 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 15, No. 4, Dec, 2011, pp. 109-119 Original Research Article Sexual and reproductive health education among dressmakers and hairdressers in the Assin South district of Ghana Education sexuelle et de santé de la reproduction chez les couturières et les coiffeuses dans le district d’Assin South du Ghana. Samuel A Owusu1*, Emmanuel J Blankson2 and Albert M Abane2 1Directorate of
Organisational Development and Consultancy, University of Cape Coast, Ghana; Code Number: rh11058 Abstract This was an exploratory study on how dressmakers and hairdressers in the Assin South District of Ghana receive education on sexual and reproductive health. The respondents comprised mainly of full time female dressmakers and hairdressers as well as their apprentices (aged between 15 and 35 years, had attained basic education and were never married). Although some of the respondents were able to mention some sexual and reproductive health education programmes such as ‘Mmaa Nkomo’, most of them could not recall the recent topic discussed. Respondent’s major sources of information on sexual and reproductive health were friends, mass media, health professionals and parents. A significant proportion of them did not consider sexual and reproductive health issues as a priority for human development and thus paid little or no attention its educational programmes.It was recommended that dressmaking and hairdressing supervisors should be regularly trained in sexual and reproductive health issues to enable them educate their apprentices (Afr J Reprod Health 2011; 15[4]:109-119). Résumé Il s’agissait d’une étude exploratoire sur la façon dont les couturières et les coiffeuses dans le district d’Assin South du Ghana au Ghana reçoivent l’éducation sexuelle et de santé de la reproduction. Parmi les interviewées, il y avait des couturières et des coiffeuses â plein temps aussi bien que leurs apprenties. Nous avons choisi les couturières et les coiffeuses parce qu’elles sont les objets des programmes éducatifs financés par les ONG et les états sur la santé sexuelle et de la reproduction. D’ailleurs, les magasins des couturières sont les endroits où les jeunes gens se rassemblent pour discuter les problèmes relatifs â la santé sexuelle et de la reproduction au Ghana. Du point de vue démographique, la plupart des interviewées étaient des femelles agées d’entre 15 et 35 ans, qui ont acquis une éducation fondamentale et n’étaient jamais marées. Celles qui avaient plus de 35 ans constitueraient un peu moins d’un pourcent. Bien que quelques interviewées aient pu mentionner quelques programmes d’éducation sexuelle et de la reproduction tels « Mmaa Nkomo », la plupart ne pouvaient pas se rappeler le dernier sujet discuté. On a remarqué que la source majeure d’information sur la santé sexuelle et de la reproduction chez les interviewées étaient des amis, les médias (la presse écrite non comprise), les professionnels de santé et des parents. Une proportion importante des interviewées n’ont pas considéré que les problèmes de santé sexuelle et de la reproduction est une priorité pour le développement humain et ont donc accordé peu d’attention ou n’ont pas accordé l’attention du tout aux programmes éducatifs sur la santé sexuelle et de la reproduction. On a proposé que les surveillantes des couturières et des coiffeuses soient régulièrement formées dans le domaine des problèmes de santé sexuelle et de la reproduction pour permettre de former leurs apprenties (Afr J Reprod Health 2011; 15[4]: 109-119). Keywords: Reproductive health, Sexual health, Education, Tailors, Hairdressers, Ghana Introduction The 1994 International Conference on Population and Development (ICPD) held in Cairo, Egypt, is widely regarded as the turning point for a number of countries inincorporating population issues into their development programmes1. Ghana had earlier adopted a population policy in 1969 with the intention of ensuring that population issues were integrated into all aspects of national development planning and implementation process. Analysts opine that although the policy failed to effect the needed changes due to lack of political commitment, the policy raised the awareness of the people, especially urban residents, to family planning issues1-3. In 1994, Ghana adopted a revised population policy which made provision for the inclusion of population and family life education (PFLE) to the people at formal and informal educational settings to prepare them to become responsible citizens2. The policy also proposed the development of population information, education, communication and motivation (PIEC&M) materials in the various local languages in Ghana to meet the needs of local people and also to complement the activities of radio, television and newspaper discussions on sexual and reproductive health. Reproductive health seeks to ensure that people are able to have a responsible, satisfying and safe sex life as well as having the capability to reproduce and the freedom to decide if, when and how often to do so4 . This also includes having appropriate health-care services that will enable women to go through pregnancy and childbirth safely4-5. Currently, sexual and reproductive health education issues form an integral part of the curriculum at all levels of education in Ghana5-8. For instance, students at the basic level are taught sexual and reproductive health issues such as sexually transmitted infections (STIs) including human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS), teenage pregnancy, unsafe abortions and abstinence from sexually related activities. Furthermore, a number of educational programmes have been and continue to be implemented in Ghana to sensitise the general public on the need to adopt appropriate sexual and reproductive health behaviours. The Ghana Social Marketing Foundation has undertaken a number of projects such as ‘Stop AIDS Love Life’, ‘Things we do for Love’ and ‘Life Choices’. The latter was aimed at boosting the use of modern family planning methods in urban, peri-urban and rural areas through the collaborative efforts of opinion leaders9. According to Bankole, (1994), the mass media can be a powerful tool not only for awareness creation about new technology but also for stimulating people’s desires for more information on sexual and reproductive health as well as facilitating their efforts to apply the information to their own behaviour10. Programmes such as “Wo ba ada anaa”, “odo ahomaso”, “aware so” and Happier Healthier Home (He Ha Ho) are few examples of sexual and reproductive health education programmes aired on radio in Ghana. Programmes such “Mmaa Nkomo”, ”You and your Health” and “Complete Woman” showed on some television networks in Ghana provide education on sexual and reproductive health to the citizenry. Personnel from the Ghana Health Service (GHS), on the other hand, regularly undertake outreach programmes on sexual and reproductive health in addition to the routine services they provide to patients at the various health facilities. Resource persons for such programmes include religious leaders, health care providers, legal practitioners, gender activist and traditional rulers. Undoubtedly, the provision of sexual and reproductive health education in Ghana has expanded both in content and coverage during the last two decades. It is therefore expected that Ghanaians will continue to receive education on sexual and reproductive health from these resource persons and outlets such as schools, churches, health facilities, mass media, durbars and workplaces. A major proportion of Ghana’s population are engaged in informal economic activities. This economy covers a variety of activities such as agriculture, fishing and fish processing, wholesale and retail food vending, chemical/drug sale, refuse collection, carpentry, portage, hairdressing and dressmaking11-13. A dressmaker is a person who makes women’s cloths, especially as a job while a hairdresser is a person whose job is to cut, wash and shape hair while a tailor is a person whose job is to make men clothes14. However, in this study, dressmaking and hairdressing vocations were generically used as comprising all persons whose vocation is to sew men and women clothes as well as cutting, washing, plaiting or shaping peoples hair in exchange for money. The informal economy had been largely regarded as unnoticed, unprotected, mostly ignored, rarely supported, unregulated, sometimes unprofitable and confined to marginal activities11-12. Some operators, especially apprentices, in the informal economy have little or no financial sustenance and will therefore find it difficult to negotiate for safer sex with their sexual partners. This situation also makes them vulnerable to unhealthy sexual and reproductive practices that largely expose them to gender-based violence, Sexually Transmitted Diseases (STDs) and unsafe abortions. Some dressmakers and hairdressers are targets of the state and NGO sponsored programmes on sexual and reproductive health education. In Ghana, some dressmakers are regarded as “informal counsellors” on sexual and reproductive health and non-traditional distributors of condoms 9, 15-16. Lastly, dressmaking shops and hairdressing salons are sometimes the venues where young people congregate to discuss sexual and reproductive health issues15. According to the Guardian News (2006), in Zimbabwe, more than 1,000 hairdressers have been trained to give advice to their clients about sexual matters and to sell male and female condoms. The salons in the country have been identified as favourable environments where women could freely communicate about HIV-related issues. The hairdressers offer sexual and reproductive health counselling as well as distribute female condoms to their clients as part of an innovative programme to reduce HIV infection through increased Voluntary Counselling and Testing (VCT) and the practice of safer sex17. In Kenya, a community-based group, Teenage Mothers and Girls Association of Kenya (TEMAK) assists some female dropouts to learn dressmaking, hairdressing, typing or computer literacy. The apprenticeship programme is interspersed with sexual and reproductive health information and education, counselling, testing for HIV, treatment for skin infections, free distribution of condoms and access to clinical services through referrals18. Togo also offers useful insights into how dressmakers have become targets of structured programmes on sexual and reproductive health. For instance, dressmakers have been trained as peer educators to sensitise the youth on HIV/AIDS and its related problems19. As at 1997, Assih reported that about 881 supervisors and apprentices had benefited from the programme. The sewing shops became active outlets for the sale and distribution of condoms. These unique features about dressmakers and hairdressers informed the decision to use the two vocational groups for this study. Studies on how sexual and reproductive health education programmes are delivered to dressmakers and hairdressers in the Assin South District of Ghana had not been comprehensively carried out. This study therefore explored how dressmakers and hairdressers in the Assin South receive education on sexual and reproductive health. The varying religious, economic and social context within which dressmakers and hairdressers operate may influence their knowledge and attitude to sexual and reproductive health issues. For example, a person’s religious affiliation sometimes determines the choice of sexual partner and reproductive health care seeking behaviour. Social connectedness to family, adults and peers has also been identified to have some influence on communication about sex-related matters 20-21. Sexual and reproductive problems such as higher maternal mortality, lower contraceptive prevalence rate and poor family planning practices are not peculiar to dressmakers and hairdressers. However, it appears that not much attention has been given to providing sustained or structured educative programmes on sexual and reproductive health for people who earn their livelihood from informal economic activities. It therefore becomes imperative on all individuals or groups who can affect or be affected by the sexual and reproductive activities of people who are directly involved in informal economic activities to act in concert to ensure that accurate information is made available to enable them make informed choices on their sexuality. The services of the public and private health practitioners, educational institutions, Civil Society Organisations (CSOs), faith-based organisations, the media, researchers and Non-Governmental Organisations (NGOs) would be beneficial in this direction. Perhaps, it is in this light that organisations such as the Planned Parenthood Association of Ghana (PPAG), an NGO affiliated to the International Planned Parenthood Federation (IPPF) as well as the Ghana Social Marketing Foundation (GSMF) have played frontline roles in equipping the population with information and materials to enable them exercise their basic rights to decide freely and responsibly on their sexual and reproductive health9, 22. For instance, the GSMF, through its TOOLGUARD programme provides sexual and reproductive health programmes to equip dressmakers and hairdressers between the ages of 17-35 years with the necessary information on HIV/AIDS and fertility management issues to help them make informed and responsible choices regarding their sexual health. The TOOLGUARD programme has recruited and trained about 460 dressmaking and hairdressing apprentices nationwide as peer educators and equipped them with toolkits to use in educating their colleagues9. Besides, some 300 salons and dressmaking shops have been branded and stocked with a variety of HIV/AIDS and other reproductive health literature, such as leaflets, mirror messages and other behavioural change materials to serve as resource centres to other users of the shops/salons. Failure to provide positive behavioural change programmes in sexual and reproductive health could lead to human resources that are not well positioned to take productive decisions on STDs, abortions, contraception, personal hygiene, nutrition and family planning. The long term implications would be an increase in the dependency ratio, intimate partner violence, unwanted pregnancies, unsafe abortions, increased child and maternal mortalities. The provision of education and services on sexual and reproductive health involves several stakeholders operating at different levels and in continuum. The national social, cultural or political environment generally prevailing in the community or country must be conducive for the delivery of such services.In the same vein, the different communities (and families) where individuals live should be supportive in the provision of such services. Furthermore, the services have to be available and should address the needs of the individual concerned. Ghana intends to become a modernised and middle income country in the next few years. The achievement of the above depends on the quality of Ghana’s human resource. The existing sexual and reproductive health education programmes should be broadened to incorporate the peculiar needs of the population. They must also be accessible to the section of the population that have not been previously targeted. New programmes must also be introduced to deal with the specific needs of the people who work in the informal economy including dressmakers and hairdressers. It should be noted that the social, cultural and economic context within which dressmakers and hairdressers find themselves, the availability of institutions to provide comprehensive sexual and reproductive health policies and programmes within the prevailing social, cultural, economic or political context to the population as well as the consequences of poor or non-existent sexual and reproductive health education programmes on the individual, community or nation are linked and interrelated. This will require that an integrated approach be adopted in providing education on sexual and reproductive health to the people of Ghana including dressmakers and hairdressers. The principal objective of the study was to assess the delivery of sexual and reproductive health education to dressmakers and hairdressers in the study area. Specifically, the study sought to (1) identify the existing sexual and reproductive health education programmes dressmakers and hairdressers in the study area were knowledgeable of, (2) determine the sources of information on sexual and reproductive health available to dressmakers and hairdressers in the study area, (3) assess the communication pattern(s) on reproductive health among the dressmakers and hairdressers at their workplaces, (4) evaluate the contribution of institutions in the provision of sexual and reproductive health education to dressmakers and hairdressers in the district, and (5) recommend measures that could be adopted to ensure effective delivery of sexual and reproductive health education to dressmakers and hairdressers. Methods The study was conducted in the Assin South District (ASD) in the Central Region of Ghana. The district could be described as rural in nature. According to the 2000 Population and Housing Census, the population of the district was 98,228 with a sex ratio of 99 males to 100 females 23. The majority of the adult population (72.2%) were predominantly cash crop farmers who were mainly into the cultivation of cocoa, oil palm and citrus. Other important economic activities in the district were dressmaking, hairdressing and petty trading. At the time of the study, the district was served by six Health Centres, two Health Posts and three Community-based Health Planning and Services (CHPS) Compounds. These facilities provide general health services including sexual and reproductive health care and counselling. Figure 1 is the map of the Assin South District. This exploratory research targeted all dressmakers and hairdressers in the Assin South District in the Central Region of Ghana. The accessible population was, however, the dressmakers and hairdressers who were identified undertaken dressmaking or hairdressing activities during the period of the data collection. It became evident during a preliminary survey that data on the number of dressmakers and dressmakers were non-existent in the district. It was also difficult to locate all the shops or salons of potential respondents because some operated from their homes, kiosks, on verandas or as itinerant dressmakers and hairdressers. Although the two vocations have well organised national secretariats, the same could not be said about the district. They could best be described as non-functional. At least during the study period no NGO was working in the study area on sexual and reproductive health focussing on dressmakers and hairdressers. It was further observed that most dressmaking and hairdressing activities were undertaken in urban and semi-urban areas in the district. The major semi-urban and urban settlements in the district were therefore purposively sampled as study sites. The study was therefore conducted in eleven settlements namely Nyankomase Ahinkro, Katakyiase, Assin Ngresi, Ankwaso, Darmang, Nsuem, Kyekyewere, Assin Manso, Assin Andoe, Assin Atonsu and part of Assin Fosu that was within the Assin South District. The snowballing technique was therefore employed to identify a shop or salon which then became the basis for selecting the respondents. The census method was employed to reach fulltime dressmakers and hairdressers as well as their apprentices. The supervisors and apprentices were both included in the study as a result of the need to gather data on sexual and reproductive health discussions at the workplaces of dressmakers and hairdressers. The census technique resulted in contacting 148 dressmakers and hairdressers comprising 119 individual respondents and 29 focus group discussants. Finally, the district director of health services in-charge of reproductive health, the leadership of the two vocations and a staff at the Business Advisory Centre of the District Assembly were purposively sampled as key informants to provide insights on the overall sexual and reproductive health education situation in the district. In all 153 respondents provided primary data for this study. The main data collection instruments were questionnaires, focus group discussion and in-depth interview guides. Results Background characteristics of the respondents Age, sex and marital status are important variables in analysing demographic trends 24. As indicated in Table 1, the majority of the respondents in both vocations were females. In both vocations, almost all the respondents (99%) were aged between 15 and 35 years. The age distribution of the respondents indicates that a higher proportion of them were young (15-24 years) and within their reproductive ages (15-49 years). Table 1: Background characteristics of respondents
N= Number of respondents The high proportion (93%) of respondents who completed only the basic education corroborates the findings that large proportion of the population attains only the basic education as their highest educational level18-19. Again, the level of educational attainment of the respondents confirmed the observation that the informal economy was fraught with mainly the youth and women who are essentially low-skilled and semi-literate 12-13, 25-27. Of the total respondents, more than two-thirds of the dressmakers (69%) and hairdressers (69%) have never been married. Relationship to household head Indeed, the size, nature and composition of the household in which dressmakers and hairdressers live are very essential in determining the sexual behaviour and knowledge of reproductive health of dressmakers and hairdressers. In one of the key informant interviews, the respondent had this to say:
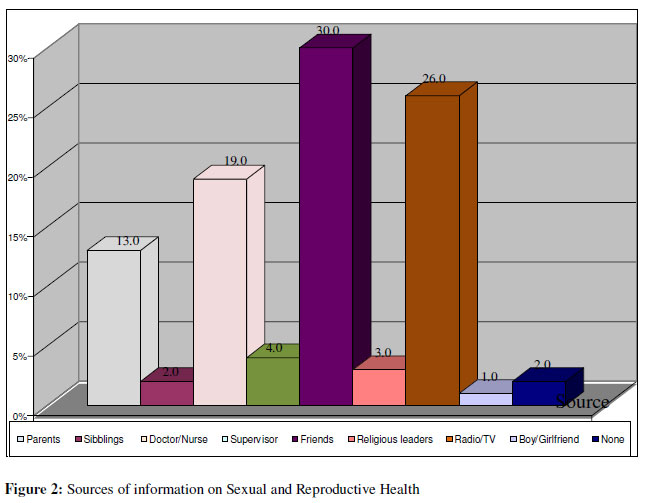
Sources of information on sexual and reproductive health It could be observed from Figure 2 that the major source of information on sexual and reproductive health available to individual respondents was through their friends (30%) followed by radio/television (26%) and parents (13%). These variety and authentic sources of information enable the respondents to make decisions and choices on sexual and reproductive health issues. Awareness of Sexual and Reproductive Health Education Programmes A prudent assessment of the respondent’s awareness of and their levels of interest in some of the sexual and reproductive health education programmes being implemented in Ghana are presented in Table 2. Mmaa Nkomo, an interactive programme on wide ranging issues of family planning, sexual and domestic violence, seems to be the most popular among the respondents. The popularity of this programme may be due to the fact that it has been consistently aired on television every week for the past decade. This gives credence to the notion that continuity is a fundamental aspect of learning and that different sets of audience can be reached through a series of different materials, messages and campaigns 28. Nearly 20% of the respondents could not identify any sexual and reproductive health related programme. The programmes mentioned in table 2 constitute the respondents’ sources of education and understanding of sexual and reproductive health programmes. Recently discussed topics in Sexual and Reproductive Health education Observations from Table 3 show that as high as 32% of the respondents could not recall the topic discussed during the last sexual and reproductive health education programme. While “Relationships” was the common topic among 39% of the dressmakers, sexuality was also a general topic cited by 20% of the dressmakers and 20% of the hairdressers. Table 2: Sexual and reproductive health education programmes in Ghana
Table 3: Topic for recent sexual and reproductive health education
Communication in Sexual and Reproductive Health issues at workplaces Effective communication at workplaces is deemed vital in ensuring harmony, increased productivity and the building of strong relationships among co-workers. Table 4 indicates that while 18% of all the respondents were conversant with issues of sexual and reproductive health education and therefore hardly discussed them at workplaces; as high as 38% of them did not consider such issues as a priority for discussion. On the other hand, 28% of the respondents were always alone in their shops or salons and therefore missed the opportunity for such exposures. In a focus group discussion with hairdressers, a 25 year old discussant said:
In a similar discussion with the dressmakers, discussants were forthright with their supervisor’s inability to educate them on sexual and reproductive health issues. According to a 22 year old dressmaker: Our mistress is very shy on sexual and reproductive health issues. She encourages us to concentrate on our vocation so that we can graduate in time. We do not discuss sexual and reproductive health issues to her hearing. She may think that we are spoilt girls. Table 4: Communication in sexual and reproductive health at workplaces
Access to mass media in dressmaking shop or hairdressing salon The respondents had far better exposure to mass media at their homes than workplaces. Explaining this further, a 22 year old hairdresser discussant had this to say:
Reasons for lack of interest in Sexual and Reproductive Health programmes A number of reasons were offered to justify respondent’s general dislike for sexual and reproductive health education programmes aired through the mass media. During a focus group discussion with hairdressers, some of the discussants expressed reservations for deliberately listening to such programmes. According to them, they do not want to show keen interest in such programmes to avoid being labelled as “spoilt girls” because already some members of the public perceive dressmakers and hairdressers, especially the apprentices, as people with weak morals who engaged in unhealthy sexual and reproductive health practices such as having multiple sexual partners and aborting the foetus when pregnant. A 20 year old hairdresser remarked:
Institutional support Responses from in-depth interviews of key informants in the district suggested that not much had been done by the various institutions to provide dressmakers and hairdressers in the study area with sexual and reproductive health education. It was also established that the district secretariat of the two vocations, Ghana National Tailors and Dressmakers Association and the Ghana Hairdressers and Beauticians Association, were non-existent in the Assin Area, at least during the period of the study, to organise programmes on sexual and reproductive health for their members. A 36 year old “executive member” of the dressmakers association in one of the settlements said:
The response of a ‘senior hairdresser’ was not different from her dressmaking counterpart. According to the 38 year old hairdresser:
Reactions of individual respondent’s on the significant contributions made by the institutions in the provision of information, education and communication including services on sexual and reproductive health to dressmakers and hairdressers indicate that no specific programme on sexual and reproductive health education had been organised for dressmakers or hairdressers in the district. Again, almost all the focus group discussants were unanimous in their responses that no institution had ever organised any educational programme on sexual and reproductive health for them. However, the Adventist Development and Relief Agency (ADRA) was cited by a discussant for organising a one day workshop on HIV/AIDS for Dressmakers. The agency had rounded up its activities in the district before the commencement of this study. According to a key informant in the district:
Discussion Ghana is making frantic efforts to reduce sexual and reproductive health related problems through the implementation of a number of sexual and reproductive health programmes and services. However, results from this study raise some major threats towards achieving this goal. For instance, some of the dressmakers and hairdressers de-linked their vocation from sexual and reproductive health while a large proportion of the respondents were either not interested in sexual and reproductive health education programmes or are ignorant about the existence of such programmes. Lack of coordinated and targeted programmes by government and private institutions on sexual and reproductive health education for dressmakers and hairdressers are indications that these groups within the country’s population are at greater risk of engaging in negative sexual and reproductive health practices 29. Currently, the informal economy is expanding in Ghana providing employment to a large proportion of the youth 12-13, 26. The formal economy, in most instances, depends on the services of the informal economy to exist and expand30-32. It becomes imperative that people in the informal economy are provided with information to make informed decisions and choices on sexual and reproductive issues since the continuity of the human race does not only depend on quantity but also quality of the people as well. Supervisors in the various shops and salons were not keen on discussing sexual and reproductive health related issues with their subordinates. Rather, peers who are their immediate contact persons have become the important sources of such information. The unstructured sexual and reproductive health education programme(s) specifically designed for dressmakers and hairdressers and other workers in the informal economy could undermine the quest for harnessing the full potential of every Ghanaian for national development Conclusion Meeting the sexual and reproductive health needs of Ghanaians is one of the key challenges confronting policy makers and implementers. Providing antidotes to these challenges require new insights into the overall effectiveness of existing policies and programmes and how operators in the informal economy will have access to and use of sexual and reproductive health information. Based on the findings of the study it is recommended that (1) it is recommended that dressmaking and hairdressing supervisors in the various shops or salons could be periodically trained in sexual and reproductive health issues by reproductive health training institutions or organisations to engage their subordinates in formal discussions on sexual and reproductive health issues, (2) the perceived misconceptions and taboos associated with sexual and reproductive issues should be urgently demystified to provide enough public discussion and affirmative action, (3) the institutions involved in reproductive health advocacy programmes will develop Behavioural Change Communication programmes messages targeting dressmakers and hairdressers. This will enable the dressmakers and hairdressers to make informed decisions on matters related to their sexual and reproductive lifestyles, and (4) a detailed study on sexual and reproductive health education in the informal economy of Ghana to be undertaken by research institutions to inform policy formulation and programming is also important. This will enable the government and other development partners to address the development challenges of Ghana holistically. References
Copyright 2011 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh11058f2.jpg] [rh11058f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}