 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
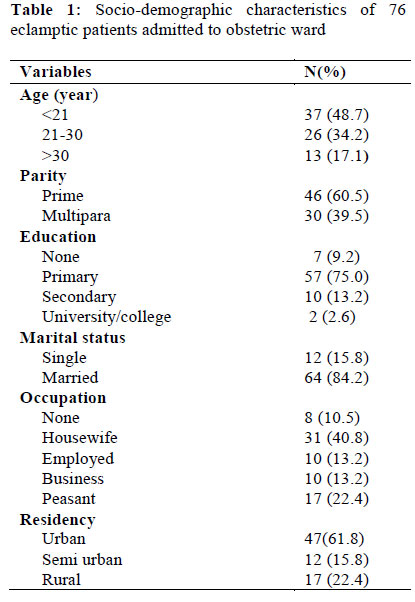
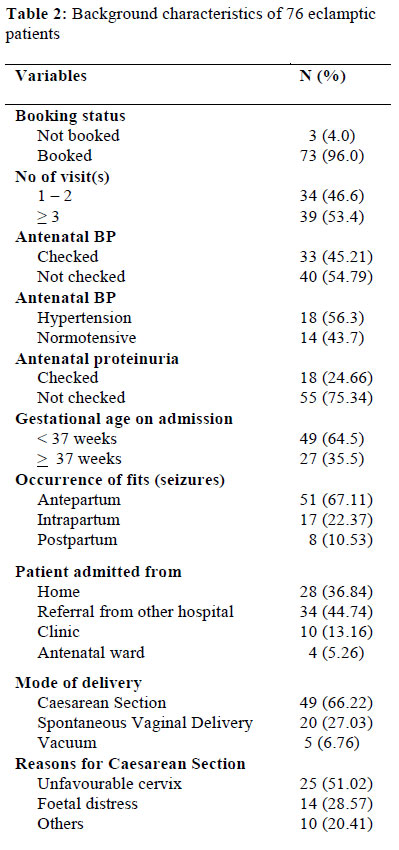
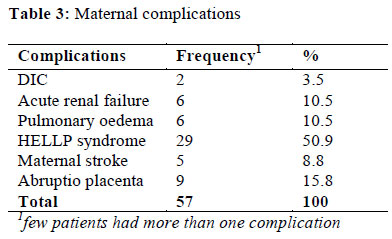
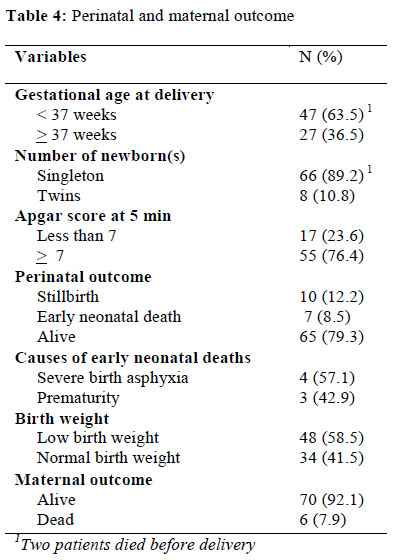
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 35-41 ORIGINAL RESEARCH ARTICLE Maternal and Perinatal Outcomes among Eclamptic Patients Admitted to Bugando Medical Centre, Mwanza, Tanzania Conséquences maternelles et périnatales chez les patientes atteintes de l’éclampsie qui sont admisses à Bugando Medical Centre, Mwanza, TanzanieEdgar M Ndaboine1 , Albert Kihunrwa1, 2 , Richard Rumanyika1, 2 , H Beatrice Im1, 3 and Anthony N Massinde1, 2 * 1Department of Obstetrics and Gynaecology, Bugando Medical Centre, Mwanza, Tanzania; Code Number: rh12004 Abstract Eclampsia continues to be a major problem, particularly in developing countries such as Tanzania, contributing significantly to high maternal and perinatal morbidity and mortality. We conducted a study to establish the incidence of eclampsia and the associated maternal and perinatal outcomes among eclamptic patients admitted to our center. A descriptive cross-sectional study of all women presenting with eclampsia was performed from June 2009 to February 2010. Seventy-six patients presented with eclampsia out of a total 5562 deliveries during the study period (incidence of 1.37%). Antenatal attendance was 96% among patients with eclampsia; however, only 45.21% and 24.66% were screened for blood pressure and proteinuria respectively. Maternal and perinatal case fatality rates were 7.89% and 20.73% respectively. The main factors contributing to maternal deaths were acute renal failure (10.5%), pulmonary oedema (10.5%), maternal stroke (8.8%), HELLP syndrome (50.9%), and Disseminated Intravascular Coagulopathy (3.5%). Perinatal deaths were caused by prematurity (42.9%) and birth asphyxia (57.1%). Forty-eight babies had low-birth weight (58.54%). The high incidence of eclampsia and its complications during this study period may indicate the need for earlier and more meticulous intervention at both the clinic and hospital levels (Afr J Reprod Health 2012; 16[1]:35-41). Résumé L’éclampsie ne cesse d’être un problème majeur, surtout dans les pays en développement tel que la Tanzanie, ce qui contribue significativement à la morbidité et à la mortalité maternelle et périnatale élevées. Nous avons mené une étude pour établir l’incidence de l’éclampsie et les conséquences maternelles et périnatales qui y sont associées chez les patientes atteintes de l’éclampsie admises dans notre Centre. Nous avons fait une étude transversale descriptive de toutes les femmes qui souffraient de l’éclampsie et qui venaient nous consulter dans notre Centre du mois du juin 2009 au mois du février 2010. Sur un total de 5562 accouchements au cours de l’étude, soixante-seize patientes souffraient de l’éclampsie (Incidence de 1,37%). La fréquentation au service de l’anténatal était de 96% chez les femmes souffrant de l’éclampsie ; toutefois, seulement 42,21% et 24,66% ont subi le test de dépistage pour détecter la pression artérielle et la protéinurie respectivement. Les taux de fatalité des cas maternels et périnatals étaient de 7,89% et 20,73% respectivement. Les principaux facteurs qui contribuent au décès maternel étaient l’insuffisance rénale (10,5%), l’œdème pulmonaire (10,5%), l’apoplexie cérébrale maternelle (8,8%), le syndrome de HELLP (50, 9%), et la coagulopathie intra vasculaire disséminée (3,5%). Les décès périnatals ont été causés par la prématurité (42,9%) et l’asphyxie de la naissance (57,1%). Quarante huit bébés avaient des poids de naissance bas (58,54%). La haute incidence de l’éclampsie et ses complications au cours de cette étude peuvent indiquer la nécessité des interventions plus tôt et plus méticuleuses aux niveaux de la clinique et de l’hôpital (Afr J Reprod Health 2012; 16[1]:35-41). Keywords: Eclampsia, maternal, perinatal, morbidity, mortality, Tanzania Introduction Eclampsia continues to be a major problem worldwide, particularly in developing countries. In Tanzania eclampsia is one of the leading causes of maternal mortality and morbidity. The maternal mortality rate related to eclampsia varies worldwide from 1.8% in the UK up to 43.1% in Nigeria.1, 2 Morbidity from eclampsia is associated with acute renal failure, pulmonary oedema, cardiopulmonary arrest, and aspiration.4,5 Perinatal mortality from eclampsia is reported to be 5% -11.8% in developed countries as compared to a developing nation such as Tanzania where eclampsia-related perinatal mortality can be as high as 40%.1, 6, 7 The causes of perinatal death are chronic placental insufficiency, preterm delivery, and placental abruption.8, 9 The aetiology of eclampsia has not yet been established and there are controversies surrounding the definition of an atypical presentation of eclampsia.10-12 In most cases the onset of pre-eclampsia is insidious, and pathological changes occur weeks before clinically detectable hypertension and proteinuria. In addition, symptoms occur only at the end stage of disease, just before the eclamptic episode. It has been established that good antenatal care can prevent the occurrence of eclampsia, though not in all cases.4, 13, 14 Therefore, the challenge is to balance the timing of delivery of pre-eclamptic patients before the onset of eclampsia with foetal viability. In developed countries, the incidence of eclampsia has fallen considerably. This decline has been attributed to improvements in antenatal and intrapartum care.3, 4 Despite a reported 97% rate of antenatal clinic attendance in Tanzania, adequate screening or identification of women at risk for eclampsia appears to be lacking.4 Maternal mortality due to hypertension and eclampsia was ranked as the third leading cause of maternal death in a community-based study in Ilala District, Tanzania.14 Eclampsia is also the leading cause of direct maternal death at two of the four major tertiary referral centres in Tanzania, Bugando Medical Centre (BMC) in Mwanza and Muhimbili National Hospital (MNH) in Dar es salaam.15-17 Despite the high prevalence of maternal and foetal deaths from eclampsia, there are no published data on the outcome of eclamptic patients at BMC. The purpose of this study is to analyse the incidence of eclampsia and to identify the maternal and perinatal outcomes of eclamptic patients treated in a tertiary care referral hospital. Methods Study setting A descriptive cross-sectional study was carried out between June 2009 and February 2010 in the Department of Obstetrics and Gynaecology at BMC. BMC is a teaching and referral hospital in Mwanza Region, Tanzania, with approximately 6,700 deliveries per annum. 15 Eclamptic patients at BMC are either admitted to the labor ward or postnatal ward unless they need intensive care, in which instance they are admitted to the Intensive Care Unit (ICU). Neonates of eclamptic women are admitted to the Neonatal Unit or the Neonatal Intensive Care Unit (NICU) for observation or treatment depending on the needs of the particular neonate. Study population Our study population included all pregnant women admitted to BMC for delivery during the study period. Eclamptic patients were identified during the hospitalization, and all data were collected from the patient or patients’ relatives after the appropriate informed consent was obtained. All babies delivered of eclamptic patients at BMC were also included in this study. Patients who presented with uncertain diagnoses and patients who had delivered and then were referred to BMC from a peripheral clinic were excluded from the study. Sample size and sampling techniques The sample size of this study was calculated using the Kish and Lisle method to obtain a prevalence of 5%. 6 The expected sample size was 73 patients. Serial sampling was used to recruit all eclamptic patients admitted during the study period until the desired sample size was reached. Data collection All relevant information regarding demographic data, clinical findings, laboratory results and each patient’s outcome and her newborn (s) were collected. Data about antenatal care were extracted from the patient’s history file and antenatal card. Maternal and perinatal variable measured Maternal data gathered include maternal age, parity, gestational age, admission blood pressure (BP), presence or absence of proteinuria on urine dipstick, the number and timing of seizure activity, and the mode of delivery. Lab values of interest included the complete blood count (CBC), creatinine, aspartate amino-transferase (ASAT), alanine aminotransferase (ALAT), and lactate dehydrogenase. Data from antenatal clinic include number of visits and any documented proteinuria and BP readings during those antenatal visits. The outcomes examined include the incidence of maternal death, stroke, HELLP syndrome, abruptio placenta, disseminated intravascular coagulation (DIC), pulmonary oedema, acute renal failure, perinatal mortality (including stillbirths and early neonatal deaths), preterm delivery, low birth weight babies, and low Apgar score. Data management and analysis Data collected from the data collection form were entered into EpiData version 3.1 and then transferred to STATA version 10.1 for analysis. Patient Management Management of eclamptic patients is according to our hospital protocol. Seizures are controlled by using magnesium sulphate 4 g as slow intravenous bolus followed by intramuscular injections of 10 g and then 5 g every 4 hours. The total duration of therapy is usually 24 hours from the last fit or delivery, whichever occurred first. Severe hypertension (diastolic BP of more than 110 mmHg) is managed with intermittent intravenous hydralazine. Investigations include ALAT, ASAT, CBC, and urinalysis are performed. Delivery of the patient is final treatment, and mode of delivery will be determined depending on Bishop’s score or any other additional obstetrical problem. Ethical consideration The study obtained clearance from the Bugando Research Ethics Committee. Results The incidence of eclampsia and social demographic characteristics There were 76 patients who presented with eclampsia out of 5562 deliveries during the nine month study period. This yielded an incidence of 1.37%. Of the women who attended antenatal clinic, 53.46% had had three or more visits. The mean age of the eclamptic patients was 23 years (ranging from 16 to 37), and the majority of these patients were primiparous (Table 1). Of all 76 eclamptic patients, 73 had attended an antenatal clinic prior to admission (Table 2). Most of the patients who attended antenatal clinic did not have their blood pressure and urine protein checked. According to the antenatal cards reviewed, only 45.21% had had a documented antenatal BP, and only 24.66% had had a documented antenatal urine dipstick result. Among the patients who had antenatal blood pressure screening, 56.3% were hypertensive during antenatal visits. Among those who developed eclampsia, 51 patients developed the condition before labour, 17 during labour and 8 in postpartum period. Forty-nine patients present with eclampsia before term, while all other presented at term. Many patients were either referred from other hospitals or came from home. Four patients were admitted to the antenatal ward due to severe pre-eclampsia and subsequently developed eclampsia. Ten patients came from antenatal clinics with eclampsia. More than half of the patients were delivered by caesarean section. The main reasons for caesarean section were unfavourable cervix remote from delivery and foetal distress. Maternal outcome There were six maternal deaths, two before delivery and four after delivery, accounting for a case fatality rate due to eclampsia of 7.89%. HELLP syndrome developed in 29 patients. A few patients had more than one complication at the same time. Causes of death included multi-system organ failure, pulmonary oedema, acute renal failure, stroke, and Disseminated Intravascular Coagulopathy (DIC) precipitated by abruptio placenta (Table 3). Perinatal outcome There were eight sets of twins and 66 singletons accounting for a total of 82 delivered babies. Forty-eight babies (58.54%) had a low birth weight. There were 17 perinatal deaths (10 stillborns and 7 early neonatal deaths) which yielded a perinatal mortality rate of 207/1000 births. The majority of these neonates were preterm. Birth asphyxia (defined as an Apgar score < 7 at 5 minutes) occurred in 23.6% of the live births (Table 4). Discussion To the best of our knowledge, this was the first study of maternal and perinatal outcomes among eclamptic patients to be conducted in the Lake Victoria region. Our study showed that the hospital-based incidence of eclampsia at BMC was 1.37%. The findings in our study concur with those in Benin, which reported the incidence to be 1.32%.18 However our incidence was lower when compared to studies done in Northern Nigeria, Uttar Pradesh-India and Muhimbili-Tanzania with the incidences of 9.42%, 2.2% and 2%-5%, respectively.2,4,6,19 The observed difference in incidences among the aforementioned areas could be explained by geographical variability, access to health care services and medical attention provided for patients. The incidence of eclampsia is very low within developed countries with a range of 0.29% -0.75%, due to the provision of standard antenatal care for most pregnant women in these countries.3, 20-22 Morbidity and mortality among eclamptic patients admitted to our hospital was similar to that of eclampsia-associated morbidity and mortality seen in other developing countries. We had a maternal case fatality rate of 7.89%, which was similar to that of Muhimbili, Tanzania (7.7%), and Benin (10.7%).6,18 However our case fatality was very high compared to studies conducted in United States of America, where the fatality rate is less than 0.5%.5, 22, 23 The high maternal mortality from complications of eclampsia is attributed to the limited capability to manage such complications in a low resource setting.6, 18 However, many of the maternal complications seen in the eclamptic patients appeared to arise from delays in the timely management of pre-eclamptic patients.24 High maternal mortality rates in countries with limited resources have sometimes been understood in the context of the three delays model. These delays include the delay in seeking medical care, delay in arriving at the facility, and delay in receiving standard care at the healthcare facility.25 Our data indicate that the third delay may be a major contributor to eclampsia-related maternal mortality in our region. A simple and effective method of screening for pre-eclampsia is to have blood pressure monitoring and proteinuria checked by dipstick in all pregnant women at every antenatal visit. However, information gleaned from patients’ antenatal cards show that among all women who developed eclampsia, only 45.2% had a documented BP and only 24.7% had a documented urine dipstick result, despite a high antenatal attendance rate of 96%. Failure to screen for such basic but important parameters may reflect the local clinics’ lack of access to basic equipment such as sphygmo-manometers and urine dipsticks. A study by Urassa et al demonstrated this to be the case in some parts of rural Tanzania14. While the data seem to indicate that inadequate care at the antenatal level was associated with maternal death, at the referral hospital level, a major predictor of maternal mortality was having multiple eclampsia-related complications. Many of the patients referred to our hospital from other centres were already critically ill. Our study’s findings of eclampsiaassociated morbidities and their outcomes concur with the findings of several different studies from other parts of the world.3,7,24,26-28 These associated complications contribute significantly to the challenge of managing eclamptic patients in our setting because of limitations in critical care resources such as dialysis for renal failure and adequate blood products to reverse DIC. While limited resources present a major challenge to taking care of the critically ill patient, patients also often presented to our facility already in critical or moribund stages because of delays in seeking health care by the patients themselves, providers’ failure to recognize and manage a critical situation at peripheral health facilities, and poor infrastructure preventing the timely transport of patients to a higher level facility.14, 25 Countries that have greatly reduced their maternal mortality appear to be those with not only adequate resources to manage critically ill patients but also provide such services in a timely fashion. 7 The majority of pregnant women in our study had eclamptic seizures before term and caesarean section was a leading mode of delivery, which is comparable to other studies.18, 29 In this study, the majority underwent caesarean section due to an unfavourable cervix remote from delivery and foetal distress. The presence of eclampsia alone was not an indication for caesarean delivery, but the decision to perform a caesarean delivery was based on multiple factors which included foetal gestational age, foetal status, the stage of labour, and cervical Bishop score.7 The perinatal mortality rate in this study was 20.7%, which is almost equivalent to the 21.4% reported in Benin. However, our rate was low compared to 40% at MNH.6, 18 The higher rate of perinatal deaths in our study and other similar studies6,18 could be explained by the three delays model as explained.25 Another contributing factor is the limitation in resources for managing extremely preterm infants. Our study revealed that the major causes of early neonatal deaths were severe birth asphyxia and prematurity. Other studies have reported similar findings.2,7,18 A significant number of low birth weight neonates might have been the result of the high number of preterm deliveries among the eclamptic patients. Similar findings have been reported in the literature that links the incidence of low birth weight infants with preterm deliveries in eclamptic patient.4, 5, 18 Conclusion We have demonstrated that the incidence of eclampsia at BMC was 1.37% and that the proper management of eclampsia at our hospital faces similar challenges as those at other hospitals in the developing world. Eclampsia found to cause maternal mortality and morbidity also contributed significantly to high rates of perinatal mortality. The most common causes of perinatal death were birth asphyxia and prematurity. Patient compliance was not shown to contribute significantly to the delayed management of eclampsia as demonstrated by the high rates of antenatal clinic attendance. However, many of these women were not screened for pre-eclampsia and consequently presented late to our hospital, frequently with complications. While factors such as limited resources and infrastructure are not within the control of the health care practitioner, attention to basic details is possible at antenatal clinics. Early intervention initiated by detection of abnormal values in basic tests such as blood pressure monitoring and urine dipsticks can often change the course of a patient’s disease management. Our best chance for reducing maternal and perinatal morbidity and mortality due to eclampsia may lie with the promotion of improvements in the quality of basic care provided by our antenatal clinics. Competing interests The authors declare that they have no competing interests. Authors' contributions These authors contributed equally to this work. Acknowledgements We would like to thank the team who worked with the department of Obstetrics and Gynaecology, including residents and nurses, who supported this research work. We thank them for all their help and support including the health care they provide to obstetric patients at BMC. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12004t4.jpg] [rh12004t1.jpg] [rh12004t3.jpg] [rh12004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}