 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 55-60 ORIGINAL RESEARCH ARTICLE Pregnant Women and Alcohol Use in the Bosomtwe District of the Ashanti Region-Ghana Femmes enceintes et l’usage de l’alcool dans le Disrict d’Ashanti Region, GhanaYaw Adusi-Poku1*, Anthony K Edusei2, Agartha A Bonney2, Harry Tagbor2, Emmanuel Nakua2 and Easmon Otupiri2 1District Health Directorate, Offinso North, Ashanti-Ghana; 2Department of Community Health, School of Medical Sciences, College of Health Sciences, KNUST, Ghana.
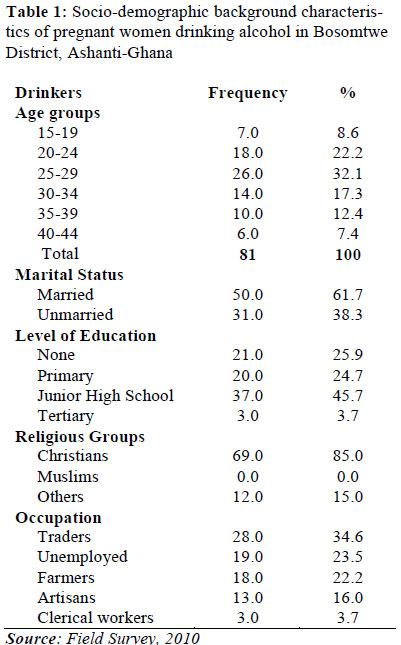
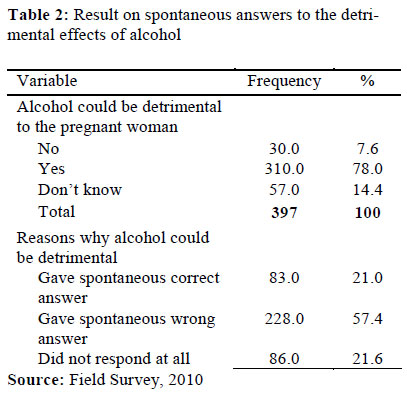
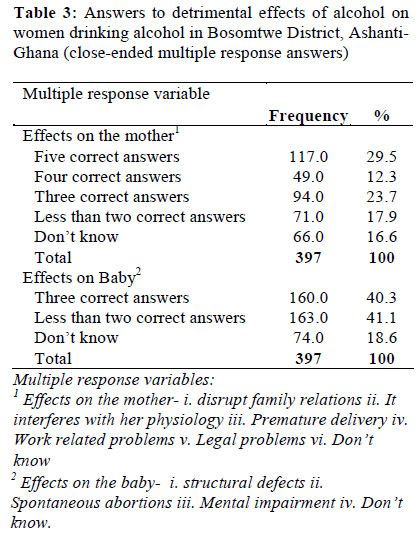
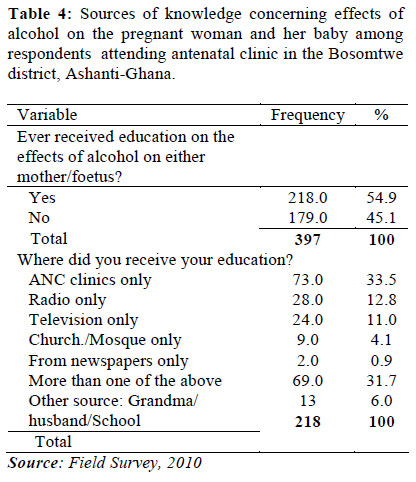
Code Number: rh12006 Abstract Drinking alcohol in pregnancy is a serious public health concern worldwide. This study sought to determine the magnitude and socio-demograhic characteristics of pregnant women attending Antenatal clinic in the Bosomtwe district, Ghana who drank alcohol and to assess their general knowledge about the effects of alcohol in pregnancy. The study, a descriptive cross-sectional, was conducted in all the ten health facilities providing reproductive health care with a sample size of 397 pregnant women using structured questionnaires. The findings of the study were that 20.4% of pregnant women drank alcohol. The 25-29 year group 26 (34.0%), married 50 (61.7%) and Junior High School Educated 37 (45.7%) as well as Christians 69 (85.0%) and traders 28 (34.6%) drank most. Majority 77 (33.5%) heard about the detrimental effects of alcohol at Antenatal Clinics (ANC). The District Health Management Team (DHMT) should strengthen health education on alcohol at ANC and through the radio as well as the DHMT collaborating with the Ghana Education Service to embark on education of school pupils and students on the harmful effects of alcohol in pregnancy (Afr J Reprod Health 2012; 16[1]:55-60). Résumé La consommation de l’alcool pendant la grossesse est un gros problème de santé publique partout dans le monde. Cette étude a cherché à déterminer l’ampleur et les caractéristiques sociodémographiques des femmes enceintes qui fréquentent la clinique prénatale qui consomment l’alcool et à évaluer leur connaissance générale sur l’effet de l’alcool dans la grossesse. L’étude, qui est descriptive et transversale, a été menée auprès de dix établissements de santé qui assurent des services de santé de la reproduction à l’aide d’un échantillon de 397 femmes enceintes à travers des questionnaires structurés. Les résultats de l’étude révélaient que 24% des femmes enceintes buvaient de l’alcool. Le groupe des femmes qui ont 25 – 29 ans, 26 (34,0%) mariées, 50(61, 7%) et celles qui sont scolarisées jusqu'au niveau du collège 37 (45,7%) aussi bien que les chrétiennes 69(85,0) et les marchandes 28 (34,6%) buvaient le plus. La majorité ,77 (33,5%) a appris les effets nuisibles de l’alcool aux cliniques anténatales (CAN). Le District Health Management Team (DHMT) doit renforcer l’éducation sanitaire sur l’alcool dans les CAN et à travers la radio et le DHMT doit collaborer avec le Ghana Education Service pour commencer la sensibilisation des élèves et des étudiants concernant les effets nuisibles de l’alcool pendant la grossesse (Afr J Reprod Health 2012; 16[1]:55-60). Keywords: Reproductive years, Alcohol consumption, Foetal Alcohol Syndrome, Ghana, Women, Pregnancy Introduction Although the existence of alcohol – induced foetal damage is well established, it has been reported that, some 6 to 20 % of a cohort of women drank alcohol ‘heavily’ during pregnancy.1 A study conducted by Ho and Jacquemard2 revealed that over a quarter of the women drank alcohol throughout pregnancy. Alcohol has profound effects on an unborn baby by a mother who drinks. It is evident that a mother does not have to be an alcoholic to expose her unborn baby to the harmful effects of alcohol during pregnancy. In other words, no amount of alcohol use during pregnancy has been proven safe.3 It also has effects on the mother. The detrimental effect of alcohol is much more pronounced on the foetus. The severest effect of alcohol on the foetus is a constellation of variable physical and cognitive abnormalities called Foetal Alcohol Syndrome (FAS) whilst if it is less severe, it is referred to as Foetal Alcohol Effects (FAE). The unfortunate child basically, can be identified by small stature and a typical set of facial traits including small head (microcephaly), small eyes (microphthalmia), short palpebral fissures, epicanthal folds, a small or flat mid - face, a flat elongated philtrum, a thin upper lip, and a small chin. Abnormal palmar creases, heart defects, and joint contractures may also be evident. After birth, cognitive deficits become apparent. The most serious manifestation is severe intellectual disability, thought to be a teratogenic effect.4 The present study was informed by anecdotal claims of alcohol ingestion in the reproductive years in the Bosomtwe District of the Ashanti region of Ghana. There were claims that Lake Bosomtwe, the largest natural lake in Ghana, which is situated in the Amakom subdistrict provided a conduit for alcohol ingestion. Numerous hotels and rest houses are scattered all around the lake. A lot of social activities such as alcohol drinking take place in this area. It was also allerged that women took unstandardised locally brewed alcohols such as akpeteshie, pito but there was lack of data to support these claims. Also, what informed this research was the prevalence of “ASRAM” among our rural communities. The word “Asram” is a commonly used term in Ghana which applies loosely to any child born with cognitive or physical defects. Initially, the babies are small for gestational age and have difficulty in surviving. People attribute “Asram” to an “evil eye” cast on the mother during the period of pregnancy. Some mothers hide their pregnancies from people they believe could harm the foetus who transfer “Asram” by spiritual means. Could drinking alcohol in pregnancy be associated with “Asram”? It may be that foetal Alcohol Syndrome may clearly be what is being referred to as “Asram” The study sought to determine the magnitude and socio-demograhic characteristics of pregnant women attending Antenatal Clinic in the Bosomtwe district who drank alcohol and their general knowledge about the effects of alcohol in pregnancy. This would help plan intervention programmes and inform policy makers about the need and urgency to pass the Mental Health Bill in Ghana. Again by determining the magnitude of women who drank alcohol, it would be recommended for a prospective study to investigate the effects of alcohol on the foetus. Methods The study was conducted in all the 10 health facilities providing reproductive health care in the Bosomtwe district within the period of July and October, 2010 after ethical approval from the Committee on Human Research Publication and Ethics (CHRPE), School of Medical Sciences, SMS, of the Kwame Nkrumah University of Science and Technology, KNUST and the District Health Management Team (DHMT), Bosomtwe. All study participants gave their written consent prior to granting interviews. The study design was a descriptive crosssectional and sample size was calculated to be 385 with a 5% non-response rate, totalling 401. This was to detect a 50% prevalence of pregnant women who drank alcohol at 95% confidence interval. An interviewer -administered questionnaire was administered to pregnant women attending antenatal care clinics. Four persons did not consent to being interviewed leaving 397 pregnant women who responded to the questionnaire. The inclusion criteria were: confirmed pregnancy at any gestation and parity as well as consumers of alcoholic base between 4 to 60 % to include most of the alcoholic beverages used world -wide. Pregnant women who were severely ill or who consumed alcoholic tinctures, syrups or sips of church wine were excluded from the study. At a facility where the number of registrants for ANC was larger than the quota allotted based on the expected pregnancies, Systematic Random Sampling method was used. By this method, the number of registrants for a particular facility was compared to the expected pregnancies for that facility’s catchment area in 2010. If the number of registrants was found to be larger, systematic random sampling was used. For example, at St. Michael’s hospital where the total registrants exceeded the quota for the study, the sampling interval, K was determined; K= N/n, where: N=Expected pregnancies for the year, 2010 n= Sample size This implied that every Kth person was interviewed. Then the starting point, say, X was determined using simple random sampling by balloting for the registrant between 1 and the Kth person inclusive. Pregnant women were then interviewed in the manner as follows: X, X+K, X+2K and so on until the required number was achieved. However, in other facilities where the number was few; all the pregnant women who were willing to participate were included. Data was collected using structured questionnaire with open and close ended questions which bordered on their socio-demographic characteristics and general effects of alcohol on the mother and the foetus as well as where these pregnant women received their education about the general effects of alcohol if any. Data were entered into EpiData (version 3.1) software 5 and analysed in STATA (version 10).6 Pretesting was done prior to the study at Foase, a nearby district. Measurements included means, proportions and percentages. Results The total number of pregnant women interviewed was three hundred and ninety-seven (397.0). Those responding ‘yes’ to alcohol were 81.0. Hence the magnitude of alcohol drinkers was 20.4%. The socio-demographic characteristics (Table 1) were as follows: the highest drinking age group was found among the 25-29 years. The least drinking group was the 40-44 year-olds. Married women drank most (61.7%). With respect to level of education, those who had completed Junior High School drank most (45.7 %) followed in about equal proportions by those who had never had any formal education (25.9 %) and those whose education ended at the primary level (24.7 %). Tertiary -educated women drank least (3.7%). Majority of drinkers were traders (34.6%). The unemployed and farmers followed in almost equal proportions – 23.0%. Again, of the 397 respondents (Table 2), 7.6% said alcohol had beneficial effects during pregnancy compared to 78.0% who said alcohol could be harmful. More than two-thirds -57.4% of these 78.0% gave spontaneous wrong answers when asked to mention some detrimental effects of alcohol in pregnancy. In the ensuing close-ended multiple response-answers (Table 3) about the effects of alcohol on the mother, 83.4% gave at least one or more answers whilst 16.6% did not know at all. The result was not quite different from the effects of alcohol on the foetus; 81.4% gave at least one correct answer and 18.6% did not know. About fifty-five percent (54.9%) of the respondents received education on the detrimental effects of alcohol in pregnancy (Table 4). Majority of these (33.5 %) received this education at Antenatal Clinics only; followed by radio/ television only (12.8%; 11.0% respectively). The least respondents were those who received their education via newspapers only (0.9 %). Discussion The magnitude of pregnant women consuming alcohol was 20.4% and the age group with the highest number of drinkers was 20-29 year group. This was high compared to other studies done in the United States/Canada. For example, the study by the Behavioural Risk Factor Surveillance System (BRFSS), in the U.S.A as reported by Sullivan7 found that the prevalence of pregnant women who drank at least once, during pregnancy was 12.0%. In Canada, the prevalence was 5.8 %.8 However, the age group with the highest drinkers was similar to the findings by the Institute of Alcohol Studies9 that most alcoholic beverage drinkers were in their 20’s and 30’s. The highest numbers of alcoholic beverage drinkers were married (61.7%) but with respect to the level of education, the highest percentage was those with junior high education (about 46.0%). This result differs from the study in the U.S by BRFSS that alcoholic beverage in pregnant women in the U.S.A was highest among collegeeducated women, and the unmarried.7 This finding somehow reflects the cultural differences and the level of education among the different populations where these two studies were conducted. In the district where this current study took place, a married woman must appear to be living an improved lifestyle and this must be seen by her deliberately putting on weight and a change in the tone of the skin colour (by bleaching the skin). With respect to weight gain, alcohol is taken to boost appetite. Again, the findings of the study showed that of the 397 respondents, 7.6% said alcohol had beneficial effects during pregnancy. They did not agree that alcohol could have harmful effects except when taken in large quantities. These respondents were of the view that alcohol acted as a relaxant to reduce stress, it ‘cleaned’ the baby in the womb or acted as an appetizer. This finding was no different from a similar study by Peadon and others10, in which 7.3% of pregnant women did not agree that drinking alcohol during pregnancy could harm the unborn child. Furthermore, of those (78.0%) who responded that alcohol had harmful effects in pregnancy, more than two –third of them (57.0%) did not actually know the possible harm that alcohol could cause on pregnancy as they gave wrong answers compared to one-third (21.0%) who gave correct answers to open -ended questions. This is consistent with a larger study (national survey) conducted in Canada11 on women in their reproductive years on the awareness of the effects of alcohol use during pregnancy and foetal alcohol Syndrome; 71.0% knew alcohol could be harmful in pregnancy but did not really know what the effects really were The relatively poor spontaneous correct responses about specific harmful effects of alcohol could have stemmed from the non-formal education of some of the respondents. About a quarter of all those interviewed (25.9%) had no formal education. Hence except through radio discussions or through oral education in the local language, education of harmful effects of alcohol through formal education would be difficult. In the ensuing close-ended multiple responseanswers about the effects of alcohol on the mother (Table 3), 83.4% gave at least one or more answers whilst 16.6% did not know at all. The result was not quite different from the effects of alcohol on the foetus; 81.4% gave at least one correct answer and 18.6% did not know. This result is consistent with a similar result of the study by the national alcohol survey conducted in Canada11 that put at least 89.0% of the respondents believing that alcohol could cause life-long disability in the child and also some effects on the mother. About 35.0% of the respondents had received previous education on the detrimental effects of alcohol at ANC (oral education), followed by radio/television (about 12.0%). In contrast to a more literate society such as Canada, 72.0% had received previous education about the detrimental effects of alcohol; (33.0%) rather received their education through pamphlets/brochures/. Smaller numbers mentioned television advertising (24.0%), a doctor or healthcare professional (20.0%), books (15.0%), a poster (12.0%), magazine advertising (11.0%), infant care groups/classes (6.0%), and personal experience/ word of mouth (5.0%).11 Conclusion There was high illiteracy (about 45.0%, refer Table 4) among pregnant women about the knowledge of the detrimental effects of alcohol on either the pregnant woman or on the baby. Since most of the respondents received their education at antenatal clinics and through the radio, all efforts must be made by the District Health Management Team (DHMT) to strengthen the health education through these channels which is easy to deliver in rural settings. The DHMT must also liaise with the churches, mosques and the prayer camps for this health education to be effective. It is also recommended that prospective studies be conducted on alcohol consumption in pregnancy among this percentage of women who drink to determine the true effects of alcohol on the foetus in the Bosomtwe district. Further studies to determine a nation -wide prevalence is recommended for appropriate action to be taken by the reproductive unit of the Ghana Health Service/Ministry of Health, Ghana. Antenatal care services across Africa offer health education in the form of talks generally before the antenatal sessions and this avenue could be employed to educate pregnant women on the African continent. Acknowledgements The author wishes to acknowledge the District Health Management Team, the Medical Superintendent and staff of the Reproductive and Child Health of all the ANC clinics at the Bosomtwe District. I am also indebted to all the pregnant women who voluntarily contributed to the study; without them the study would not have been possible. My appreciation goes to Gabby, Mariam, Mr. Addai-Donkor and Dr. (Mrs) Gifty Antwi all of the Department of Community Health, KNUST and to Mr. Kofi Poku and Alhaji Ibn Ibrahim at the Regional Health Administration, Ashanti. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12006t4.jpg] [rh12006t3.jpg] [rh12006t2.jpg] [rh12006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}