 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
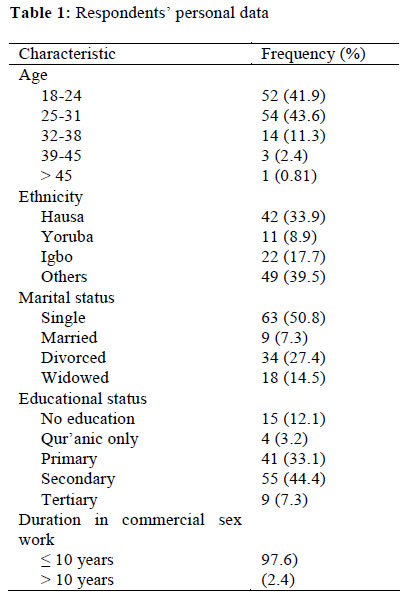
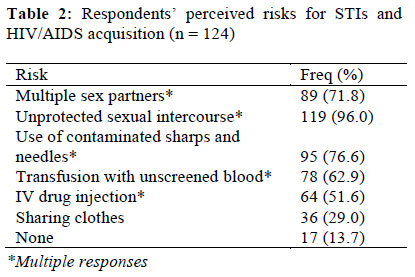
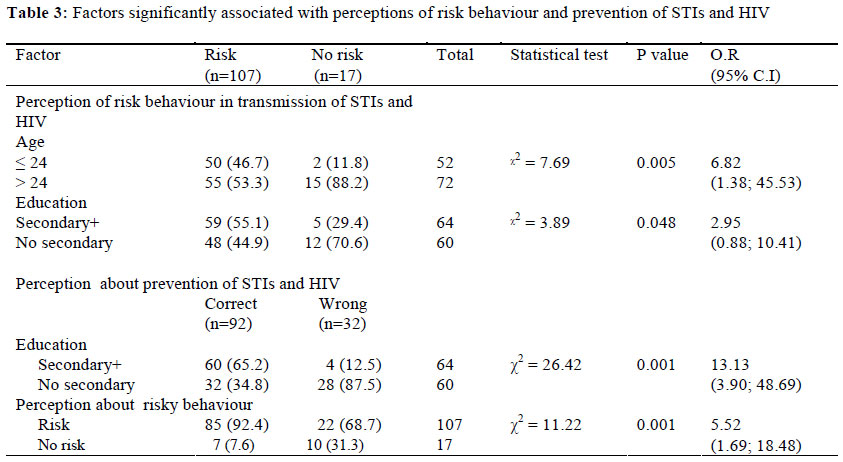
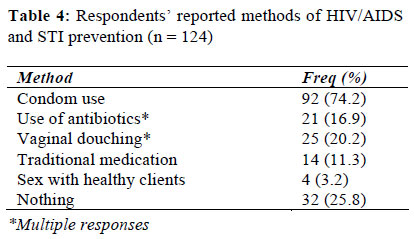
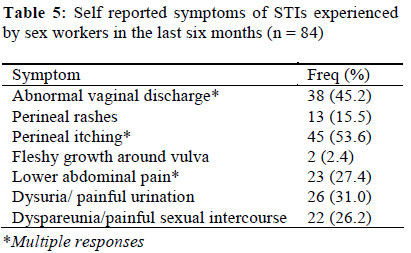
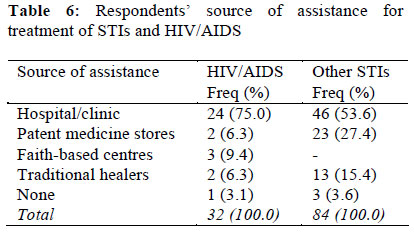
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 61-67 ORIGINAL RESEARCH ARTICLE Risk Perceptions, Prevention and Treatment Seeking for Sexually Transmitted Infections and HIV/AIDS among Female Sex Workers in Kano, Nigeria Perceptions de risque, prévention et recherche du traitement pour les infections sexuellement transmissibles chez les prostituées à Kano, NigériaLawan UM,1* Abubakar S1 and Aisha Ahmed2 1Department of Community Medicine, Bayero University and Aminu Kano Teaching Hospital, Kano State, Nigeria; Code Number: rh12007 Abstract We examined the risk perceptions, prevention and treatment seeking for HIV/AIDS/STIs of 124 female commercial sex workers from 52 randomly selected brothels in Kano, Nigeria using a descriptive cross sectional design. We analysed the data using Epi Info® 3.5.1. The mean age of the sex workers was 26.4 ± 1.9 years, and most were indigenous Hausas (33.9%), single (50.8%) and had at least secondary school level of education (51.7%). Majority perceived that unprotected sexual intercourse (96.0%) is the commonest risk factor associated with STIs and HIV/AIDs acquisition. Surprisingly, 25.8% did not believe that any method protect against STIs and HIV/AIDS. The most common symptom reported was perineal itching (53.6%); and 60.7% with the symptoms continued to have unprotected sex. Alarmingly, 29.6% of the sex workers were HIV positive, and all continued with unprotected sexual intercourse with clients. Despite the sex workers’ good perception and knowledge of HIV/AIDS/STIs prevention, they demonstrated unhealthy sex behaviour and treatment seeking. We recommend a peer education package that targets the workers and their clients, with focus on reducing risk behaviours associated with STIs and HIV transmission, safer sex; and treatment seeking (Afr J Reprod Health 2012; 16[1]:61-67). Résumé Nous avons fait une étude sur les perceptions, la prévention et la recherche du traitement pour le VIH/SIDA/IST chez 124 prostituées sélectionnées au hasard auprès des 52 maisons closes à Kano, Nigéria, à l’aide d’un modèle transversal descriptif. Nous avons fait l’analyse à l’aide de l’Epi Info*3.5.1. L’âge moyen des prostituées était de 26,4±1, ans et la plupart étaient d’origine haoussa (33,9%), célibataires (50,8%) et elles ont été scolarisées jusqu’au niveau secondaire (51,7%). La majorité d’entre elles ont perçu que le rapport sexuel non protégé (96,0%) constitue le facteur de risque le plus commun qui est lié aux IST et à l’acquis du VIH/SIDA. Etonnamment, 25,8% ne croyaient pas qu’aucun méthode ne protège contre les IST et le VIH /SIDA. Les 60,7% qui avaient le symptôme ont continué à avoir des rapports sexuels non protégés. Fait alarmant, 29,6% des prostituées étaient séropositives et elles ont toutes constitué à avoir des rapports sexuels non protégés avec leurs clients. Malgré la bonne perception et la connaissance qu’avaient les prostituées de la prévention du VIH/SIDA, elles ont fait preuve d’un comportement sexuel et la recherche du traitement malsain. Nous préconisons un programme d’éducation de pairs qui vise les prostituées et leurs clients en vue de réduire les comportements de risque liés aux IST et à la transmission du VIH, aux rapports sexuels moins dangereux et à la recherche du traitement (Afr J Reprod Health 2012; 16[1]:61-67). Keywords: HIV/AIDS, STIs, Female Commercial Sex Workers, Perceptions, Northern Nigeria Introduction The number of young females engaged in sex business is increasing by day especially in the sub-Saharan African countries bewildered by problems associated with urbanisation and pressure from poverty, food and political insecurity; and civil unrest. Commercial sex workers constitute one of the high risk groups for sexually transmitted infections (STIs) and human immune deficiency virus infection (HIV/AIDS) acquisition and transmission.1 This is perhaps because sex workers have numerous sex partners and they engage in unprotected sex and other forms of sex that cause contact with body fluids of a partner who may be infected with sexually transmitted diseases.2-4 STIs are infections that are spread primarily through person-to-person contact. More than 30 bacteria, viruses and parasites are transmitted sexually.5 The WHO estimates that 340 million new cases of curable STIs occur annually throughout the world in adults aged 15-49 years; and in developing countries, STIs and their complications rank among the top five disease categories for which adults seek health care. The presence of an untreated STI increases the risk of both acquisition and transmission of HIV by a factor of up to 10.5 HIV and STIs prevalence among female sex workers in sub-Saharan Africa varies widely, but in some countries it is more than 20 times higher than the HIV prevalence of the general population2,6,7 Thus, prevention and prompt treatment of STIs is important for preventing HIV in people at high risk, as well as in the general population. Many commercial sex workers come from disadvantaged backgrounds, are poorly educated and lack the skills and resources for other types of formal or non-formal employment. The risk for STIs and HIV in this group is a manifestation of their extraordinary social or economic vulnerability, which is expressed in their willingness to adopt high risk sexual behaviour. This underlying vulnerability is more often due to gender-based inequality, insufficient STIs and HIV information, and prevention commodities; and perhaps limited access to health and other social services because of stigmatization and marginalization. Therefore, controlling the spread of STIs and HIV among this vulnerable group and the general population will remain a mirage if the sex workers are not empowered to negotiate safer sex at all times. Substantial evidence from sub-Saharan Africa shows that the risk of HIV infection is lower among sex workers that use condom consistently.8,9 However, this is only possible if the sex workers are able to appreciate the risks associated with unprotected sex, and are also empowered to negotiate safer sex at all cost. This study investigates the perceptions about the risk and prevention of STIs and HIV/AIDS, the prevalence of STIs and HIV/AIDS; and the ways female sex workers operating in Kano handle such infections. We hope that our findings will provide evidence that will assist in designing more targeted STIs and HIV/AIDS interventions for this vulnerable group and their clients; as well as highlight the need for more research in this area. Methods Kano State is located in north western Nigeria and is one of the oldest and largest states in the country, and perhaps also the most traditional. Commerce and agricultural production have been the backbone of the Kano economy. Islam is the dominant religion, though there are significant groups of Christians. Urban drift from rural areas within Kano, from other states in Nigeria and from West Africa has provided a steady stream of migrants adding to Kano’s growing population. Kano is therefore a cosmopolitan melting pot of people. Majority of the residents are traders, civil servants, farmers and students. The study was carried out among brothel-based female commercial sex workers in Sabon-Gari of Fagge Local Government Area (L.G.A). Fagge is one of the eight metropolitan L.G.As that make up the Metropolis of Kano state. Sabon-Gari was originally a settlement of strangers located in Fagge, an outskirts of the old Kano city. Over time, the small settlement grew and eventually housed a diversity of people from all parts of Nigeria and to a lesser extent from other parts of West Africa. Today, Sabon -Gari is one of the three districts of Fagge L.G.A, and is predominantly inhabited by people from Southern Nigeria. According to the 2006 National population census, Fagge L.G.A had an estimated population of 198,828 out of the 9,383,682 people in Kano state.10 With the pronouncement of Sharia law in the northern states of Nigeria including Kano State, Sabon–Gari, a predominant non Muslim settlement became the seat of officially forbidden activities like alcohol consumption, gambling and prostitution.11,12 We used a descriptive, cross-sectional study design for this study. A sample of 124 commercial sex workers was used for the study, and this was determined using the formula for estimating sample size for descriptive studies;13 and 1.6% prevalence of higher-risk sexual intercourse among women who had sexual intercourse within the last 12 months of a survey in northwestern Nigeria.14 We identified 52 brothels in Sabon–Gari using unofficial networks of commercial sex workers, and selected the respondents using multistage sampling technique. In the first stage, 11 brothels were randomly selected from the 52 by drawing lots. In the second stage, from each of the selected brothels, the rooms therein were counted, and eleven (11) were selected by systematic sampling method using a sampling interval obtained by dividing the number of rooms in each of the brothels by the required number of rooms (11 rooms). Finally, a commercial sex worker was interviewed from each of the selected rooms, and where there were two or more residents in a room, one sex worker was selected by drawing lots. Three trained interviewers administered the pre-tested questionnaire that contained open and closed-ended questions. The questions were designed to elicit the socio-demographic characteristics of the respondents, their perceptions about risks of STIs transmission, as well as the prevalence, prevention and treatment seeking for STIs and HIV/AIDS by the commercial sex workers. The questionnaire was pretested in a different L.G.A other than that where the data was eventually collected. Some of the questions were rephrased for clarity based on observations made during pre-testing. Informed consent was obtained from prospective respondents before administering the questionnaire. Literate respondents indicated acceptance by signing the consent form, while non-literate participants affixed their thumbprint. Ethical clearance for the study was obtained from the Ethics Committee of Kano State Hospitals Management Board. Data collection was initiated and completed in May 2011. Data was analyzed using Epi Info® 3.5.1 statistical software package (CDC Atlanta, Georgia, USA). Quantitative variables were summarized using appropriate measures of location and variability, whereas categorical variables were presented as frequencies and percentages. The chi-square test was used to test for significant associations between categorical variables. P≤.05 was considered statistically significant. Results Socio-demographic profile of the respondents The mean age of the sex workers was 26.4 ± 1.9 years. Most (89.5%) were in the age group 18 to 31 years. The majority were indigenous Hausas (33.9%), single (50.8%) and had at least secondary school level of education (51.7%). Most of the sex workers (97.6%) were in the trade for 10 years or less (Table 1). The mean duration of the commercial sex workers in the sex business was 3.9 ± 3.4 years. Perceptions about risks and prevention of STIs and HIV/AIDS Majority of the sex workers perceived that unprotected sexual intercourse (96.0%), use of contaminated sharps and needles (76.6%), multiple sexual partners (71.8%) and transfusion with unscreened blood (62.9%) are the most common risks associated with STIs and HIV/AIDs acquisition. Less than a quarter (13.7%) believed that no risk behaviour is linked with STIs including HIV infection (Table 2). The sex workers’ perception of risk of HIV transmission was significantly associated with their age (ᵡ2= 7.69, p < 0.05) and level of education (ᵡ2 = 3.89, p < 0.05) but not with their marital status (Fisher’s exact p = 0.25) or duration in sex business (Fisher’s exact p = 0.64). The sex workers that were more than 24 years old were more likely to perceive that HIV transmission is associated with some risk behaviors (O.R = 6.82 [1.38; 45.53]). Similarly, those that posses at least secondary school level of education were also more likely to perceive that HIV transmission is associated with some risk behaviors (O.R = 2.95 [0.88; 10.41]) (Table 3). When the sex workers were asked about the measures to take in order to prevent themselves from STIs including HIV/AIDS while in business, majority (74.2%) reported the use of condoms. The sex workers also mentioned other remedies including antibiotics, vaginal douching and traditional herbs. Surprisingly, about a quarter (25.8%) do not believe that any method can be used to protect against HIV/AIDS and other STIs (Table 4). The respondents’ belief about prevention of HIV and other STIs was significantly associated with their level of education (ᵡ2 = 26.42, p < 0.05) and perception of risk for HIV transmission (ᵡ2 = 11.22, p < 0.05), but not with their age (ᵡ2 = 1.01, p = 0.31), marital status (Fisher’s exact p = 0.58) or duration in sex business (Fisher’s exact p = 0.59). Respondents that had at least secondary school level of education were more likely to perceive that the use of condom is effective for preventing HIV and other STIs. Similarly, those that believed that the transmission of STIs including HIV is associated with some risk behaviour were more likely to correctly perceive that the use of condoms is a veritable means of preventing HIV and other STIs (O.R = 5.52 [1.69; 18.48]) Table 3). Experiences with STIs and HIV/AIDS and treatment seeking We asked the sex workers about their experiences with common symptoms of STI syndromes in the last six months, and if they had undergone HIV screening within the period. The majority 84 (67.7%) had experienced one or more of the symptoms of STIs. The common symptoms reported include perineal itching (53.6%), abnormal vaginal discharge (45.2%) and dysuria/ painful urination (31.0%) as shown in Table 4. More than half of the sex workers that had symptoms of STIs, 51 (60.7%) continued to have unprotected sex with clients despite the infection. The sex workers’ indulgence in unprotected sexual intercourse despite symptoms of STIs was not associated with age (ᵡ2 = 0.48, p = 0.49), educational status (ᵡ2 = 0.36, p = 0.55), marital status (Fisher’s exact p = 0.27), duration in sex business (Fisher’s exact p = 0.47) or their perceptions of risk behaviour associated with transmission of STI and HIV (Fisher’s exact p = 0.52) (Table 3). The majority of the sex workers, 108 (87.2%) had been screened for HIV. Eighty nine (82.4%) were tested in the hospitals/clinics while the remaining 18.0% were tested in the brothels during a previous survey. Out of the 108 sex workers tested for the HIV antibodies, 76 (70.4%) were negative while 32 (29.6%) were positive. Alarmingly, all the HIV positive sex workers continued to engage in unprotected sexual intercourse with clients. We also asked the sex workers how they handled their experiences with STIs and HIV/AIDS. Three-quarter (75.0%) of the HIV positive clients attend antiretroviral treatment centres in hospitals; whereas half of those that had other STIs (53.6%), sought treatment in other hospitals/clinics (Table 6). Discussion Sex work is associated with the spread of sexually transmitted infections including HIV/AIDS. Studies in urban setting of sex work in developing countries have shown a strikingly high burden of STI among sex workers.7 This indicates a potential reservoir for STIs in the general population. Although the health authorities and non governmental organizations are investing a lot of efforts and resources on the sex workers to improve their knowledge and practices about safer sex, a significant proportion of them still indulge in unsafe sex. This development is a serious challenge to the control of STIs including HIV/AIDS. We observed that the majority of the sex workers correctly perceived that unprotected sexual intercourse, multiple sexual partners, and use of contaminated sharps and needles are common risk behaviours associated with STI and HIV acquisition. We also found that most of the sex workers reported the use of condoms as being most effective for STIs and HIV/AIDS prevention. However, while these findings are encouraging on one hand, it is disconcerting to find on the other hand that a significant proportion of the sex workers believe that there is no particular sex behaviour that predispose to the risk of contracting STIs and HIV infection. In addition, a sizeable number of the sex workers wrongly believe that the use of antibiotic cover after the day’s sex business, use of traditional herbs and selection of apparently healthy clients were formidable strategies that can protect one from contracting STIs including HIV infection. More disturbing is the fact that a quarter of the sex workers used “nothing” for prevention purposes. These findings do not augur well for the control of STIs and HIV/AIDS in Nigeria. The sex workers’ experience on STIs is a clear reflection of their perceptions and practices. More than two-thirds (67.7%) had reported experience with one or more symptoms of STI syndromes within the last six months. Common symptoms reported in order of occurrence were perineal itching, abnormal vaginal discharge and dysuria/ painful urination among others. These findings are similar to those reported by Oyefara from southern part of Nigeria,15 and Desai and colleagues from India,16 However, Zachariah and other scholars reported a lower prevalence of STIs (25%) among female commercial sex workers in rural Malawi, although the symptoms reported in both studies were similar.17 Perhaps the lesser prevalence reported from the Malawi study was due to the fact that it was conducted in a rural settlement while the other studies were based in urban areas where sex workers get more patronage. Sex workers are generally stigmatized, marginalized and criminalized by the societies in which they live and work in, and this makes it hard for them to access health and other social services. This is especially so in Kano where the Sharia legal system has officially banned prostitution from the state. This development is reflected in the health seeking behaviour of this vulnerable group. Almost half (46.4%) of the sex workers that were infected with STIs would not seek appropriate medical treatment from the hospitals. On the other hand, because of the belief that HIV/AIDS can be transmitted outside the sexual route, and perhaps as a result of interventions from health authorities and nongovernmental organizations, majority of the HIV positive sex workers sought care and support from the ART centres in the hospitals. While the rest of the sex workers sought help from other facilities such as patent medicine stores, traditional healers and from faith-based centres. This poor treatment seeking behaviour may be to fear of discrimination, ignorance, lack of finances, lack of access appropriate health care services. We observed in this study that the sex workers’ perceptions of risk behaviour associated with STI and HIV transmission; and of its prevention were significantly associated with their levels of education and age but not with the other variables considered. This is suggestive of the fact that intensified health education intervention will favourably have a stake in improving the respondents’ sex behaviour. In view of the observations that emanated from this study we recommend that the health authorities and NGOs in Kano should spearhead the development and implementation of a targeted peer education package for sex workers and their clients with a focus on reducing risk behaviours associated with STIs and HIV transmission, safer sex; and treatment seeking. The social structure in the brothels can be utilized to actualize this model. The sex workers should also be empowered through vocational training for occupational alternatives to sex work. It is clear that sex workers are ‘universally’ at high risk of becoming infected with HIV and other STIs, and that the situation varies widely between regions. However, it is also apparent that in many of the countries where STIs including HIV/AIDS is taking its heaviest toll, a large number of sex workers are being affected by HIV, and this is a major issue. Improving the situation will require greater efforts by governments, civil society organizations (CSOs) and NGOs; and individual members of the society to support sex workers. It is particularly important that sex workers gain access to HIV and STIs prevention and treatment programmes. Such programmes not only save sex workers’ lives but can also help to stem the wider impact that HIV is having on societies around the world. Competing Interest We (the authors) declare that we have no competing interests. Authors’ Contribution Lawan UM, Abubakar S, Aisha Ahmed. All the authors read and approved the final manuscript. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12007t5.jpg] [rh12007t2.jpg] [rh12007t3.jpg] [rh12007t4.jpg] [rh12007t1.jpg] [rh12007t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}