 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 4, Dec, 2011, pp. 98-105 Original Research Article Identification and understanding of pre-term birth at Kintampo Municipal Hospital: A qualitative cross-sectional study Identification et compréhension de la naissance avant terme dans l’Hôpital Municipal à Kintampo : Etude transversale qualitative Joanna Jean Parga1*, Emilia Asuquo Udofia2 and Damien Punguyire3 1Pediatric Residency Program, The Children’s
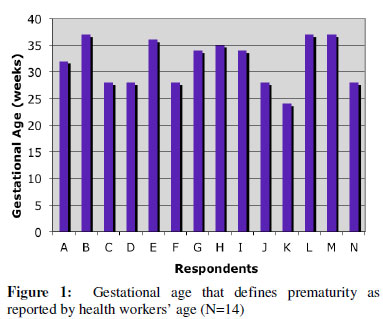
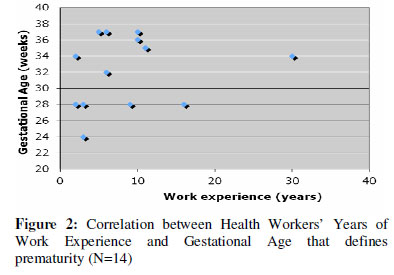
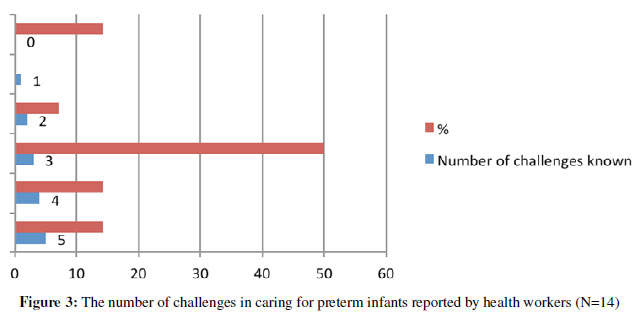
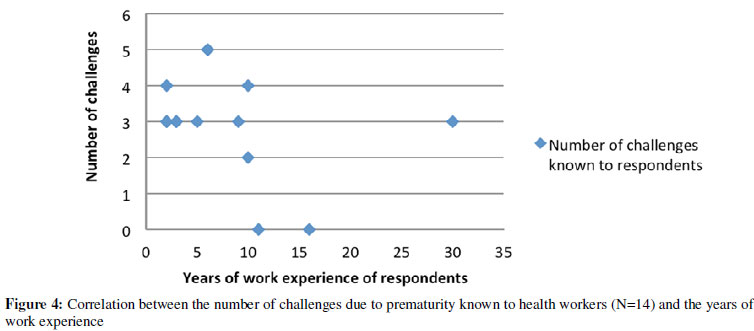
Hospital of Los Angeles, Los Angeles, California, USA; Code Number: rh11056 Abstract Up to 42% of nearly 10 million under five deaths occur in neonates with prematurity being a principal cause. This paper presents the outcome of a cross sectional qualitative study conducted among 14 hospital staff engaged in infant care in Kintampo, Ghana. Confidential interviews were used to evaluate their knowledge and practice of preterm care. Critical steps in caring for normal and preterm infants were ranked as adequate, satisfactory or inadequate if 75% or more, 50% to 74%, or less than 50% of the health workers completed them respectively. For term infants, adequate care was provided in terms of cleaning and wrapping, weighing, and initiating early feeds. Knowledge and practice were inadequate in relation to preterm care. Educational interventions emphasizing preterm care are recommended as an essential package for rural health workers. A newborn assessment tool was designed to address the gap in data collection identified during the study (Afr J Reprod Health 2011; 15[4]: 98-105). Résumé Plus de dix million enfants âgés de moins de cinq ans meurent chaque année. Jusqu’à 42% de ces décès-là sont des nouveau-nés et la cause principale du décès des nouveau-nés est la prématurité. Un million enfants nés avant terme meurent chaque année, ce qui est responsable de 27% des décès des nouveau-nés. L’étude avait comme objectif d’évaluer la connaissance du personnel de santé concernant la prématurité et de créer un simple instrument pour le recueil de données pour évaluer le nouveau-né à l’hôpital municipal à Kintampo, Région Brong Ahafo, Ghana. Nous avons mené une étude qualitative transversale au niveau d’une école secondaire dans un milieu rural. Il s’agissait des interviews confidentielles recueillies auprès de 14 membres du personnel soignant directement engagés dans le soin des enfants dans le centre gynécologique-obstétrique. Toutes les interviews ont été recueillies en anglais après avoir obtenu le consentement. Les démarches critiques concernant le soin des enfants normaux et les enfants nés avant terme ont été catégorisées comme adéquates, satisfaisantes ou inadéquates si 75% ou plus, 50% jusqu’à 74% ou moins de 50% du personnel de santé ont les ont rempli respectivement. Nous avons formulé une feuille d’évaluation pour les nouveau-nés afin de collecter des données pour chaque enfant. Pour les enfants nés à terme, on assure un soin adéquat en ce qui concerne le nettoyage et l’emballage, mesurant le poids et l’initiation à la nourriture précoce> Le soin était inadéquat dans toutes les catégories de soin avant terme. On a signalé un soin adéquat dans l’utilisation de l’étuve à incubation et une fréquence augmenté de la nourriture. Le manque de connaissance à l’égard de la prématurité a beaucoup engendré des soins inadéquats pour les enfants nés avant terme. Nous préconisons des interventions éducatives pour améliorer les soins des enfants dans les milieux ruraux, tout en mettant l’accent sur le soin avant terme(Afr J Reprod Health 2011; 15[4]:98-105). Keywords: Prematurity, preterm, neonatal, Ghana, Kintampo Introduction Worldwide approximately four million infants will die before one month of life. They are part of the nearly ten million children who die before reaching age five; accounting for 38% of childhood mortalities1. While under-five mortality rates in sub-Saharan Africa have declined by 22% since 1990, the progress in addressing the mortality rates of newborns has been slow2. These deaths primarily occur in low and medium income countries, where access to health care is difficult, and data collection on newborn infants is minimal or non-existent. Other reasons for the predominance of neonatal death in low-income countries include; lack of systemic estimates for the prevalence of preterm births, lack of accurate estimation of gestational age, and lack of simple care and quality health services for mothers and newborns3. Complications of preterm birth are the single biggest risk factor for neonatal death and increased morbidity. Prematurity accounts for up to 27% of the nearly four million neonatal deaths annually, from both direct and indirect causes. The challenges a premature infant faces include, but are not limited to respiratory distress (respiratory distress syndrome, brochopul-monary dysplasia, apnea of prematurity) in 93% of premature newborns, late onset sepsis (sepsis occurring at 3 days of life) in 36% of premature newborns, intraventricular hemorrhage (IVH) in 16% of premature newborns, and necrotizing enterocolitis (NEC) in 11% of premature newborns3,4. To explore the risks associated with prematurity, it is necessary to define preterm birth. Preterm birth includes any infant born before 37 weeks of gestation and has gradations of moderately (33-36 weeks), very (28-32 weeks) and extremely (less than 28 weeks) preterm. These categories are important because survival rates increase with increasing gestation. A study of newborn infants in Nigeria found that for a gestational age of 31 weeks the survival rate was roughly 53.3%. By 35 weeks there was a substantial increase in survival to 96.6%5. Along with gestational age, the weight of a newborn is often considered an important tool in determining prematurity. An infant is considered low birth weighing less than 2500g, and very low birth weight weighing less than 1500g. However, low birth weight is not necessarily a product of prematurity. Therefore gestational age is a better indicator of preterm birth4. Despite its influence on neonatal mortality, preterm birth lacks visibility and political backing in low-income countries. Issues such as lack of human resources, poor funding, and improper facilities make neonatal care difficult6. In addition to lacking the resources to provide appropriate care, places with the highest risk of preterm death currently have the smallest amount of recorded information available on it. This presents a large problem for neonatal care, because the neonatal mortality rate depends on the place of delivery. It is related to the supplies available and the expertise of the staff. Thus each obstetric unit should establish their own gestational age-specific mortality rates contingent on the care they provide5. This can only be done if the quantity and quality of information on neonates can be improved by seizing opportunities to add to ongoing hospital data collection3. Kintampo Municipal Hospital is among the many rural district hospitals that lack accurate data collection and assessment of newborns. Steps need to be taken at Kintampo Municipal Hospital to raise awareness about both the prevalence and risks of prematurity. Promoting documentation of infant health at birth would help do this. An assessment of healthcare workers’ understanding of preterm birth, and clinical skills surrounding prematurity would also aid in the creation of targeted interventions for newborns, thereby improving care. Methods Kintampo is located in the geographical center of Ghana in the Brong Ahafo Region. It lies in the rainforest-savanna transitional zone. While formally one district, Kintampo has broken into a North and a South district with the hospital in the North district. The population in 2008 was 130,972 individuals with females and males comprising 50.7% and 49.3% respectively. Kintampo is a predominantly Christian community where the major occupation is farming. While the official language is English, the main language spoken in the region is Twi. Kintampo Municipal hospital is a referral hospital that serves all sub-municipal health facilities in the area. It is affiliated with the Kintampo Health Research Center (KHRC), Kintampo Municipal Health Directorate, and the Kintampo Rural Health Training School (KRHTS). The hospital strives to be a primary care center that meets generally acceptable standards of care, combined with clinical research and training. In 2010, 1,337 expectant mothers attended the antenatal clinic and 832 deliveries were reported. There were 39 stillbirths, but the number of preterm infants was not recorded7. Permission to conduct the study was obtained from the Kintampo Municipal Health Directorate and the Kintampo Municipal Hospital Administration. A qualitative cross-sectional study was conducted at Kintampo Municipal Hospital to evaluate the care provided for preterm infants. Confidential interviews were held with health care workers at the hospital. A fourth year medical undergraduate as a part of the General Electric/National Medical Fellowships program for foreign students performed the interviews while in Ghana. All interviews were conducted in English after obtaining consent. The study sample comprised of all health staff at the hospital who were directly involved with neonatal care at the maternity unit. Full-time midwives from the maternity ward, the antenatal clinic and the Reproductive and Child Welfare Clinic, the owner of Glory Prince of Peace Maternity Home/Clinic (a past employee of Kintampo Municipal Hospital) and one physician were interviewed after consent was sought and obtained. Workers who were not directly involved in infant care, or who did not have a permanent position as hospital were excluded from the study. Participants were asked their age and designation, years of work experience, and various questions on both term and preterm infant care (Appendix 1). Critical steps in caring for infants were based on; medical literature, what could be sustained given the setting, performed easily with little training, and has a significant impact on neonatal survival. For term infants, crucial steps were; cleaning and wrapping the infant, measuring the head circumference, chest circumference and weight, recording APGAR scores, a general physical examination of the infant, administration of vitamin K and initiating breastfeeding early. For premature infants, crucial steps were incubator care, increased frequency of feeds, preparation for resuscitation, minimizing exposure (no bathing) and subsequent referral to the Reproductive and Child Welfare Clinic. Responses were reported as “yes” if they would complete, or “no” if they would not complete the selected steps in infant care. An arbitrary scale was created to determine where improvements in care would be required. If > 75% of respondents said “yes” they completed that step in care, then the care provided was considered adequate and no group intervention was recommended. Those observed to be deficient in completing any critical step would be guided to do so individually. If 50-74% of respondents had completed that step in care, then the care was considered satisfactory however an intervention was recommended such as on-site training for a small group. If < 50% of the respondents completed that step in care, the care was considered inadequate and major intervention was recommended such as re-training in batches for all health workers involved in care. The interviews took place between the hours of 8am and 4pm on week days. The study was conducted over a three-week period at the Kintampo Municipal Hospital from March 22nd to April 14th 2011. Results were analyzed with Excel version 2008. Proportions of variables were presented as frequency tables, graphs, pie and bar charts. Neonatal Assessment Sheet In order to encourage data collection on all neonates, and ultimately the prevalence and risks of prematurity at Kintampo Municipal Hospital, a Neonatal Assessment Sheet was developed. It requires little or no clinical skill to complete and was created to record basic data on all newborns. Previously no data was collected on neonates. The document went through several revisions. Initially it included the Dubowitz-Ballard scale to assess postnatal gestational age and compare to the gestational age listed in the mother’s chart - derived from Last Menstrual Period (LMP) and Ultrasound. The Dubowitz-Ballard exam is a relatively better predictor of gestational age than the LMP, because LMP is uncertain or unknown for 20% of pregnant women in low-income countries8. While ultrasound in the 1st or early 2nd trimester is the gold standard of pregnancy dating, seldom in rural Africa is the scan done in the correct time period9. Furthermore, at Kintampo Municipal Hospital it was common for a mother to deliver at the hospital with no prenatal care or dating done. It was therefore hypothesized that the Dubowitz-Ballard scale would offer a reliable determination of gestational age and prematurity. However, the Dubowitz is a relatively complex technique that requires considerable clinical experience and training to detect slight changes in neonatal posture and muscle tone. This limits its applicability in the field9,10. Thus, the Neonatal Assessment sheet had to be simplified so that any midwife in the maternity ward, without instruction or training, could fill it out (Appendix 2). Since the neonatal assessment tool was initiated at the time of the study, it was not evaluated Results Background characteristics The respondents comprised of 13 females and 1 male. The ages ranged from 25 to 59 years with an average of 43 years +/- 13 years. The median age was 49 years. The average working experience was 9 years +/- 6 years. The median number of years of experience was 6 years with a range from 2 to 30 years. Defining prematurity Each respondent was asked at what gestational age an infant could be considered premature. The responses provided are depicted in Figure 1. The average estimated gestational age for prematurity was 32 weeks +/- 4.4 weeks, with a median of 33 weeks. There was no correlation between the years of work experience, and knowledge of the definition of prematurity. The results are shown in the Figure 2. Standard of care for term infants The result for standard of care for term infants is shown in Table 1.Adequate care was provided for the neonates in terms of cleaning and wrapping (93%), weighing (93%), and encouraging early breast-feeding (79%). Other critical care components were considered inadequate. Very few respondents obtained the head and chest circumference of the neonates (36% and 21% respectively). The APGAR score was either not mentioned as a standard of care, or not performed correctly, as only 43% of respondents would perform it. Physical examination was not routinely performed on newborn infants (29%). Only 14% of respondents considered vitamin K as standard of care for all newborns. Standard of care for preterm infants The standard of care for premature infants is shown in Table 2.Adequate care was not provided in any category of preterm care. Satisfactory care was provided in the areas of incubator usage (57%) and increased frequency of breast-feeding (57%). Only 43% of premature patients were referred to Reproductive and Child welfare clinic. Fourteen per cent of respondents prepared for resuscitation as part of routine care of premature infants. One fifth of those interviewed (21%) reported the need to decrease exposure of infants by bathing them less frequently. Challenges in preterm care Each health workers was expected to be able to name at least 5 challenges to the survival of preterm infants. However, the average number of challenges respondents could name was 3 +/- 1.5, with a median of 3. Challenges to premature life that were mentioned by respondents were respiratory distress, hypothermia, hypo- or hyperglycemia, immature organ development, infection, difficulty feeding and difficulty growing. Fourteen per cent of those interviewed could name 5 challenges. Figure 3 outlines the number of challenges each respondent could name. Figure 4 indicates no correlation between the years of working experience and the ability to mention 5 challenges. Table 1: Components of standard neonatal care reported by health workers (N = 14)
* If the respondent could not name the components of the APGAR scale they were recorded as not having completed it Table 2: Components of preterm care reported by health workers (N = 14)
Views on infant life Respondents related their views of infant life. The importance and significance of infant life varied greatly depending on what region and tribe respondents were from. Overall, many respondents reported that infants were “not like adults” and that an “infants death is not as painful as an adult death.” Culturally, it was said that when a newborn dies he or she has “gone back to God” and that the family would say, “Let’s give it to God”. Being valued differently than adult life, traditionally infants will not have funerals. Ten out of fourteen respondents believed that if a funeral were held for an infant, another baby in the family would die. Even the act of mourning a dead infant was viewed as an act that could make another child suffer and die. This was because the mother would not be giving the living children the time and attention they need to survive, if she “wastes” her time on a dead infant. Thus mothers are said to “not put too much time” into mourning newborns. One respondent reported that many simply bury the body of a newborn in a box in their backyard. However, respondents mentioned that mothers do experience “psychological trauma from losing a child.” Onerespondent said it was “a midwife’s job to educate and have compassion,” because it is “very painful for the mother.” It was also recommended that mothers “should go and deliver again” because “mourning too much can disturb you,” and the distraction of trying for another child was thought to ease a mother’s pain. Discussion Kintampo Municipal Hospital exists in a resource limited setting. There are shortages of medical supplies and motivated hospital staff to care for patients. The maternity ward is an especially difficult place to provide quality health care. Taking care of two patients at once - both mother and infant - overstretches the midwives. With maternal mortality being high and scarce human health resources, infants are neglected. This paper aimed to assess the knowledge of health workers in relation to infant care, and to recommend cost-effective and sustainable interventions to improve infant care. While increased technology and resources are tied to decreasing neonatal mortality, initiating simple interventions in an area where neonatal care is under practiced could greatly influence care. No category of care was deemed adequate for preterm infants. This was due to the fact that premature infants are not recognized. The average estimated gestation age for prematurity identified by the respondents was 33 weeks’ gestation, while the threshold for defining a preterm birth is below 37 weeks’ gestation. It was expected that each respondent should be able to name at least 5 challenges that premature infants face, only 2 could name that many. The underestimation of preterm birth and lack of awareness of challenges to preterm infants are reflected in the inadequate care for premature infants at the hospital. However, it is not just preterm birth that suffers from a low standard of care. For all births at Kintampo Municipal Hospital, there is little data collected on neonatal assessments and care. Measurements for head circumference and chest circumference were not performed routinely. There were many reasons why basic anthropomorphic data was not taken: difficulty obtaining the data when working alone, the measuring tape being missing, the measuring tape being torn, dealing with two patients [mother and child] and the mother’s well-being taking precedent over the infants. In addition The APGAR score was either not performed, or not accurately assessed in the majority of births. Even simple and cheap interventions were not carried out. For example, only 14% of respondents considered the administration of vitamin K as standard of care for all newborns. Vitamin K has been identified as a prophylactic treatment for newborns to prevent abnormalities in the coagulation cascade. It would be particularly helpful in premature infants to decrease the risk of intraventricular hemorrhage11. This therapy used to be provided at Kintampo Municipal Hospital, but the vitamin K used caused neonatal jaundice and it was discontinued. Educational interventions are needed to stress the importance of dealing with neonates and their status as patients in the hospital. Aside from education, providing basic supplies like vitamins could have a significant impact on infant care. Even if targeted educational programs were started by Kintampo Municipal Hospital, the way in which infant care is viewed and implemented requires standardization at a national level. Ghana Health Services, under the auspices of the Ministry of Health, can play a lead role in redefining infant care. As a policy, hospitals should have their own audits for neonatal care that will involve the collation of data using a formalized collection tool12. For example, a countrywide Neonatal Assessment Sheet, like the one in this study, should be a required document for neonates at birth. Municipal or District Health Directorates should hold each health facility accountable for accurately tracking data, given that the minimum resources to do so have been provided. This will facilitate trend recognition in infant morbidity and mortality, and help to offer targeted recommendations for improvements in care. The Ghana Health Services can also liaise with the National Health Insurance to provide insurance earlier for newborns so they are recognized as distinct patients with their own right to healthcare. Aside from creating a national data collection system for neonates, the government should also review and revise the current training program for nurses and midwives to include courses in neonatal care. There is a need to retrain healthcare workers who are involved infant care. Making the small interventions outlined in this paper could mean huge improvements in neonatal care. However, one cannot underestimate the cultural barriers to achieving this. A long-standing history of neonatal deaths in rural areas, coupled with the ravages of poverty, make infant life transient. Parents are familiar with the possibility of infant death and would rather invest in more children than improve the quality care for their existing young. By improving awareness and care for infants, attitudes toward infant life can begin to shift. Parents can start to expect that their infants will live, and mothers can be spared the pain of losing their newborns. The above study has its limitations. Constrained by time and budgetary provisions, it was conducted at one health facility on a sample which is too small to make conclusions. Therefore a larger multi-centre study is recommended to address this limitation. It also represents the health worker perspective to neonatal care and does not involve the community. However, its strength lies in the fact that a critical gap in measuring an outcome (neonatal care) was identified and an instrument created to meet the need for documentation. In future, it will be useful to evaluate the instrument when it is formally adapted. Conclusion An evaluation of newborn care at the Kintampo Municipal Hospital in Brong Ahafo Region, Ghana based on staff interviews revealed the absence of data on neonatal care, as well as gaps in health workers’ knowledge and practice of preterm care. For term infants, adequate care was provided in terms of cleaning and wrapping, weighing, and initiating early feeds. Neonatal care appears to be specific where it is practiced and related to the availability of resources. Ghana is uniquely positioned to use this opportunity to assist rural areas which are worst hit to build a neonatal care system from very minimal resources. With adequate data collection and documentation of infant care, a system for neonatal health can be built that is tailor-made for Ghana’s population and needs. They can learn from the mistakes of developed countries, and adapt to provide the best care possible in a resource-limited setting. By creating standardized guidelines for neonatal care, Ghana will be that much closer to achieving the Millennium Development Goals, especially Millennium Development Goal 4 which aims to reduce child mortality. In turn, the precious lives of Ghanaian children will be preserved for a promising future. Acknowledgments This paper would not have been possible without the generous support of the General Electric/National Medical Fellowships program. Within the program, special thanks go to Dr. Esther Dyer and Melissa Brito. My mentor on site, Dr. Damien Punguyire, was instrumental in providing support on the ground for the study. Dr. Emilia Udofia was responsible for helping develop the methods and editing the paper for publication. She was also a source of inspiration and a wealth of wonderful ideas. Dr. Stephanie Staples, Dr. Maria Berenice Nava and Dr. Anne-Lise Paisible are acknowledged for their support while traveling in Ghana. Appendix 1 Neonatal Care Survey - Interview for Healthcare Providers -- Kintampo Municipal Hospital Hello. My name is Joanna Parga and I am a visiting fourth year medical student from the United States. I would like to invite you to take this confidential survey about your views on Neonatal Care here at Kintampo Municipal Hospital. The responses will be used to help improve infant care at the hospital.
Thank you for your participation! Appendix 2 Newborn Assessment Sheet Date of Birth: 44444 Time of Birth: 4444 Mother’s Hospital ID Number: 44444 Estimated Gestational Age in Maternal Folder (weeks): 44 Is the infant premature (less than 37 weeks - circle one): ------------------------------------------ How preterm is the infant (circle one): --------------------------- Moderate (33-36 weeks) Very (28-32 weeks) Extremely (less than 28 weeks) APGAR Score: 1 min 44444 5 min 44444
Need for neonatal resuscitation (circle 1): Yes No If yes, describe the resuscitation: 44444444 Did the infant require placement in an incubator (circle one): --------------------------------------------------------------------------- Physical Exam:
Weight (kg): 4444 Length (cm): 44444 Head circumference (cm): 44444 Chest circumference (cm): 44444 General (posture, activity, gross abnormality, color): 444 Ability to Suck (circle one): Strong Weak Absent Other Comments: References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11056f2.jpg] [rh11056f1.jpg] [rh11056f4.jpg] [rh11056f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}