 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
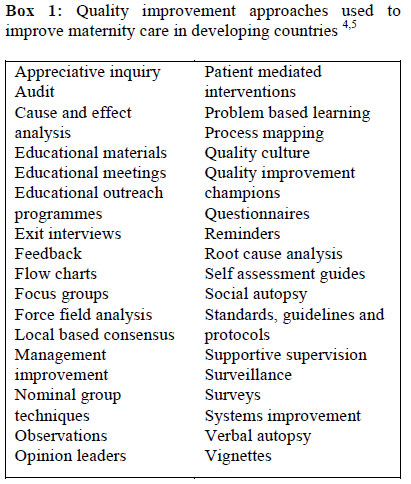
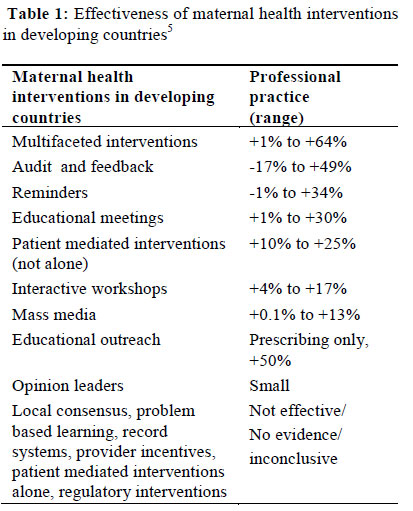
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 9-14 EDITORIAL Time for Action: Audit, Accountability and Confidential Enquiries into Maternal Deaths in Nigeria Temps d’agir: Vérification, responsabilité et enquêtes confidentielles sur les décès maternels au Nigéria Julia Hussein* and Friday Okonofua2 1Initiative for Maternal Mortality Programme Assessment (Immpact), University of Aberdeen, Scotland; Code Number: rh12001 Abstract Improving the quality of care is essential for achieving reductions in maternal mortality. Audit is one of the methods which can be used to simultaneously assess as well as improve quality. This commentary discusses one type of audit – confidential enquiries into maternal death. We believe that the enthusiasm for establishing a confidential enquiry system in Nigeria is growing. The challenges faced in setting up an audit system are discussed and 6 steps are proposed to locate the conduct of a confidential enquiry as part of a set of activities which will take cognizance of existing know-how, create shared ownership and provide a coherent picture of needs and information gaps in the provision of quality maternity services. Having such a system in place can be a route towards achieving a progressive vision of accountability for the reduction of maternal mortality in Nigeria (Afr J Reprod Health 2012; 16[1]:9-14). Résumé L’amélioration de la qualité de soin est nécessaire pour assurer les réductions dans la mortalité maternelle. La vérification est une des méthodes qu’on peut utiliser simultanément pour évaluer et améliorer la qualité. Ce commentaire discute un type de vérification – les enquêtes confidentielles sur le décès maternel. Nous sommes persuadés que l’enthousiasme pour l’établissement d’un système d’enquête confidentielle au Nigéria s’accroît. Les défis auxquels l’on fait face quand on établit un système de vérification sont discutés et nous proposons six démarches pour situer la conduite d’une enquête confidentielle comme faisant partie d’une série d’activités qui tiendront en compte le savoir-faire actuel, qui créeront une priorité partagée et rendront une image cohérente des besoins et des déficiences au niveau de l’information en matière de la dispensation des services de maternité de bonne qualité. Si l’on met un tel système en place, il pourra être un moyen d’accomplir une vision progressive de responsabilité pour la réduction de la mortalité maternelle au Nigéria (Afr J Reprod Health 2012; 16[1]:9-14). Keywords: Confidential enquiry, maternal mortality, Nigeria, accountability, audit Introduction Universal access to maternal health care is recommended for achievement of the millennium development goal target 5 of maternal mortality reduction. Within the paradigm of universal access, improvement in the coverage of health services is important, but it is also crucial that the services accessed should be of high quality. 1,2,3 Efforts to increase coverage and utilization of services are more likely to be sustained if women can find care where they know their lives and that of their babies will be in safe hands. Audit and quality improvementBut how does one go about improving quality of maternity care in a scaled up manner? The literature is replete with different quality improvement approaches. Many have been tried out in maternity settings in developing countries (Box 1). They include traditional strategies like educational meetings, self assessments and clinical protocols, as well as newer, innovative means such as process mapping, patient mediated interventions and force field analysis. 4,5 The effects of some of these quality improvement efforts have been evaluated and are summarized in Table 1.5 Audit is one of the methods commonly used for quality improvement in maternal health care. Evidence on its effectiveness varies, with some studies reporting negative effects, while others show improvements in professional practice by nearly 50%.5 amongst the quality improvement strategies, audit has some unique characteristics. Firstly, the full audit cycle comprises five key steps: case identification, data collection, analysis of findings, action and refinement. 6 This reiterative process implies that audit has to satisfy two concurrent roles, to improve quality, and also to measure it. Secondly, quality is made up of three distinct components: structure (for example, the adequacy of health facilities, equipment and staff); process (whether appropriate clinical management and care is provided); and outcome (such as case fatality, stillbirths or morbidities).7 Of these three key components, audit measures the most elusive but arguably the best indicator of whether care is being adequately provided.8 So, despite the uncertainty about its effectiveness, audit continues to be widely used to assess and to drive quality improvement. In the maternal health field, two main types of audit are described. Criterion based audits are founded on the use of pre-set criteria and generally produce quantitative assessments. Critical incident audits are not usually assessed against set criteria and include maternal death reviews and confidential enquiries. 6 Confidential enquiries into maternal deaths Confidential enquiries study adverse events related to maternal deaths, identifying areas of poor clinical practice with the aim of improving quality of care. To conduct a confidential enquiry, a panel of clinicians from several different disciplines appraises cases of death. The assessment usually uses clinical case notes as a data source and results in the issue of a high level policy report with key recommendations.6 Confidential enquiries are in place in some developing countries, including South Africa, Malaysia, Egypt and Jamaica, but are rarely established where levels of maternal mortality are highest. The barriers to implementation of confidential enquires are likely to be related to the organization and functional capacity of the health system with poor quality documentation; overly onerous clinical workloads resulting in lack of interest and low priority given to making clinical care accountable; and fear of negative consequences such as litigation or exposure. 9 In contrast, maternal death reviews are more widely conducted. Although sometimes described as interchangeable with confidential enquiries, there are key differences between the two approaches which affect their utility as a quality improvement mechanism. Maternal death reviews are usually done at a local level, for example, within a health facility or a district. The findings are less likely to be collated, not seen as being nationally representative and therefore have less weight in influencing policy.6 Although maternal death reviews done locally have the advantage of providing immediate feedback at the local community, facility or district level, there are important disadvantages of such a system. Confidential enquiries espouse concepts of confidentiality (no patients are named) as well as anonymity (the people involved and the hospitals are not known), obviating concerns of punitive action and blame, thus encouraging open, objective assessment of events. The localized nature of maternal death reviews however, make it difficult to ensure confidentiality or anonymity, so the reviews can engender lack of objectivity, feelings of defensiveness and fears of being blamed. There have been a number of practical ways that confidential enquiries and maternal death reviews have been adapted to improve their uptake. These include: offsetting the negative nature of the process by identifying positive events; using selected samples of cases to reduce the workload of appraising large numbers of deaths; and using interviews with care providers and relatives involved in the event to supplement lack of hospital documentation and to investigate social, behavioral and systems factors in the community.9 Key lessons have been learnt from these innovations. The lack of availability or poor quality of clinical case notes can be overcome by using the tested adaptations. Appraisal of even negative outcomes like death can result in identification of some positive actions or factors, and the practice of doing so is useful and motivating when conducting a confidential enquiry. The costs of holding a confidential enquiry are not prohibitive and can be limited by assessing a sample of cases and by conducting intermittent rounds, rather than continuous cycles of enquiry. 10 Audit in Nigeria Nigeria’s maternal mortality ratio was estimated at 545/100,000 live births in the 2008 demographic and health survey11 although considerable controversy surrounds this and the various other estimates available. Although improvements in maternal health have been prioritised by government, various factors prevent effective implementation, including preferences for delivering at home, low perceived quality of health services, poor linkages between levels of health care provision and delays in referral. 12 Nigeria has built up considerable experience in the conduct of audit. In a search of PubMed, we found 112 maternal audit studies conducted in Nigeria since 1990. Of these, the vast majority were conducted in tertiary, teaching hospitals. Few studied rural health facilities. Almost all studies were confined to individual hospitals and did not collate or compare data across hospitals or within a specified area. One nationwide study investigated opportunities for national level data collection on maternal mortality and morbidity, but nevertheless concentrated on tertiary level health facilities.13 It may be that audits, including maternal death reviews, are being done in other types of health facilities and are not published, but it is likely that such efforts are sporadic and uncommon. The situation described raises two concerns. In a country with only 35% of births taking place in health facilities,11 the focus on tertiary level facilities must represent only the ‘tip of the iceberg’. The data generated will tell us little about the circumstances and quality of care that most women (who do not reach these tertiary facilities) encounter during pregnancy and childbirth. The second issue is that studies confined to individual hospital settings cannot pool data, make comparisons or provide a comprehensive picture of the quality of service provision within the health system of a particular state or geographical area. Despite the many individual studies, there appears to have been little attempt to combine audit efforts to improve the understanding of the health system as a whole and the interlinkages between various levels of health care delivery. The result is that the findings of the audit tend to be of interest to individual clinicians, hospital directors and administrators of single facilities, rather than having the power to influence decision makers, politicians or governors at regional, state and local government level. Advocates of confidential enquiry have long awaited its commencement in Nigeria.13,14 There are indications of progress, for example, Governor Olusegun Mimiko of Ondo State has signed into law a bill on confidential enquiry into maternal deaths, demonstrating that political support can result in big strides forward. 15 Time for action Having observed the momentum built up and the support for confidential enquiries in particular, at the recent SOGON (Society of Gynaecology and Obstetrics of Nigeria) conference in Ibadan, we see Nigeria on the cusp of change. Ensuring that the excellent efforts of many do not disintegrate into intentions not translated into action is crucial. At this moment, some of the challenges faced are:
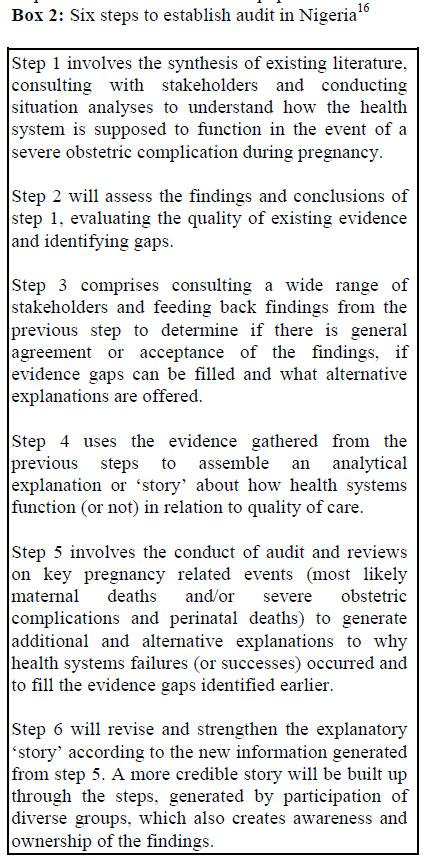
To some extent, decision making around the first two points in the list above are organizational -the institutional base for maternal audit in Nigeria should have a track record, demonstrable capacity and wide credibility to act as a national point of reference. The designated constituent(s) of this base should show leadership, but also have the commitment and interest in bringing together and coordinating the formulation of a national system for audit that is perceived as mutually owned by diverse groups of stakeholders. Generating the depth of understanding of the existing situation will involve more than a single survey or study. It is imperative that the wealth of experience and knowledge existing in Nigeria is marshaled, collective lessons learned, feedback and consultation reiteratively undertaken so that key gaps in knowledge are systematically identified and filled using both qualitative and quantitative data and approaches. Demand for evidence will need to be assessed and responses to fulfill the demand adequately will require insight into the needs of diverse groups, from potential influencers within the community and health services, to people whose voices are not always heard. Reaching out to all levels of the health system including the community will need utilization of innovative ways to conduct confidential enquiries and other forms of audit. Borrowing from the idea of ‘contribution analysis’ 16, we believe that these challenges can be met by situating the conduct of a confidential enquiry within a larger set of activities which include evidence synthesis, building of participatory involvement and generation of explanatory ‘stories’ as shown in the 6 steps in Box 2. Accountability in maternal mortality reduction Accountability is not necessarily a welcome concept, least of all by those in power, public servants, or those who are perceived to be responsible for the welfare of a population or state. One explanation for this situation may be that the traditional view of accountability emphasized control and blame, identifying a responsible person and taking appropriate action when things went wrong. Today, we face a more complex management context, where several people may be involved in influencing an outcome, with constraints around their own authority and the resources available. Effective accountability means that such factors are considered and that capacity is available to deal with these complex situations17 . Perceptions of accountability must change: blame should be replaced by views of ‘making a difference’ and ‘contributing to results’. Establishing a scaled up audit system in Nigeria may be the route toward achieving a progressive vision of accountability in maternal mortality reduction. Conclusion
If we agree that the risk of a mother dying in pregnancy is too high, we need to ask ourselves first, whether we can continue to rely on trust, and if not, whether we need to heighten our checks and balances -through the use of audit -in order to reduce maternal mortality. In Nigeria, the time to introduce a confidential enquiry process is right. The time for action is now. Acknowledgements This article was based on a presentation given at 45th the Annual Scientific Conference of the Society of Gynaecology and Obstetrics of Nigeria (SOGON), Ibadan, 22nd to 26th November 2011. We would like to acknowledge the support provided by the John D. and Catherine T. MacArthur Foundation which enabled the first author to attend the conference. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12001t1.jpg] [rh12001b1.jpg] [rh12001b2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}