Email:Mara.decker@ucsf.edu Tel: (415) 476-3375 Fax: (415) 476-0705 Code Number: rh11053 Abstract After emerging from decades of civil war, Angola’s economy has rapidly grown, yet its reproductive health outcomes have not improved at a commensurate level. At the time of this study, Angola had one of the highest rates of maternal mortality and fertility in the world. Only 6 percent of women aged 15-49 used contraception, with substantial differences in use and access across the different provinces of the country. This study uses a mixed-methods approach, combining analyses of a nationwide cross-sectional survey to assess which factors are associated with contraceptive use, with data from qualitative, semi-structured interviews of health care providers and internally displaced women to better understand and illuminate the survey data. High educational level and living in the capital region were strongly associated with contraceptive use, while age below 20 years was negatively associated with use. During qualitative interviews, health professionals commonly mentioned rural living, young age, cultural beliefs, and power imbalances as reasons for not using contraception. Internally displaced women often described difficulty paying for services, lack of nearby services, and limited knowledge of methods as barriers to use (Afr J Reprod Health 2011; 15[4]: 68-77). Résumé Après avoir survécu des décennies de guerre civile, l’économie de l’Angola connaît un accroissement rapide, pourtant les conséquences de santé de la reproduction ne se sont pas améliorées de la même manière. Au moment où s’effectuait cette étude, l’Angola avait l’une des taux de mortalité et de fécondité les plus élevés du monde. Seuls 6% des femmes âgées de 15-49 ans utilisaient des contraceptifs, avec des différences significatives dans l’utilisation et l’accès à travers les diverses provinces du pays. Ce travail se sert d’une approche des méthodes mixtes, tout en combinant les analyses d’une enquête transversale qui couvre le pays entier ; l’objectif est d’évaluer les facteurs liés à l’utilisation des contraceptifs à l’aide des données obtenues des interviews semi-structurées recueillies au sein des fournisseurs de soins de santé et chez les femmes déplacées à l’intérieur du pays pour mieux comprendre et éclairer les données de l’enquête. Le haut niveau de scolarité et de vie dans la région de la ville capitale ont été fortement liés à l’utilisation des contraceptifs alors que l’âge de moins de 20 ans a été lié de manière négative à l’utilisation. Au cours des interviews qualitatives, les professionnels de santé mentionnaient fréquemment la vie rurale, la jeunesse, les croyances culturelles et les déséquilibres du pouvoir, comme des raisons pour le non-usage des contraceptifs. Les femmes déplacées à l’intérieur du pays ont souvent décrit la difficulté éprouvée pour payer les services, le manque des services voisins et une connaissance limitée des méthodes comme constituant des obstacles à l’utilisation des contraceptifs (Afr J Reprod Health 2011; 15[4]: 68-77). Keywords: Contraception, Angola Introduction Angola recently emerged from 27 years of war, during which time its contraceptive prevalence rate remained very low and stagnant. Only 6 percent of women aged 15-49 currently use contraception, the second lowest rate in the world1. Angola’s low rate of contraceptive use and its high fertility rate correspond with extremely high rates of maternal mortality and under-five mortality 2,3. To gain a more detailed perspective of the individual and structural factors associated with the use of contraception in Angola, this paper combines quantitative data from a nationwide cross-sectional survey with qualitative interview data from health professionals and internally displaced women. By identifying and understanding these use-related factors, some potential barriers to use could be addressed and positive predictive traits supported. These results may also provide insight for researchers and health care providers working in other countries affected by war. In the past three decades, worldwide contraceptive use and availability have increased dramatically, yet these changes have varied substantially by region 4,5. As Figure 1 illustrates, the contraceptive prevalence rate (CPR) for sub-Saharan Africa continues to lag behind the rest of the world, even compared to other less developed regions. The CPR for Angola has remained stagnant for more than three decades at only one tenth the average rate found in developed countries, and one fourth of the average in sub-Saharan Africa6. During most of these years, Angola’s population was engaged in a prolonged civil war. Prior research has investigated barriers to access for contraceptive use in developing countries well as individual factors associated with use. Barriers include financial cost, distance to service delivery site, and provider bias, among others (1-3). Positive factors include female education, partner approval, and urbanization (4, 5). These issues, however, have not been well studied during wartime or in post-conflict settings. Personal characteristics associated with the use of contraception have been investigated extensively, with women’s education level consistently found to be a strong predictor in sub-Saharan Africa and globally 7,8. Research in developing countries also has found an association between economic factors, such as higher levels of women’s employment and income, and increased contraceptive use and lower fertility levels9. These findings have been less robust for sub-Saharan Africa than for most of Asia and Latin America, with many African countries having a higher fertility rate and lower contraceptive use than those at comparable stages of socioeconomic development elsewhere 10. However, substantial individual differences in contraceptive use within countries still demonstrate an association with wealth. In one analysis of 45 developing countries, including 22 in sub-Saharan Africa, the richest fifth within each country had contraceptive use rates five times higher than the poorest fifth11. Other research has found women’s autonomy, family structure, child survival, preferred family size, and partner support to be significant factors in some settings, though their relative importance and causal pathways remain debated12. In addition, community-level factors, such as the health service environment and overall approval of contraceptive use, may also influence individual behavior13. At the country-specific level, few studies have examined the differences between rural and urban contraceptive use or other geographic differences. In the limited locations studied, which include Malawi and Uganda, couples living in rural areas had much lower rates of contraceptive use than those in urban areas, potentially related to difficulties in access14-16. Due to the difficulty of collecting data in war-torn, developing countries, few researchers have attempted to assess the relationship between conflict and fertility. One study found a fertility decline in Eritrea related to the border conflict with Ethiopia in 1998-2000 largely due to the fact that fewer men were living with their wives during that period17. In a retrospective study in Ethiopia, times of war and famine were associated with short-term declines in fertility18. An earlier study of fertility in Angola, which used data from a 1996 nationwide survey, found that the probability of giving birth declined as the war intensified and rebounded after the fighting diminished, with women living in regions most affected by the war significantly less likely to desire pregnancy in the next 12 months than those women in less affected areas. This study also showed a significantly lower level of fertility for women living in the capital of Luanda compared to those in other areas19. Additional research by the same authors found no indication that the war exerted any direct or enduring impact on fertility trends in Angola beyond “its generally inhibiting effect on any improvements in social welfare that might otherwise have encouraged some fertility decline”20. Angola offers a compelling case of the many challenges and needs facing family planning in sub-Saharan Africa and in war-torn countries. After gaining independence from Portugal in 1975, the country quickly descended into a protracted civil war that devastated virtually every aspect of society. For the next 27 years, the government fought rebel forces, leaving the country littered with landmines, ruined infrastructure, millions of deaths and injuries, and virtually no professional health care providers. According to the International Monetary Fund, defense spending typically absorbed three times the amount budgeted for all of the social sectors combined during the war. For example, 41% of spending in 1999 went for defense and public order as compared to only 9% for all social services 21. Although several humanitarian organizations worked within the country during the war, an assessment of reproductive health care services provided by those agencies found that even the most basic minimum standards were not being met, including prenatal care and contraceptives22. Angola is now enjoying relative peace, yet it still must recover from years of war, corruption, and neglect. Although Angola has a wealth of natural resources including petroleum and diamonds, the vast majority of the population suffers from extreme poverty. In 2008, Angola overtook Nigeria as Africa's primary oil producer and the country had one of the world’s fastest-growing economies prior to the global recession; however, this economic growth has not impacted the majority of the population’s health and living standards 23,24. The reproductive health (RH) situation in Angola is especially dire. The Reproductive Risk Index, which uses World Health Organization data for ten key RH indicators, ranked Angola as the second worst country in the world 25. At the time of the study, Angolan women had a 1 in 7 lifetime risk of dying of maternal-related causes and more than 1 in 4 children die before age 5 26,27. While child mortality rates have improved in recent years, there has been virtually no change in contraceptive use2. The total fertility rate of 7.2 children per woman is higher than in 1970, and only 6-8% of women aged 15-49 are estimated to use any form of contraception 28,29. Methods This study used a mixed-methods approach, combining responses from a nationwide cross-sectional survey to assess which factors are associated with contraceptive use, with data from qualitative, semi-structured interviews to better understand and illuminate the survey data. Individual characteristics that consistently have been shown to be significant in previous research and theoretical models, such as wealth and educational level, were analyzed using the survey data. In addition, the study focused on the role of location in both the quantitative and qualitative components. For the survey, location, particularly living in urban areas and in the capital region, was hypothesized to be positively associated with use. Because survey data on proximity to, or availability of, services is unavailable, the two location variables used act as a proxy measurement. Semi-structured interviews with internally displaced women and health professionals provided another perspective to explore these issues. This research was approved by the Committee for Protection of Human Subjects at the University of California, Berkeley. Cross-sectional survey UNICEF’s 2002 Multi-Indicator Cluster Survey (MICS) was conducted under the direction of Angola’s National Institute of Statistics (INE). It is the most recent nationwide database available to assess the socioeconomic, demographic, and health situation of Angolan women. Detailed information about the survey design and general results are available elsewhere 30,31. Data were collected between April and October 2001. Clusters of 20 households each were selected using a multi-stage probability sample 30. A total of 7,090 women aged 15-49 years of age were interviewed about issues related to reproductive and maternal health. The analysis for this study used the women’s dataset as the primary source of data, but merged specific demographic and migration data from the other survey components. Data collection for MICS was restricted to the territory that was regarded as secure by the Angolan Government in 2001. The territory covered comprised approximately 65% of the population and was disproportionately limited in rural areas, although data were collected in each of Angola’s 18 provinces. The results can be considered a reasonably accurate representation of the situation in urban settings, but may offer a less representative representation of rural Angola. Note that the MICS was completed prior to the war’s end in 2002. In contrast, the qualitative interviews specifically targeted internally displaced women living near Luanda and were conducted in 2004, two years post-conflict. All statistical analyses were conducted using SPSS for Windows version 11.5. Cases were weighted according to the cluster sampling design as calculated by the original MICS researchers. The sample weights used were the inverse of the relative probabilities of selection and adjusted to account for non-response 32. Logistic regression analysis was used to access the relative contribution to contraceptive use of several potential individual and ecological factors. Spatial maps showing results by province were created using ArcMap 8.3, a geographic information systems software from ESRI (www.esri.com). Key variables from the MICS dataset were mapped in order to visually represent the findings and to explore the results for possible spatial trends or patterns. All data shown on the map were compiled using the same MICS dataset of women aged 15-49. Semi-structured interviews Semi-structured interviews with 12 health professionals and 20 internally displaced womenwere conducted in Angola during June and July 2004. These interviews were used to better understand and illustrate the current RH situation in the country and to help interpret the MICS results in a post-conflict setting. Health professionals were selected based on their involvement in the funding or provision of RH care in Angola. Individuals and organizations working in the field were identified through a review of the literature and through referrals from other respondents. International, governmental, and local agencies were contacted. Interviews were conducted in either Portuguese or English, based on the preference of the interviewee, and covered themes such as perceptions of Angola’s RH situation, existing health and RH services, access to health care, barriers to access, and post-conflict development priorities. Stratified purposeful sampling33 was used to select women from ten neighborhoods across two peri-urban communities, Samba and Viana, near the capital of Luanda. Neighborhoods and communities were selected based on the distinct settlement patterns and areas of origin of the residents. Individual women were selected to represent a range of ages, income levels, and migration patterns. The first author interviewed internally displaced women aged 18-49. Prior to each interview, the purpose of the study, confidentiality, and the right to not participate were discussed. No women refused to participate and informed consent was received from all. One woman was excluded after confirming that she did not sufficiently speak or understand Portuguese. Each interview was conducted in a private location of the respondent’s choice. The interviews explored the women’s particular circumstances leading to migration, their RH histories, social networks, plans after the civil war, and access to health services. All interviews were tape-recorded and then initially transcribed in Portuguese by a professional transcriptionist. Each tape was reviewed and the transcripts edited by the first author to ensure the quality of the transcriptions. All quotes used in this paper were translated by the first author. Interviews first were reviewed to identify persistent themes. From this initial review, two matrices of major themes were developed, one for health professionals and one for internally displaced women, and each interview was again reviewed and coded. Using an iterative process, the interview responses were again reviewed after conducting the survey data analyses to compare the key findings and to verify through the qualitative interviews the survey data’s continued relevance after the end of the war. Results Demographics Two thirds of the 7,090 women aged 15-49 interviewed for MICS lived in urban settings, due to the inability of surveyors to reach many rural areas for safety and logistical reasons. Interviews were conducted, however, in all 18 provinces. Table 1 illustrates the prevalence of some of the extreme hardships and challenges reported by the women surveyed, which are consistent with the qualitative findings. When educational levels and wealth index quintiles are mapped by province, conspicuous differences emerge depending on location (maps not shown). In particular, the provinces of Cabinda and Luanda, which were government strongholds throughout the war and are key petroleum and economic centers, have much higher rates of wealth, of government per capita expenditure on health, and of education. Women living in many of the rural areas and interior provinces are less likely to have access to schooling beyond the primary level or own items such as refrigerators or electricity, which are used as a proxy for wealth. Only 17% of women in the provinces of Luanda and Cabinda have no formal education compared to almost 60% of women in Kuando Kubango and 67% in Malange. Similarly, the majority of the respondents’ households were in the top two wealth quintiles in Luanda and Cabinda whereas 66% of women in Kuando Kubango were in the lowest quintile. Wealth index quintiles are used as a proxy for economic status in the absence of accurate income data and are an aggregate index of assets such as household ownership of a radio or bicycle and a household’s primary floor material[1]. In terms of provincial per capital health services expenditures from 1997-2001, the coastal province of Namibe on the border with Namibia joins Luanda and Cabinda in the top tier, with over $10 per capita spent on health services. In several of the interior provinces, less than $2 was spent per person per year34. Table 1: Demographic characteristics of respondents (n=7090)
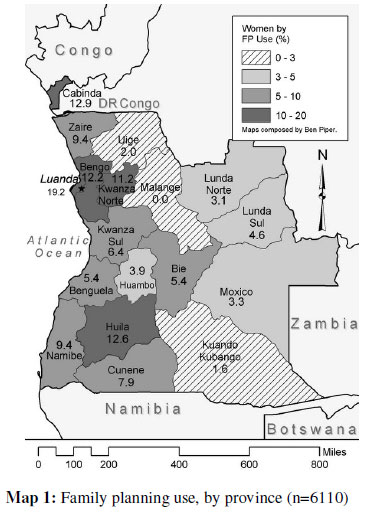
Of the 7,090 women interviewed, 13.2% (n=935) were pregnant and an additional 0.6% (n=45) did not respond to the item regarding pregnancy. In the remaining sample of 6110 non-pregnant women, 5.4% reported using modern contraceptive methods and 2.1% employed traditional methods such as periodic abstinence. Oral contraceptives (2.9%), periodic abstinence (1.7%) and injections (1.3%) were the most common methods reported. Less than one percent (0.5%) of respondents reported using condoms. As expected, the rate of contraceptive use varied substantially by women’s educational level, level of wealth, and area of residence. Parity did not correlate with use. Prior to adjusting for other factors, women’s educational levels were strongly associated with their rates of contraceptive use (p <.001). Of the 2193 respondents with no education, only 2.0% were currently using any method of contraception as opposed to 7.2% of the 3193 women with a primary education and 32.4% of the 139 women who had an 11th grade education or higher. Similarly, dividing the respondents into quintiles of wealth shows a significant increase (p <.001) in use from the poorest (2.0%) to the richest (17.1%), although the differences are relatively modest in the first three quintiles. The respondents comprising the richest quintile were 8.7 times more likely to use contraceptives than the poorest women. Use of family planning services appears to be associated not only with individual characteristics such as educational level and wealth, but also with location. In this sample of women, location may serve as a proxy for access, with contraception simply unavailable in many areas. Women living in urban settings were found to have triple the rate of use compared to those in rural areas (9.4% to 3.0%). Map 1 shows the difference in contraceptive use by province. Table 2: Bivariate correlation of variables (n=6110)
** Correlation is significant at the 0.01 level (2-tailed). * Significant at the 0.05 level (2-tailed) Table 3: Odds ratios of contraceptive use, by variable and model(n=6110)
* Odds ratio significant at p<.01, two-tailed test; ** Odds ratio significant at p,<.001, two-tailed test Table 2 shows the bivariate correlation coefficients of contraceptive use and other variables, weighted according to the sampling framework. As expected, many of these variables have significant correlation between one another. In particular, the wealth index levels are strongly correlated with living in an urban area and level of education. Using this simple bivariate analysis, all of the explanatory variables are significantly correlated with contraceptive use. To assess the relative influence of these factors, hierarchical logistic regression analyses were conducted. The initial model contained individual characteristics of the women which had been found significant in other settings. The two binary age variables of whether a woman was under 20 or over 40 years of age were included, with the age category of 20-40 years selected as the reference category due to the higher levels of contraceptive use among this age group compared to the younger or older groups. For the education variable, women were separated into three categories of no education, primary level, or secondary level. Wealth is measured according to the composite wealth index quintiles. The second and final model added two geographic variables: the binary variables of urban or rural and living in the capital region or any other region. A total of 6110 women aged 15-49 who were not pregnant were included in the analysis. In addition, the same model was tested using a sub-sample of the 3127 non-pregnant women who were married or in unions in case single and divorced women reported different behaviors or were not engaged in sexual activity. Because the results were highly similar when only including married women, with the exception of the “over age 40” variable, only the results for all non-pregnant women are shown here. The final model was also used to test for possible differences in predictors of use for traditional versus modern methods. Table 3 shows the expected odds ratio of current contraceptive use according to the two models. Individual characteristics were first included: age (under 20 years old, over 40 years old), educational level (none, primary, or secondary), and wealth (quintile), followed by two geographic variables (whether the respondent lived in an urban setting, and whether the respondent lived in the capital region). As hypothesized, both individual and community-level factors are associated with women’s contraceptive use. This was consistent when the sample was restricted to women who were married or in unions (not shown). In each model, a woman’s educational level strongly predicts contraceptive use, even after accounting for the other factors. The odds ratio in the final model shows that women with a primary education are 2.44 times more likely to use contraception than those with no education. Similarly, the odds of using contraception increase significantly with each increase in wealth quintile. Age also appears to predict contraceptive use, with teens far less likely to use contraception than the reference group of women aged 20-40. Similarly, the odds ratio for women over 40 was also lower compared to women aged 20-40; however, when only married women were included, over 40 was no longer a significant predictor[2]. After adjusting for the other variables, the odds of use for women living in the capital region was 2.11 times greater than that for women living in other regions, even after adjusting for the higher rates of wealth and education typically found in this region. The difference between women living in urban and rural areas was not significant. However, in a secondary analysis considering specific types of contraception, the use of modern methods was significantly predicted by urban living (odds ratio=1.80, p<01) (data not shown). These survey results can be better understood in conjunction with the data from the qualitative interviews with the health professionals and the internally displaced women. Health professionals Several themes regarding influences and challenges to the use of contraception emerged from the qualitative interviews with health professionals. The most common reasons given for not using contraception in Angola were rural living, young age, cultural beliefs, and power imbalances. Most healthcare providers and donors interviewed noted the lack of basic services available outside of Luanda. One said, “Nobody knows what’s happing in the rural areas.” Another estimated that 60-70% of the health infrastructure was destroyed throughout the country, with the greatest impact outside of the capital. And another noted, “Since the war, the situation has stayed pretty much the same. The government still isn’t planning according to the needs of the people. Rural areas still don’t even get emergency medicine for months at a time.” Most of the health professionals interviewed were concerned about the lack of services for youth and the pervasiveness of teens having children. One respondent estimated that 60% of adolescents were sexually active by age 15 and nearly all teens were sexually active by 18. Another stated that teens start having children young in order to “get a man.” Others pointed to the lack of sex education, inability to negotiate safe sex practices, and lack of youth-friendly services as serious barriers for teens. As one explained, “youth-friendly family planning services” simply didn’t exist in Angola as the health system neither provided for youth nor offered RH services. Cultural beliefs and attitudes were also frequently portrayed as reasons individuals did not use contraception. Four respondents noted that many Angolans want big families. One stated that Angolans believed the country needed more people and that “if we’re bigger, we’re better.” One professional explained, “Children are seen as wealth, but women also see them as maintenance. Men just see them as wealth.” In addition, several believed that women get pregnant when entering into a new relationship to “build obligations” with the man. They explained that, in general, a man wouldn’t take responsibility for the woman or her children from previous relationships until he fathered a child with her. One respondent stated, “Angolan women believe there’s a lack of men, so if someone has a boyfriend, she will do anything to keep the guy, including not using condoms.” Finally, several health professionals commented that many women are not in the position to negotiate the use of contraceptives due to their extremely vulnerable status. As one explained, “Women can’t negotiate anything” as most are in “exchange relationships” where they trade sex for necessities like food in rural areas and “wants” in urban settings. Another pointed to young teenage girls on the streets who were not professional sex workers, but did occasionally engage in sex for survival — making a couple hundred kwanzas (less than 1$US). Internally displaced women A slightly different picture emerged from interviews with internally displaced women. Money was a constant source of concern for nearly all of the women interviewed. Several were worried about the lack of jobs available and explained that without money, they and their children could not attend school or get health care. One woman said, “At times, we don’t have bread in our house…and when the kids are sick, we don’t have money to go to the health post…. They don’t give medicine for nothing.” One of the most frequently reported barriers to health services—including contraceptives—was that payment was required before the provision of any care or treatment. As another respondent explained, “Here we are able to live free and the area is good, but when a person is sick, to go to the hospital you need money. From the time you’re born, you are sick because you can’t get treatment because you don’t have money.” One woman stated, “In this area, in order to go to the hospital to deliver your baby, you have to have money in your hand. If not, the midwives won’t attend to you.” Another echoed this statement saying that if you’re sick, “you must go to the city to receive treatment in the Central hospital. If you don’t have money, you might die.” One woman said she actually went to the hospital and tried to get family planning, but she needed to pay for it in advance and, at that time, she had no money. Because so few services exist locally and many women had to travel long distances for health care, finding and paying for transportation was also a challenge. Several internally displaced women also mentioned the poor infrastructure and services. They discussed this situation both in reference to their former rural communities and in the peri-urban settlements. One woman expressed a common complaint saying, “Here we don’t have a health post or a school. One man built a health post, but it doesn’t have anything inside it or any medicines.” A woman who was forced to leave the province of Moxico noted, “The people in Moxico are suffering a lot; they don’t have schools or hospitals.” Although several women knew about condoms, the women either didn’t know where to purchase them or said they were available only in the city. Contrary to reports from health professionals who believed most Angolans wanted large families, several of the women interviewed felt people shouldn’t have children in such difficult times. One woman said she didn’t want to be pregnant because the conditions were so unfavorable. Another responded that family planning was important and that “you can’t have a child for no reason.” She continued by saying that she regretted having children during times of suffering and wished that people knew how to avoid having children because “tomorrow, as today, they will suffer.” Health professionals and some of the women did agree on other cultural issues. One woman stated that some men could have “ten to twenty women, this would depend on his means,” and that all of these women would have children with the man. She further explained that there were “always a couple [of these women] who have six or seven children. If you survive, then you are valued for having many children.” Another woman was alarmed by young people’s attitudes toward sex and pregnancy. She explained that youth “get together for no reason” and that when they get pregnant, they leave the children “in garbage ditches for other people to pick up.” This woman had adopted a child that she had found abandoned on the streets. In general, most of the women interviewed had at least heard of family planning, but few had ever used it. One exception was a woman who said that after leaving her province, she went to the maternity hospital to get contraception. A few mentioned specific methods, with injections being the most frequently cited. One wanted to use Depo-Provera in the future, though she was unsure of its cost. Another planned to use a modern method to space future births. One woman voiced the comment of many by saying simply, “we don’t know how to avoid getting pregnant.”. Discussion According to the analysis of the nationwide MICS survey, age, education, level of wealth, and location all were associated with contraceptive use. These findings were reinforced by themes that emerged in the qualitative interviews with health providers, and with internally displaced women. Explanatory qualitative findings include the lack of services and infrastructure available outside of Luanda, the difficulty in paying for services, and the unlikelihood of teens using contraception. Although not included in the MICS survey, the interplay between cultural values, gender roles, and contraceptive use also merits further consideration. Many of these findings reflect similar results found in other countries of sub-Saharan Africa 7,8 and the results of this study may have applications in comparable settings in the future. In addition, many of the factors studied show a strong interconnection. For example, women repeatedly stated their desire for their children and themselves to attend school, which suggests that an individual’s access to education may face many of the same barriers as access to contraception, including cost and lack of local services. Even after adjusting for individual characteristics including educational level and wealth, location significantly predicted contraceptive use. Women who live in the capital region, where more goods and services are available and which spends more per capita on health than other regions, appear to take advantage of what is offered. The differences between contraceptive use in rural and urban areas were only significant for modern methods, after adjusting for other factors. This is likely due to the strong correlation between rural versus urban living and the other variables, such as wealth. In addition, most rural area surveys were conducted in the capital region, which is likely to have different services available than those found in the rural areas of other regions. Therefore, more robust rural/urban differences might be found if other rural areas were surveyed more comprehensively. In any case, additional research is needed to determine the most efficient way of supplying contraceptives to rural areas and other regions currently lacking access. The especially low level of contraceptive use among adolescents requires careful consideration. This finding might be explained by adolescents’ sexual vulnerability or the lack of services or information targeting youth, possibly combined with negative attitudes of service providers toward teens who do seek contraception. In Angola, a third of women have already had at least one child by age 18 30. The finding that women in the highest wealth index quintile are nearly nine times more likely to use contraception has several possible explanations. Because the wealth variable was an aggregate index of assets, including having electricity, radio, television, car, or bicycle, this variable may act as a proxy for other important factors including access to information and transportation. However, it also may reflect the common concern of the internally displaced women interviewed who repeatedly remarked that they could not pay for health services. Other research suggests that most people will not pay more than 1% of their disposable income for condoms or hormonal methods 35. For many Angolans, this estimate may put the cost of contraceptives beyond their means without subsidized pricing or an increase in income. Cultural issues, particularly the perceived desire for a large family, were not assessed in the MICS survey and showed mixed results from the qualitative interviews. Unlike many of the health professionals who believed women wanted to have many children, several of the internally displaced women discussed the importance of carefully considering the feasibility of caring for children during difficult times. The concept of power imbalances, which several health professionals mentioned, also was not addressed in MICS. Most of the displaced women interviewed said that they and their husbands jointly made important decisions. However, several of the women did acknowledge domestic violence within their communities, and few had ever discussed issues such as desired family size or family planning with their partners. This suggests that not all women have the ability to negotiate contraceptive use. More research is needed to better understand the role that cultural norms and values, particularly desired family size and power imbalances, plays with contraceptive use. This research is especially needed in conflict and post-conflict settings where gender imbalances and changing roles may complicate adhering to traditional norms36. This research had several potential limitations. First, the MICS survey estimates were not fully representative of Angola as a whole because data collection was restricted to the territory that was regarded as secure by the Angolan Government in 2001, although surveys were administered in each province. For the qualitative interviews, only internally displaced women ages 15-49 living near Luanda were interviewed. Therefore, the results of both the quantitative survey and the qualitative interviews must be generalized with caution to other displaced populations or to individuals living in different areas. In addition, the differences between the samples used for the quantitative and qualitative studies, as well as the different timeframes of data collection, might limit direct interpretations and comparisons of their results. Nevertheless, similarities in findings across the these two studies provide confirmatory evidence of validity (triangulation), and are useful in highlighting important issues that were present both during and after the end of the war. Note that some of the disparity in the wealth index quintiles may be partially accounted for by the choice of assets included in the index and the exclusion of other possible indicators of wealth, especially ownership or land and livestock, which may be more common in rural areas. Finally, some potentially important predictive factors such as family structure and religion were not included in the logistic regression models and might offer additional insight. The findings of this study point to several potential avenues for increasing contraceptive use: improve the distribution of services to rural areas and areas outside the capital region, develop youth-friendly programs, reduce the price of contraceptives for poor individuals through cost subsidization, and increase access to education. Given the poor infrastructure in most of Angola, consideration should be given to supporting suppliers of contraception outside of health posts and hospitals, such as street vendors and pharmacies. With the end of the war, record-breaking profits from the petroleum industry, and the relative stability of peace, the Angolan government is in the position to address many of these issues and consequently, to improve women’s reproductive health. Notes [1] MICS attempts to derive a measure of economic status by household when there is an absence of income or consumption data through a series of questions including: main material of floor, source of drinking water, toilet facility, main cooking fuel, and whether household has electricity, television, radio, refrigerator, motorcycle, bicycle, or car. Additional details about the methodology are available on the MICS website at http://www.childinfo.org/MICS2/ finques/gj00106a.htm. [2]When tested using only women married or in unions (n=3127), the variable over 40 was not statistically significant. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11053m1.jpg] [rh11053f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}