 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
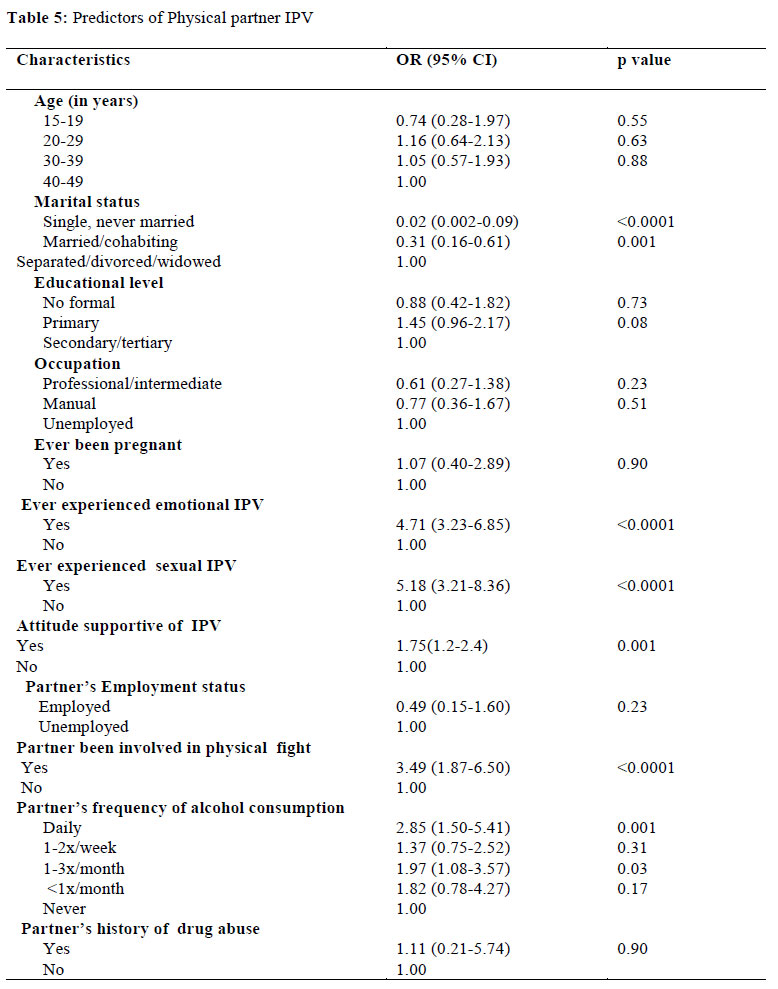
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 43-53 ORIGINAL RESEARCH ARTICLE Women at Risk of Physical Intimate Partner Violence: A Crosssectional Analysis of a Low-income Community in Southwest Nigeria Femmes en danger de violence physique causée par le partenaire intime : analyse transversale d’une communauté à faible revenu au sud ouest du Nigéria.Eme T Owoaje and Funmilola M OlaOlorun Department of Community Medicine, College of Medicine, University of Ibadan. Code Number: rh12005 Abstract Intimate Partner Violence (IPV) is prevalent in Nigeria but a culture of silence exists, making it difficult to identify women at risk. A descriptive cross-sectional survey was employed to determine the prevalence and predictors of physical IPV in a low income, high density community in south west Nigeria. Among 924 interviews of everpartnered women aged 15-49 years, prevalence of lifetime experience of physical IPV was 28.2%. The significant predictors for physical IPV were previous experience of psychological abuse (adjusted OR: 4.71; 95% CI: 3.236.85); sexual abuse (aOR: 5.18; 3.21-8.36); having attitudes supportive of IPV (aOR: 1.75; 1.2-2.4); partner’s daily alcohol consumption (aOR: 2.85; 1.50-5.41); and previous engagement in a physical fight (aOR: 3.49; 1.87-6.50). Community based IPV prevention programmes targeted at breaking the cycle of abuse, transforming gender norms which support IPV and reducing alcohol consumption should be developed (Afr J Reprod Health 2012; 16[1]:43-53). Résumé La violence causée par le partenaire intime (VCPI) est répandue au Nigéria, mais il existe une culture de silence, ce qui le rend difficile à identifier les femmes en danger. A travers une étude descriptive transversale, nous avons déterminé la prévalence et les indices de la VCPI physique au sein d’une communauté à faible revenu ayant une densité bien élevée au sud-ouest du Nigéria. Parmi les 924 interviews recueillies auprès de femmes âgées de 15 à 49 ans qui ont eu des partenaires dans le passé, la prévalence d’une expérience de vie de la VCPI était de 28,2%. Les indices significatifs pour les VCPI étaient l’expérience antérieure de d’un abus psychologique (OR : 5,18) et ayant des attitudes qui soutiennent la VCPI (OR : 1,75), la consommation quotidienne d’alcool par le partenaire (OR : 22,85) et l’engagement dans le passé dans un combat physique. Il faut élaborer des programmes de prévention de la VCPI basées sur la communauté et qui cherchent à rompre le cycle d’abus, à transformer les normes des sexes qui soutiennent la VCPI et à réduire la consommation d’alcool (Afr J Reprod Health 2012; 16[1]:43-53). Keywords: Intimate partner violence, women, predictors of physical violence, urban community, south west Nigeria Introduction Intimate Partner Violence (IPV) has in the last few decades become a public health issue of immense significance all over the world. Such violence has been associated with serious health consequences including physical, sexual and reproductive health, psychological and behavioural problems, as well and maternal mortality.1-3 According to the World Health Report on Violence and Health, “IPV refers to any behaviour within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship”.2 IPV can take a variety of forms including physical assault such as hits, slaps, kicks, and beatings; psychological abuse, such as constant belittling, intimidation, and humiliation; and coercive sex. It frequently includes controlling behaviours such as isolating a woman from family and friends, monitoring her movements, and restricting her access to resources.2,4 Although both men and women assume either role of victim or perpetrator, females are usually the victims in male-dominated patriarchal societies with less gender equality like Nigeria, while higher levels of male IPV victimization occur in countries with greater gender equality.5 Population-based studies from various countries indicate that between 10% and 75% of women report that an intimate partner has physically abused them at least once in their lifetime. The lowest figures of 10% were reported in Paraguay and Philippines while the highest prevalence rates were recorded in Bangladesh.2,4,6-8 Overall, at least 1 in 3 of the world’s female population has been physically or sexually abused by a man or men at some time in their life.4 Research has shown that physical abuse is often associated with psychological or emotional, and sexual abuse.9 Various risk factors for IPV have been extensively reported in literature. In broad terms, they can be classified as individual, partner, couple and societal characteristics. At the level of the individual (victim), it has been reported that young women and those below the poverty line are disproportionately affected.9-11 Low socioeconomic status has also been identified as a risk factor for IPV.12 Women who contribute a greater proportion to the family income have been identified to be at risk, possibly because the woman’s economic power questions the man’s role as provider.13-15 In Nigeria, Fawole and colleagues who studied both male and female civil servants found that being young, unmarried and having a history of parental violence in the partner were significantly associated with a woman being a victim to IPV.16 On the part of the perpetrator, men who abused alcohol and other psychoactive substances were more likely than those who did not abuse alcohol to perpetrate IPV.17 Witnessing parental violence or being a victim of physical violence as a child has also been associated with men who perpetrate IPV.16,18,19 Women who were exposed to childhood violence and witnessed domestic violence are at higher risk of being victims.11 At the level of the couple, dysfunctional, unhealthy relationships characterized by inequality, power imbalance and conflict can lead to IPV.20 IPV is reportedly associated with gender inequality as well as social norms supportive of traditional gender roles, and patriarchal male dominance. Similarly, the lack of institutional support from police and judicial systems and weak community sanctions are other factors known to be associated with IPV.11 Although IPV has been thoroughly researched and widely published on the global scene, this cannot be said of Nigeria. A few Nigerian researchers have provided information on prevalence and attitudes to IPV, 16, 21-23 but data is particularly sparse on the factors predisposing women to physical IPV. This study sought to bridge this information gap by determining the prevalence of physical violence and the factors predisposing women in a low-income community in south west Nigeria to IPV. Methods Setting The study was conducted in Idikan, a densely populated low-income urban community in Ibadan, a large indigenous city located in the south western part of Nigeria. Ibadan is comprised of three well demarcated socio-economic zones namely the inner city consisting of the traditional lower socioeconomic communities; the transitional middle socio-economic zone and the sub-urban periphery higher socio-economic zone. Idikan community is located in the inner core zone and its residents are mainly of Yoruba ethnicity and are engaged in petty trading, subsistence farming and artisanship occupations.24 The estimated population of females aged 15 years and older in 2007 was 3421 based on the projection of the 1999 enumeration figures of 2870 25 and the national average annual growth rate of 2.4% between 2002 and 2008.26 Study design and sampling technique Using a descriptive cross-sectional design, this community-based survey involved interviewing women aged 15-49 years during the 4-month period of data collection in 2007. The sample size was calculated from the expression: N= Z2(100p)p/d2. Where Z is a standard normal deviate, set at 1.96. The confidence level was specified as 95% and the tolerable error margin (d) was 5%. The p is the estimated proportion of respondents with the outcome attribute. There was no previously documented estimate of physical IPV from community based studies in Nigeria so an estimate of 50% was used. A design effect of two was applied to cater for the homogeneity of the population since the cluster sampling strategy was employed. Therefore the minimum estimated sample size was 386 x 2 = 772. This was increased to 869 to compensate for 10% nonresponse to certain questions. In all, 924 women were recruited to participate in the study. The Idikan community is divided into two approximately homogenous halves by a major road that runs through the community. Each half consists of compounds made up of households. Clusters were defined as compounds and all the clusters in the randomly selected half of the community were visited. Women were interviewed either at home or in their workplace, for those who worked near their homes. Instrument and Data collection A modified version of the questionnaire used for the WHO Multi-Country Study on Women’s Health and Domestic Violence was used to collect the data for this study. The instrument obtained information on the respondents’ social and demographic characteristics, reproductive health, characteristics of current/most recent partners; attitudes towards gender roles and intimate partner violence; experience of IPV, injuries due to violence; impact and coping mechanisms used by women who experienced violence; childhood sexual abuse experiences; and financial autonomy. 27 Information was also obtained regarding partners’ use of psychoactive substances including alcohol and the occurrence of family and financial problems as a result of alcohol consumption. The women’s attitudes towards IPV were assessed by asking respondents if it was justifiable for a husband/partner to physically abuse a woman in one or more of the following situations (1) if she does not complete the housework to his satisfaction Interviews were conducted by two trained married female interviewers, either in English or Yoruba, depending on which language the respondent was most conversant with. Data Analysis Data gathered was entered into and analyzed with SPSS 16.0 software.28 Frequency tables were generated and bivariate analysis done. Summary statistics were used to present quantitative variables while Chi square (χ2) test was used to determine associations between categorical variables. Multivariate logistic regression was used to identify predictors for physical violence. Outcome Measures Attitudes supportive of IPV A positive response to any of the reasons justifying wife beating indicated that the respondent was supportive of physical IPV. Experiences of IPV Women whose partners exhibited any of the behaviours below were considered to have experienced psychological IPV: A woman was considered to have experienced physical violence if she said “yes” when asked if a current or past partner ever abused her in any of the following ways: a) Slapped you or threw something at you that
could hurt you? Sexual violence was considered to have occurred if the woman reported any of the following: a) Was physically forced to have sexual
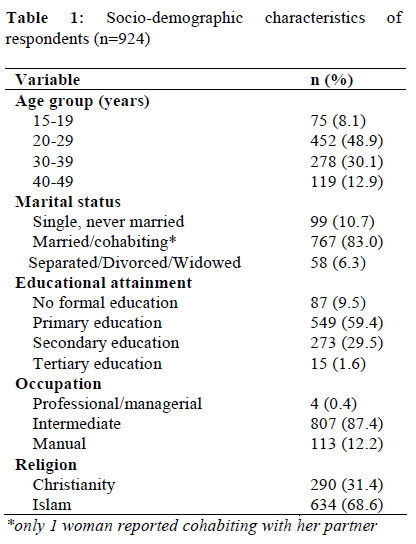
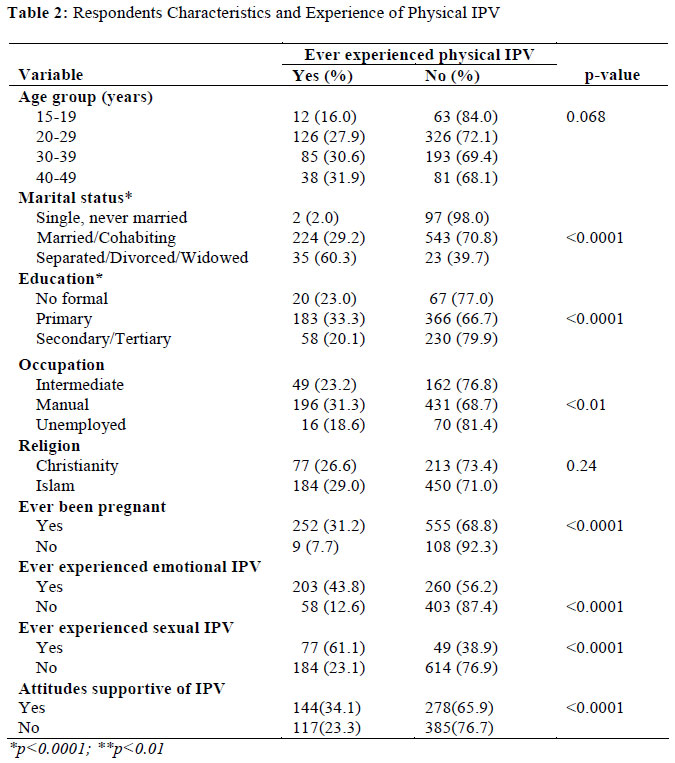
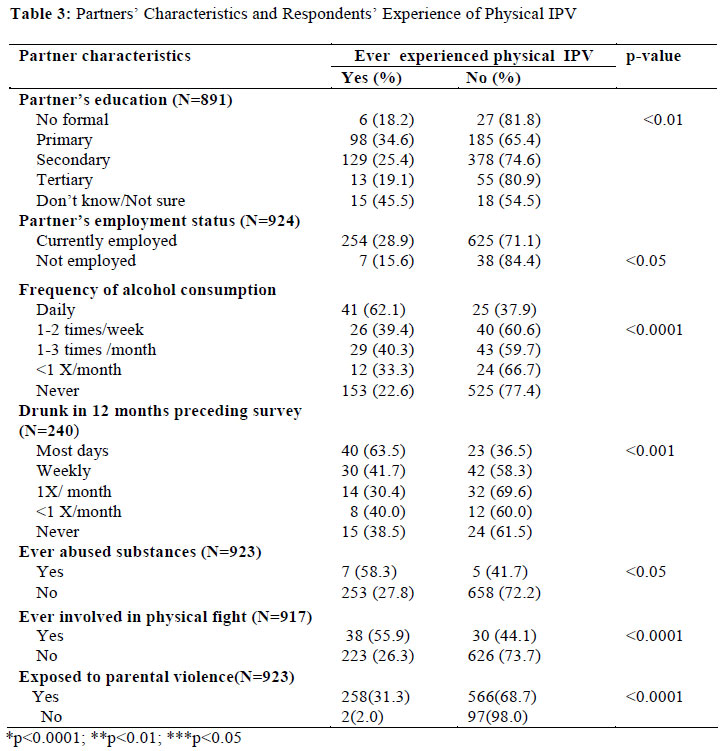
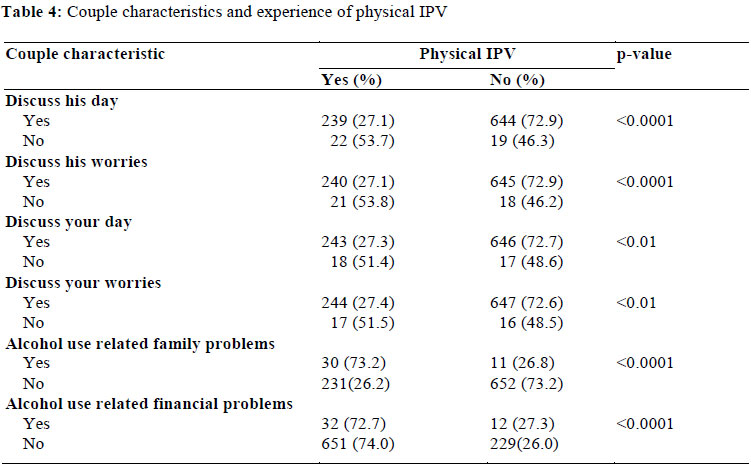
intercourse when she did not want to Ethical considerations Verbal informed consent was obtained from all participants. The interviews were conducted in quiet and secluded areas to provide privacy for the respondents. Confidentiality was maintained and ethical approval to conduct the study was obtained from the Oyo State Ministry of Health Ethical Review Committee. A total of 924 ever-partnered women aged 15-49 years consented to participate in the study out of 937 who were approached, giving a response rate of 98.6%. The mean age of the respondents was 29.1 ± 8.1 years and the women had an average of 8.2 ± 3.6 years of schooling, with 90.5% having received some formal education. Majority (83.0%) of the respondents were either currently married or cohabiting with a man, 87.4% of women were engaged in intermediate occupations such as trading, hairdressing and dress making. Details of these and other socio-demographic details are shown in Table 1. Majority, 807 (87.3%) of women had been pregnant before and the median number of living children was 2 (range 1-12). Partners of the women were aged 16 to 80 years with a mean age of 36.0 ±10.8 years and had schooled for an average of 10.2 ± 3.4 years. Respondents reported that 879 (95.1%) of their partners were employed at the time of data collection. In all, 678 (73.9%) partners were reported to have never consumed alcohol and 66 (7.2%) male partners consumed alcohol daily. Among the 240 men who had ever consumed alcohol, 65 (26.2%) were reported to have been drunk on most days in the 12-month period preceding the interview. Prevalence of lifetime experience of physical IPV among these ever-partnered women was 28.2%, the main types of physical violence experienced were slaps (27.2%), being kicked (14.4%) and being hit (13.4%). Similarly, 50.1% and 13.6% respectively had ever experienced psychological and sexual abuse. Overall, 550 (59.5%) had ever experienced any form of IPV. As shown in Table 2, significantly higher proportions of those: who were separated/divorced /widowed (60.3%, p<0.0001); who had only primary level education (33.3%, p<0.0001); engaged in manual occupations (31.3%, p<0.01); had ever been pregnant (31.2%, p<0.0001); had attitudes supportive of IPV (34.1%, p<0.001); had ever experienced psychological (43.8%, p<0.0001) or sexual IPV (61.1%,p<0.0001) had experienced physical IPV. There was no statistically significant relationship between religion or age and ever experiencing physical IPV. The main partner characteristics significantly associated with physical IPV included daily alcohol consumption (62.1%, p<0.0001), being drunk on most days in the preceding 12 months (63.5%, p<0.0001), previous abuse of psychoactive substances (58.3%, p<0.05), previous involvement in a physical fight (55.9%, p<0.0001) and exposure to parental violence (31.3%, p<0.0001) (Table 3). The associations between the characteristics of the couples’ relationship and occurrence of physical IPV are shown in Table 4. Significantly higher proportions of women in relationships in which issues about their daily activities and worries were not discussed by the couple experienced physical IPV when compared with those in relationships who did discuss these issues (72.7% versus 51.4%, p<0.01). Similarly, women who reportedly had family and financial problems associated with partners’ alcohol use were more likely than those who did not report those problems to have ever experienced physical IPV (73.2% vs 26.2% and 72.7% vs 74.0% respectively, p<0.0001). Following binary logistic regression, individual characteristics found to increase the risk of physical IPV included having ever experienced psychological (aOR 4.71 95%CI 3.23-6.85, p<0.0001) and sexual (aOR 5.18 95%CI -8.36, p<0.0001) IPV. Those who had attitudes supportive of IPV were also more likely to experience physical violence (aOR 1.75 95%CI 1.2-2.4, p=0.001). Women who were single were less likely than those who were separated/divorced/widowed to report ever being physically abused. Partner characteristics such as daily alcohol consumption and ever being involved in a physical fight were associated with an increased risk of physical IPV (Table 5). Discussion Our findings on prevalence of physical IPV are comparable to those from the most recent Nigeria Demographic and Health Survey29 , studies by other Nigerian researchers,16,23 as well as research conducted in South Africa and among Latina women living in the US.30,31 The prevalence of physical IPV in the current study, however, is higher than rate reported by the authors in another community in the same city.21 This might be explained by some differences in the cultural norms in the study population as the study was conducted among migrant women from the northern part of the country, who were mainly of Hausa ethnicity. However, the study of the migrant women reported a higher prevalence of psychological violence than was found in this study.21 In keeping with previously published research,9,32 women in the present study who had experienced physical IPV were more likely to have experienced psychological and sexual violence when compared with their counterparts who had not experienced physical IPV. Studies from South Africa and Russia report the “normalization” of physical and sexual violence in these societies and the use of such violence as an acceptable means of conflict management within the home.33-36 Cultural justifications for violence are often made in various settings in many countries around the world, usually following from traditional notions of the acceptable roles of men and women. Reports from other low-income African countries which like Nigeria have patriarchal societies characterized by relations of power also show the ubiquitous nature of the perpetration and acceptance of IPV.37, 38 The prevalent attitudes supportive of IPV found in this study have also been documented by others conducted in south west Nigeria.16,21 IPV is widely condoned in many Nigerian societies where the belief that it is acceptable for the husband to chastise his wife is deeply embedded in the culture. As a result, women have been socialized to accept and sometimes to encourage physical abuse.39 Therefore, it is not surprising that the frequency of physical IPV in this study was higher among respondents who condoned it and this is probably due to the fact that it is acceptable to women within the context of their relationships. Consequently, the women would do little or nothing to redress the situation. However, these attitudes are often learned through family and community cultural processes which can be changed through appropriate health education intervention programmes. The risk of physical IPV was significantly lower among women who were married or had never been married compared to those who were of the physical IPV experienced, whereas the separated or divorced. This could be due to the single women may not have been in longstanding fact that the separated or divorced women may relationships which would have predisposed them have been forced to leave their marriages because to experiencing IPV. In keeping with our results, several researchers have found that women whose partners consumed alcohol frequently were at greater risk of physical IPV than their counterparts whose husbands did non consume alcohol. 9, 16,40 It is possible that the link between frequent alcohol consumption and IPV is due to the fact that alcohol is a disinhibitor which could create an atmosphere for arguments and disagreements which lead to violence.7 The results also indicated that partners’ of men who had a history of fighting with other men were more likely to experience physical IPV. This is similar to the reports of other African researchers which have indicated that men who used violence to solve problems in other settings were more likely to perpetrate IPV when compared with men who did not use violence to resolve conflicts.41,42 The cross-sectional design of this study is a limitation in gaining a full understanding of the factors associated with IPV, since studies of this nature do not allow for the establishment of temporality and determination of causality. Another limitation of this study is the likelihood that the experience of IPV was probably underreported by participants, perhaps due to the social acceptability of this malady in the Nigerian context, as well as protective factors such as the contribution of the extended family and other social networks in the resolution of marital conflicts. It must also be pointed out that we may have missed some women who reside in the selected clusters due to the fact that they are engaged in formal or informal work away from the community and were not available at home or in the marketplace during daylight hours. However, we consider such women to be in the minority and do not believe the results would be different, had we been able to track them down. Finally, the results of this study, though representative of this urban community in Nigeria, are not generalizable to the entire country. However, the findings may be applicable to other urban communities that are predominantly inhabited by indigenous Yoruba populations. Conclusion Prevalence of physical IPV in this population was high. Women at greatest risk of physical IPV in this study were those who had experienced psychological or sexual abuse, had attitudes supportive of IPV and those whose partners frequently consumed alcohol. Women who were currently married and those who had never been married were less likely than women who were currently separated/widowed/divorced to have ever experienced physical IPV. Reducing the prevalence of physical IPV in this setting would require community based intervention programmes targeted at addressing the intergenerational transfer of cultural norms which support traditional gender roles of male dominance and gender inequality. Reduction of IPV would require male as well as female liberation from these binding and deeply entrenched cultural norms through a multipronged and couple-centred approach. Reduction in alcohol consumption among the males should also be addressed. Efforts must be made to find culturally appropriate and innovative ways of introducing and implementing interventions to tackle IPV. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12005t1.jpg] [rh12005t2.jpg] [rh12005t5.jpg] [rh12005t4.jpg] [rh12005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}