 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 23-34 ORIGINAL RESEARCH ARTICLE The Reach and Limits of the US President’s Emergency Plan for Aids Relief (PEPFAR) Funding of Prevention of Mother-to-Child Transmission (PMTCT) of HIV in Nigeria La portée et les limites du plan d’urgence du Président américain à l’égard du financement des secours au SIDA (PUPFSS) pour la prévention de la Transmission du VIH de la mère à l’enfant (PTME) au NigériaChigozie Ezegbe1 and Niamh Stephenson*2 School of Public Health & Community Medicine, University of New South Wales, Sydney, Australia
Code Number: rh12003 Abstract WHO advocates the use of comprehensive 4-pronged strategy for PMTCT of HIV. It includes HIV prevention, preventing unintended pregnancies in HIV positive women and follows up treatment and support as well as therapeutic interventions around delivery. This study examines PEPFAR’s funding of Nigerian PMTCT, via an analysis of the funded activities of 396 agencies PEPFAR funds to do PMTCT. PEPFAR Sub-partners selected for this study were included because they were funded to do therapeutic intervention around delivery, but significant gaps were identified regarding the other 3 prongs advocated by WHO. Up to 70% were not funded to do any primary prevention. PEPFAR’s own reporting does not allow assessment of Sub-partner involvement in preventing unintended pregnancies. Regarding follow up treatment and care, some Sub-partners were not funded at all. PEPFAR is not supporting a comprehensive approach to PMTCT in the way it funds PMTCT in Nigeria (Afr J Reprod Health 2012; 16[1]:23-34). Résumé L’OMS préconise l’utilisation d’une stratégie compréhensive à quatre fronts pour la PTME du VIH. Elle comprend la prévention du VIH, la prévention des grossesses non-voulues chez les femmes séropositives, le traitement en postcure et d’appui aussi bien que les interventions thérapeutiques autour de l’accouchement. Cette étude examine le financement de la PTME du Nigéria par le PUPFSS à travers une analyse des activités financées auprès des agences financées, elles aussi, par PUPFSS pour réaliser la PTME. Les sous-partenaires du PUPFSS sélectionnés pour cette étude, ont été inclus parce qu’ils étaient financés pour réaliser des interventions thérapeutiques autour de l’accouchement, mais on a identifié d’importants trous à propos des trois autres fronts préconisés par l’OMS. Jusqu’à 70% n’ont pas été financés pour réaliser une prévention primaire. Le reportage par le PUPFSS ne permet pas d’évaluer la participation des sous-partenaires dans la prévention des grossesses non-voulues. En ce qui concerne le traitement en postcure et au soin, certains sous-partenaires n’ont pas été du tout financés. Le PUPFSS ne soutient pas une approche compréhensive à la PTME dans la manière dont il finance la PTME au Nigéria (Afr J Reprod Health 2012; 16[1]:23-34). Keywords: HIV, PMTCT, Prevention, PEPFAR, Nigeria Introduction The target of programmes on Prevention of Mother to Child Transmission of HIV (PMTCT) is to stop children from being infected during pregnancy, labour or breastfeeding. To achieve this, the effort of women, their sexual partners, health workers, governments and donors is necessary. Without any form of intervention 1 in 3 children born to a HIV positive pregnant mother is likely to become infected(1) . Around 60% of MTCT occurs in the days prior to or during delivery2. The rest are due to breastfeeding. In the absence of treatment more than 50% of the babies who get infected die before the age of 2(3). MTCT is avoidable: antiretroviral (ARV) prophylaxis during pregnancy if instituted in time, monitored and used with or without breastfeeding can result in a significant reduction of Mother to child transmission of HIV(4,5,6) . A number or antiretroviral drug regimens have been employed for PMTCT. Nigeria uses a triple regimen and double regimen at different stages of the pregnancy and labour according to WHO guidelines (1). However, there is more to PMTCT than ARVs, a point that has been advocated by WHO (7) . Arguably, the need to take a broad approach to PMTCT is particularly important now, considering that current efforts to scale up PMTCT are occurring at a time when treatment is being widely touted as the most promising means of prevention for all (8) a move that risks glossing what effective prevention actually entails (9) . Since 2001, WHO (7) has advocated a four pronged approach be used by all nations for effective PMTCT. The interventions should be as follows: i). Primary prevention of HIV infection among women of childbearing age. This entails services geared towards reduction in primary transmission of HIV. It includes HIV counseling and testing (HCT), health information dissemination and education on HIV and sexually transmitted diseases, harm reduction for women who inject drugs, condom programming and other primary preventive services (10) .
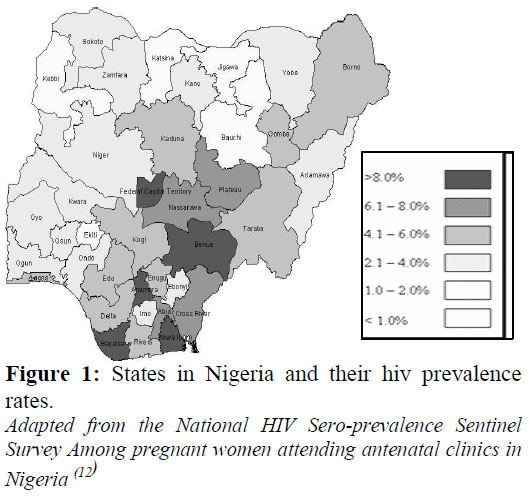
PMTCT in Nigeria Nigeria’s HIV prevalence (3.3million) is the 2nd highest in the world (1) . There are regional differences in HIV prevalence (Figure 1). The North-central region (6 States plus the FCT) has a prevalence of 7.5%, North-east region (6 States) 4.3%, North-west (7 States) 2.1%, South-south (6 States) 6.5%, South-east (5 States) 5.1% and South-west (6 States) 2.9%. HIV prevalence in different states ranges from 12.7% in Benue State in the North-Central region to 1.0% in Kebbi State in the North-west (12) . Nigeria has the highest burden of HIV positive pregnant women in the world despite all efforts (13). An estimated 85,450 HIV positive women give birth annually, or about 4.6% of all pregnant women resulting in about 56,681 annual HIV positive births (14). MTCT accounts for about 10% of new HIV infections annually in Nigeria (15) . PMTCT was flagged off officially by the Federal government of Nigeria (FGON) in July 2001 as a pilot project with six tertiary health institutions, one for each geopolitical zone (15). The nationwide coverage of the Nigerian PMTCT programme is poor: only 32% of HIV positive pregnant women that need ARV prophylaxis for PMTCT of HIV are getting it (14) . Since 2008, all tertiary health institutions provide HIV Counseling and Testing (HCT) during ANC, ARV prophylaxis for HIV positive pregnant mothers and ARV prophylaxis to newborns. These three interventions are part of WHO’s prong 3. But about 100%, 77% and 72% of the Secondary health institutions in Nigeria provide HCT during ANC, ARV prophylaxis for HIV positive pregnant mothers and ARV prophylaxis for newborns respectively. Only 53%, 36% and 10% of the primary health institutions which are largely located in rural areas provide these services (16). Whilst services are concentrated in tertiary and to a lesser extent secondary institutions, approximately 70% of births in Nigeria occur in the rural areas (17). Nigeria has the highest need for PMTCT, more than $80 million annually is required to adequately expand PMTCT services (18). Yet only about 3.2% of the $394.664 million made available from all sources for HIV was spent on PMTCT of HIV (or more specifically, WHO’s prong 3) (1) . Scaling up of services prevents a vast challenge – but not only financially. Some of the challenges include weak health systems, poor coordination and insufficient information on the scope of PMTCT services nationwide. Also the PMTCT services are largely donor driven with inadequate government supervision (14). Some agencies have come to the aid of Nigeria of which one of them is the United States President’s Emergency Plan for AIDS Relief (PEPFAR). In 2009 PEPFAR provided 88% of all international bilateral aid for HIV globally (1). One of the programme areas of HIV funded is PMTCT of HIV. PEPFAR in Nigeria Presently PEPFAR is the largest part of the United States’ government Global Health Initiative (GHI) (accounting for 73% of GHI funding requested for 2011) and the largest funding of global health by any nation (19). Initiated in 2003, PEPFAR targets HIV, TB and Malaria as global health problems through increased funding and technical assistance. Between 2003 and 2008 PEPFAR spent $18.8 billion (20). It has been re-authorized (2009 – 2014) with a budgetary proposal of $63 billion. In 2010 PEPFAR spent 81% of its budget on HIV/AIDS, and out of those funds, 37% was for treatment, 26% for prevention, 21% for care and support which includes care of orphans and vulnerable children and 16% for management, staffing, information and health system strengthening (21) . PEPFAR channels funds through 1) US departments and government agencies to 2) prime partners to 3) sub-partners who implement specific programs. The US Federal departments involved include the Department of State (State); United States Agency for International Development (USAID); Department of Health and Human Services (HHS) involving the Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), Health Resources and Services Administration (HRSA), Food and Drug Administration (FDA) and Substance Abuse and Mental Health Services Administration (SAMHSA); Department of Defense (DoD); Department of Commerce (DoC); Department of Labor (DoL) and Peace corps (22) . In many cases competitive bidding is used to choose new Prime partners for the purposes of expansion (23) . The United States embassy coordinates the activities of PEPFAR in Nigeria (in some countries it is state governments who coordinate PEPFAR activities, e.g. Vietnam). PEPFAR in Nigeria works through 59 Prime partners. They get funds through all the different US agencies mentioned above. Some of the Prime partners include US based organizations like American International Health Alliance Twinning Centre, Prohealth International, Vanderbilt University, University of Maryland Institute of Human Virology, John Hopkins University, Harvard University School of Public Health and John Snow Inc. They also include Nigerian government organizations like the Federal Ministry of Health National Blood Transfusion Service and faithbased organizations in Nigeria like the Catholic Secretariat of Nigeria (24) . These prime partners have more than 650 different sub-partners -which include government hospitals, private hospitals and local and international NGOs. In this way PEPFAR has provided more than $2 billion for the fight against HIV/AIDS in Nigeria (25) . PEPFAR (26) achievements up to 2010 include:
Given the scale and funding mechanism thework of effective coordination, evaluation and harmonization will always be a big challenge. The National Agency for the Control of AIDS (NACA) has stated that coordination is a big problem with PMTCT in Nigeria (14) . In line with the current challenges and requests from the FGON, PEPFAR will be paying more attention to PMTCT, orphan issues, behaviour change and prevention initiatives in the coming years. This, PEPFAR hopes to do by strengthening its collaboration with partners (e.g. FGON and The Global Fund) or other donors. It will be accompanied by an extra attention to human resources for health (27) . After reviewing the first phase of PEPFAR’s global strategy Sepulveda posited that the “ultimate success of the program will depend upon effective prevention” (28) . Perhaps in acknowledgment of this PEPFAR has earmarked 26% of HIV funds for prevention in 2009-14 (as compared with 20% at inception) (21) . Yet, as is commonly the case with donor driven health programmes, there are concerns that PEPFAR funds are allocated on an ideological basis and not scientific reasons therefore undermining prevention, e.g. the assigning of a significant proportion of resources for abstinence-only programmes which are not based on evidence that it is effective (29) . PEPFAR’s funding of PMTCT in Nigeria in relation to WHO’s four prongs? Given the need to scale up PMTCT in Nigeria and PEPFAR’s lead role in current PMTCT provision, and given concerns about donor driven approaches to HIV prevention, we undertook an analysis of PEPAR’s role in Nigerian PMTCT to date. This research evaluated the extent to which PEPFAR funded initiatives in Nigeria address not only the provision of HIV counseling and testing for pregnant women, anti-retroviral prophylaxis to HIV positive mothers and exposed babies as part of PMTCT (WHO’s prong 3) but extend to the comprehensive approach advocated to PMTCT in the form of WHO’s four prongs. More specifically the research questions we posed were:
Methods Data collection & coding The data for analysis were collected from PEPFAR’s Nigeria 2009-Country Operational Plan (COP). It contains the list of all United States’ agencies, Prime partners and Sub-partners and their funded HIV programme areas for the fiscal year 2009(27) . From the COP we identified the Sub-partners being funded for PMTCT with the PEPFAR budget code MTCT as part of their programme areas. This MTCT code according to PEPFAR means Sub-partners are funded to give ARV prophylaxis to HIV positive pregnant women during pregnancy and to their exposed newborns for one week postpartum, counseling and support for maternal nutrition and training of health personnel (30). This corresponds to prong 3 of the WHO recommendation -reduction of HIV transmission from women living with HIV to their infants. We then examined the COP to identify the extent to which these MTCT funded Sub-partners are involved in the other programme areas of the four prongs advocated by WHO. We identified alignments between PEPFAR’s programme areas and WHO’s 4 prongs as follows (The codes in bracket are PEPFAR’s codes): PRONG 1: Primary prevention of HIV infection among women of childbearing age: a) Abstinence and fidelity (code -HVAB) - Promote abstinence, fidelity and reduce barriers to necessary behaviour change. PRONG 2: Prevention of unintended pregnancies among women living with HIV-No code was found. PRONG 3: Reduction of HIV transmission from women living with HIV to their infants -This includes HIV counseling and testing (code-HVCT), anti-retroviral prophylaxis for HIV positive pregnant mothers, exposed babies and counseling for infant nutrition (MTCT). As mentioned, the MTCT code was the basis for selection which means all the sub-partners selected are involved. PRONG 4: Treatment, care and support to Mothers living with HIV, their children and families – Adult anti-retroviral therapy (code-HTXS), Adult care and support or psychosocial counseling and support (code -HBHC), Pediatric care and support or psychosocial counseling and support (code-PDCS) and Pediatric anti-retroviral therapy (code-PDTX). By identifying and mapping these codes for each of the sub-partners with the MTCT code we could gauge the extent to which PEPFAR funds the other 3 prongs of PMTCT. Subsequently, we collected information on total funds allocated to these sub-partners and their geographical distribution in Nigeria as a means of engaging the extent to which PEPFAR’s investment overlaps with the patterning of the HIV epidemic in Nigeria. Results The complex flow of PEPFAR funds to Subpartners with the MTCT code A total of 396 Sub-partners (about 45%) out of 892 Sub-partners had MTCT as part of their budget code in the PEPFAR 2009 COP. Their funding came through ten different funding mechanisms. As described above, each funding mechanism starts with PEPFAR allocating funds to United States agencies that channel it to prime partners who then send it on to a host of subpartners who implement programmes. More specifically the pathways identified were:
The Sub-partners include: government run Federal Medical Centres and Teaching hospitals like Lagos University Teaching Hospital (tertiary institution) and Primary health centres; NGOs; faith based organizations like some dioceses of the Catholic Church in Nigeria; and foreign based institutions like Howard University US. Interestingly, the Sub-partners are allowed to subcontract to ‘subs-of-subs’ but these are not documented in the COP. Identifying these funding channels shows us that there is a complex crisscrossing of organizations involved in PEPFAR funded PMTCT efforts in Nigeria
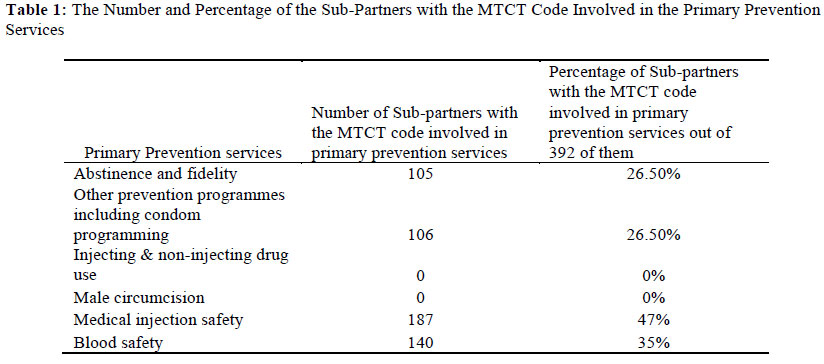
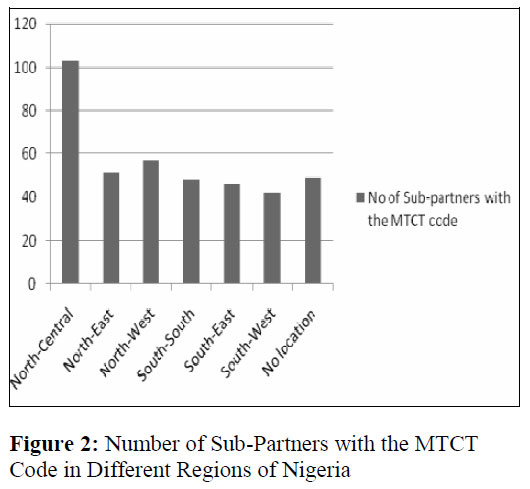
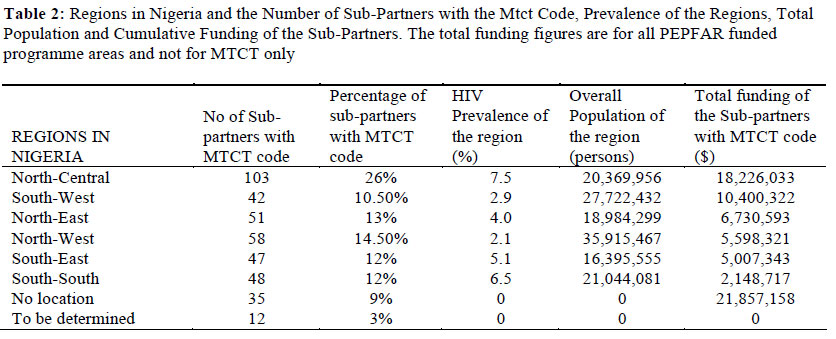
Table 2 shows that the North-Central region has the most MTCT funded Sub-partners and the highest prevalence rate in Nigeria of 7.5%,. But the South-south, which has a very similar total population and the next highest prevalence rate (6.5%) has almost the least number of Subpartners. If the regions are compared on the basis of funding (Table 2) it appears that the South-South is not receiving a share of funding commensurate with epidemiological data. This raises questions about the logic of fund distribution to Subpartners, and what can be done to ensure equity in the attempt to meet needs. In Summary, PEPFAR’s funding of PMTCT appears to support psychosocial counselling to a greater extent than it does ARV treatment for adults and children. The role of primary prevention services in PMTCT does not appear to be a priority, a little over one third of MTCT funded Sub-partners are funded for community based prevention. The benefits accruable from the integration of HIV programmes with family planning are being lost. Discussion As of 2011 (14), only 32% of women in Nigeria who tested positive during pregnancy received ARVs, there is an urgent need to scale up PMTCT services. And WHO has long recommended a comprehensive four pronged approach for PMTCT to make it more efficient and effective especially in nations with high prevalence (7). Our analysis of PEPFAR’s COP indicates that PEPFAR is assisting Nigeria in what de Waal (32) calls managing rather than solving the problem of HIV and there is considerable room for change. We identified and mapped the PEPFAR’s extensive funding of WHO’s third prong – provision of ANC-linked HCT and anti-retroviral prophylaxis for exposed women and babies (question 1). All Sub-partners selected are funded for this. Regarding our second question about primary prevention of HIV among women of childbearing age (prong 1), only about one-third of the Sub-partners that PEPFAR funds for PMTCT are funded for community targeted primary prevention services. This is arguably an instance of how global health’s focus on HIV treatment can detract from prevention (32) . Another instance of this is Peters et. al’s finding that the US and European Union governments are decreasing funding of condom programming while increasing funding of research on vaccinesanmicrobicides (33) . According to the Ottawa charter, health services are most effective when they operate with an expanded mandate that respects cultural needs, supports the needs of individuals and communities, and opens channels between the health sector and the broader environment(34) . In the context of PMTCT, community based primary HIV prevention is an important means of doing this. Regarding our third question, we found no evidence of PEPFAR’s funding of WHO’s second PMTCT prong, family planning. Expanding PMTCT efforts in Nigeria to include family planning is a valuable means of tackling HIV transmission, particularly because use is currently low. This is a problem that the Nigerian government has recently highlighted: NACA also included poor integration of HIV in Reproductive Health (RH) services as one of the challenges of PMTCT in Nigeria (14). Integrating family planning and HIV programmes and strengthening referrals from HIV clinics to Family planning clinics results in increased attendance on the part of both men and women to family planning clinics; in particular when both are administered in one location (35). This alignment of services is particularly important to develop as the Nigerian referral system is weak (36) . Donor programmes like PEPFAR should align their priorities in response to reliable information about local need (37) . Regarding our fourth question we identified more widespread PEPFAR involvement in funding psychosocial care and support for mothers (85%) and children (84%) than the provision of treatment to mothers (63%) and children (63%) (Prong 4). There are still gaps in treatment and support. More than 50% of Nigerians live below the poverty line and the majority live in rural areas with poor access to towns and information(38) and, as mentioned above, a poor referral service. If PMTCT services are not consolidated then the likelihood of attrition loss to follow up is very high. Even where the referral system is strong, transport costs could be prohibitive. Poverty affects retention in care(39, 40) . To effectively reduce transmission of HIV there is need to maximize the chances that those who willingly come for care and treatment stay in care. Our fifth question was about the extent to which the regional distribution of PEPFAR PMTCT Sub-partners reflects epidemiological data about the patterning of HIV prevalence in Nigeria. We identified considerable disparities, and the relative level of PEPFAR funding in the South-South seems particularly low. This raises questions about what can be done and whose responsibility it is to try to ensure more equity in the distribution of PMTCT funds. It also raises questions as to whether PEPFAR effectively funds PMTCT services according to expertise, or need, a mix of both or according to other criteria. However, funding should be aligned with the aim of FGON to increase access to comprehensive gender-sensitive prevention, care, treatment and support services for the general population contained in the national strategic framework (41) . Conclusion PEPFAR’s involvement in Nigeria via a multiplicity of US agencies and prime partners is vertically organized. It is increasingly widely recognized that in place of vertical programming, funders like PEPFAR can be most effective if their interventions are flexible and designed in response to local needs (42). This should be the case for HIV prevention (43) and, we argue, for the provision of PMTCT. In addition to responding to the specificities of HIV epidemics, vertical organization can prove to be difficult to coordinate. In a context where referrals are already weak such poor coordination is likely to result in highly patchy access to comprehensive PMTCT services. Vertical organization of donor funding risks having the unintended consequence of making the Nigerian health system more dependent rather than strengthening the national capacity to provide PMTCT. Already PMTCT programmes in Nigeria are largely donor driven (14) . In the process of scaling up health services national involvement and where possible ownership should be encouraged (44) . This will reduce dependence over time. The development of country involvement should include strengthening the health system to enhance comprehensive HIV prevention and care. It is through health system strengthening that global health initiatives like PEPFAR can further their role in solving rather than managing global health problems and in this case HIV (45) . Putting structures in place to advance national involvement and ownership is key to sustainability. The present pattern of funding is not only patchy, but it is organized in a way that risks excusing the Nigerian government and their health workforce. As PMTCT efforts are being scaled up, tighter coordination between donors and FGON can involve training health workforce as part of health system strengthening. In conjunction with wider, better integrated and more comprehensive service delivery a better trained FGON workforce will lead to better access, coverage, quality and safety not just to PMTCT initiatives but to broader health service provision more generally in Nigeria (46). Through this way the national PMTCT target of making HCT available to 80% of pregnant women, ARV prophylaxis to 80% of HIV positive pregnant women and exposed babies by 2015 will be realized (14) . Ultimately, maternal to child transmission will be cut down further through combined action on the four prongs. This broad approach to PMTCT is even more necessary in high-burden nations like Nigeria, where the focus of ending MTCT should be at the population level in the first instance (11) . Improving PMTCT services in terms of quality and access and the collaboration between all stakeholders in public health in Nigeria will determine the overall success in years to come. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12003f1.jpg] [rh12003t1.jpg] [rh12003t2.jpg] [rh12003f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}