 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
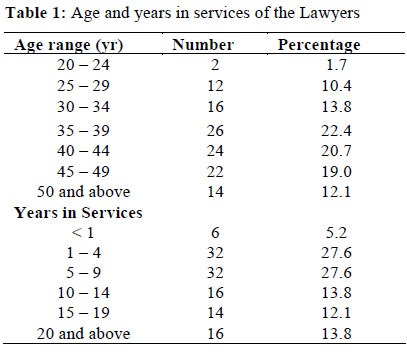
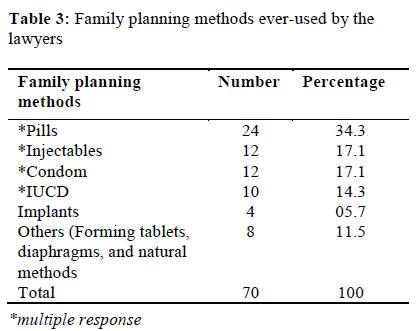
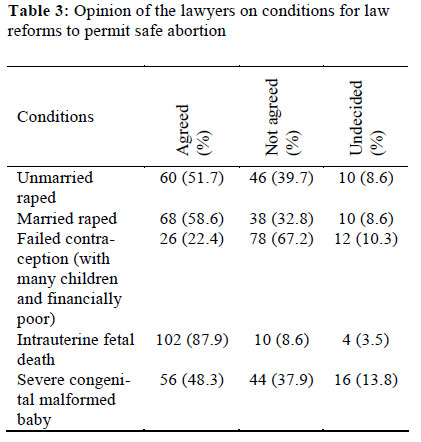
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 69-74 ORIGINAL RESEARCH ARTICLE Nigerian Lawyers and Reproductive Health Rights: A Survey of Knowledge, Practices and Opinions on Law Reforms among the Bar and Bench in North Eastern Nigeria Les Avocats et les droits de santé de la reproduction: Enquête sur la connaissance, l’usage et les opinions sur la reforme de la loi au sein des barreaux et des juges au nord-est du Nigéria Abdulkarim Garba Mairiga*1, Ado Dan’azumi Geidam1, Babagana Bako1 and Abdullahi Ibrahim2 1Department of Obstetrics and Gynaecology, University of Maiduguri Teaching Hospital, Maiduguri, Nigeria; Code Number: rh12008 Abstract The objective of this study was to determine the knowledge and attitudes of practicing Nigerian lawyers towards issues relating to reproductive health and reproductive rights, and their opinions about abortion law reform. It was a population-based study which consisted of interviews with practicing lawyers in north-east Nigeria. The results showed poor knowledge of issues related to reproductive health and reproductive rights among the lawyers. However, the majority (56.9%) disagreed that a woman can practice family planning without the consent of her husband. The prevalence of contraceptive use among the lawyers was low and attitude to abortion law not satisfactory. Only few lawyers (22.4%) supported safe abortion in cases of failed contraception. We conclude that reproductive health advocates must target legal professionals with a view to educating them on issues relating to sexual and reproductive health and rights. Lawyers in Nigeria should undergo capacity building in reproductive health laws and be encouraged to specialize in reproductive rights protection as obtainable in other developed countries (Afr J Reprod Health 2012; 16[1]:69-74). Résumé Cette étude a comme objectif de déterminer la connaissance et des attitudes des avocats nigérians en exercice par rapport aux problèmes relatifs à la santé de la reproduction et leurs opinions sur la reforme de la loi de l’avortement. Il s’agissait d’une étude basée sur la population qui comprenait des interviews auprès des avocats en exercice au nord-est du Nigéria. Les résultats ont montré une faible connaissance des problèmes relatifs aux droits de santé de la reproduction chez les avocats. Néanmoins, la majorité (56,9%) n’était pas d’accord qu’une femme puisse pratiquer la planification familiale sans le consentement de son mari. La prévalence de l’utilisation du contraceptif chez les avocates était faible et leur attitude envers la loi de l’avortement n’était pas satisfaisante. Il n’y avait que peu d’avocats (22,4%) qui aient soutenu l’avortement sans danger au cas de la contraception ratée. Nous concluons que les champions de santé de la reproduction doivent viser les avocats en vue de les éduquer par rapport aux problèmes relatifs aux droits de santé sexuelle et da la reproduction. Il faut que les avocats au Nigéria subissent un renforcement des capacités en ce qui concerne les lois de santé de la reproduction et il faut les encourager à se spécialiser dans la protection des droits de reproduction comme c’est le cas dans les pays développés (Afr J Reprod Health 2012; 16[1]:69-74). Keywords: Reproductive health, Nigerian lawyers, Northeastern Nigeria, Knowledge, Practice Introduction The International Conference on Population and Development (ICPD) held in Cairo in 1994 marked the recognition of a new paradigm in addressing human reproduction and health. For the first time, there was a clear focus on the needs of individuals, on the empowerment of women, and the appearance of a growing discourse on the relationship between human rights and health, linking new ideas of health to the struggle for social justice and respect for human dignity.1 Over the years, a human rights-based approach to reproductive health has evolved which emphasizes the rights to health, to have children by choice, and to have a safe and satisfying sex life. It is now recognized that women and (men) have the right to attain the fullest enjoyment of sexual health throughout their life cycle.Rights are defined as ‘legitimate claims’ which involve three intersecting dimensions: social, legal and personal.2 Social rights consist of claims that are legitimized variously by religion, ideology, traditions, culture and social norms. Legal rights are defined in international and national laws. The personal dimension concerns how individuals perceive their rights, based on their experience, knowledge and multiple influences from the social dimensions. Reproductive rights are entitlements to social conditions and services that make reproduction a truly mutual effort between men and women in an atmosphere devoid of coercion, fear or stigmatization. International human rights law provides well established conceptual frameworks for sexual and reproductive health (SRH) rights, 3 but how far are they relevant to the policy debate on SRH in Nigeria? The gap between legal human rights and the truth in Nigeria is enormous, particularly for poor women, men, girls and boys.4 The impediments to making SRH rights a reality in our region are multiple and mutually reinforcing, encompassing socio-cultural and gender norms, resource and capacity constraints, and unfavorable legal environments. These have much influence on not only the masses but including the policy makers and the law enforcement agents. Despite efforts by the Nigerian government, advocacy by civil society organizations, and huge financial allocations by international donor agencies, laws and policy regulations on reproductive health issues are ineffective and in dire need for reform. Despite the presence of national policies on population and reproductive health, family planning programs continue to suffer serious setbacks due to people’s socio-cultural inclinations. Abortion laws are extremely restrictive with possible reforms seeming a long way off. Attempt to reform the Nigeria's restrictive abortion law, in 2007, was opposed by women's groups and anti-abortion groups. Two bills submitted to the Nigerian national assembly—one designed to fully implement the terms of the International Convention for the Elimination of all Forms of Discrimination Against Women (CEDAW) and the other to establish an Institute of Reproductive Health in the country—were rejected because antiabortion protesters (including women) accused the bills' sponsors of attempting to legalize abortion. In these two situations, it was evident that policymakers were guided by moral and religious considerations rather than by evidence-based approaches. Lawyers and legal professionals are key stakeholders in the fight against reproductive health rights violations and abuses. In the quest for reproductive health rights of citizens, the knowledge, practices and opinions of lawyers have not previously been investigated in Nigeria, hence the need for this study. We undertook this pilot study to explore the knowledge, attitudes and perceptions of legal practitioners on matters relating to sexual and reproductive health and rights, and their opinions on abortion law reforms in Nigeria. We believe the results will be useful in finding ways to enlist lawyers in advocacy activities geared towards promoting sexual and reproductive health rights in Nigeria. Methods Study Area This study was conducted in 2009 in Adamawa, Bauchi, Borno and Yobe states, four of the six states in the north-east geo-political zone of Nigeria. According to Demographic Surveys of 2008, The Nigerian census of 2006 indicated that the region had a population of 18, 971,965 spread over 272,395 km2 of land area5. In this area, early marriage is the norm and polygamy is widespread. According to the National Demographic Health Survey of 2008, the fertility rate in the region was 7.2 children per woman, current use of any modern family planning method was only 4 percent. And 25% of childbirth occurs less than two years from the preceding birth6. A study in the area among physicians indicated that unsafe abortion was common in the area, with nearly all the physicians involved in managing unsafe abortion.7 Major ethnic groups in the area are Hausa, Fulani and Kanuri. Subsistence farming and fishing are the predominant occupations of citizens living in these states. Sampling This is a descriptive population-based quantitative study. In April 2009, Ipas brought together a team of lawyers and the police from the North-east States of Adamawa, Bauchi, Borno, and Yobe, with the aim of establishing a national network working on reproductive health and reproductive rights. The aim of the network was to advocate for positive reforms in policies and laws that relates to reproductive health rights, to sensitize the law enforcement agents on reproductive health and rights issues and to create a team of law enforcement agents that will ensure implementation of the positively-related existing policies and laws. All participants of that conference served as the subject of the study. Data Collection A self-administered questionnaire was designed for the study. The structured questionnaire, which had undergone pre-testing prior to the study, contained 23 questions to assess respondents' knowledge of reproductive health and reproductive rights, their opinion on abortion law reforms (specifically in cases of rape, life-threatening congenital malformations and failed contraception) and their opinions and practices of family planning. Socio-demographic information was also collected, including sex, age, religion, marital status and years of practice as a lawyer. Respondents were also asked to provide their opinions on circumstances in which he or she thought abortion should be legalized in Nigeria. Some of the proffered circumstances included: life-threatening congenital malformation of the fetus, fetal death in-utero, rape, socioeconomic reasons and contraceptive failure. Responses were classified under three broad categories -as agreed, not agreed and undecided. Consent to undertake the study was obtained from Borno State Ministry of Justice and the Nigerian Bar Association, Borno state chapter. The primary outcome measures were the lawyers’ knowledge and practices on reproductive health and rights, and their opinion on abortion law reforms. Data analysis The completed questionnaires were collated and entered into the computer. The data was analyzed with the Statistical Package for Social Sciences (SPSS) computer software and the results were presented in simple percentages. Results Bio-data of respondents Out of the 140 lawyers targeted, 116 filled in and returned the questionnaires; giving a retrieval rate of 82.9%. Sixty eight (58.6%) were male and 48(41.4%) were female lawyers. Eighty eight (75.9%) of the lawyers were married, 26 (22.4%) were single and two (1.7%) were widows. Seventy two (62.1%) were Muslims and 44 (37.9%) were Christians. Knowledge of reproductive health and reproductive rights Ninety-two (79.3%) of the respondents indicated that reproductive health addresses both male and female health issues and 24 (20.7%) believe that it addresses only female health issues. With regard to components of reproductive health, only 44 (37.9%) of the respondents identified at least four of the eight listed components and only 20 (22.2%) of the respondents identified at least three conventions/declarations that enshrined reproductive and sexual rights. As to whether a woman can practice family planning without the consent of her husband, 66 (56.9%) did not support the idea, 38 (32.8%) supported the idea, while 12 (10.3%) were undecided. Family planning practices among the lawyers Fifty two (44.8%) of the respondents had ever used one or more family planning methods. Out of the 64 (55%) that had never used any methods, 13 were not married while 51 were either married or windowed. Opinions on conditions for abortion law reforms Where culture goes contrary to human rights, 88 (75.9%) of the respondents indicated that they will support human rights, 14 (12.1%) will prefer their culture, while 14 (12.1%) were undecided. Discussion This study has found out that the knowledge of reproductive health and reproductive rights were poor among the lawyers interviewed; who are key stakeholders in the crusade toward achieving better reproductive health. Our socio-cultural influences on our lives are still strong among the lawyers; despite the level of their education. Even though the lawyers were selected randomly, there was fair gender representation in the sampling of the respondents. Respondents within the age bracket of reproductive life (15-49 years) (88%) dominated the sample (Table 1) which indicated that key stakeholders were reflected in the study. The respondents were mostly (62%) Muslims; which was a reflection of the dominant religion in the region. Ninety two (79.3%) of the respondents knew that reproductive health addresses the health issues of both male and female. Yet the knowledge of sexual and reproductive health and rights among the respondents was not encouraging as only 37% could identify four out of the eight components of reproductive health listed, and only 22.2% could identify three out of the six conventions and declarations that enshrined sexual and reproductive health and rights. This indicates that lawyers currently will not be good advocates on reproductive health rights, and that probably is responsible for the inadequate or rare implementation of laws protective of women’s reproductive health or even in some cases laws obstructing the women’s reproductive rights and services.8 Eighty eight (75.9%) of the respondents indicated that where culture goes contrary to human rights, they will abide by the human rights. Yet majority of them (56.9%) disagreed that a woman can practice family planning without the consent of her husband. This point stressed the dominant influence of our personal/social rights over the legal rights.9 These socio-cultural influences on our behavior and attitudes have dominant role across the African continent10 not only in our region. Many countries in Africa, the Middle East, and Latin America continue to significantly restrict reproductive rights. Laws limiting access to abortion, contraception, and sexual education, for example, negatively affects women. In such cases, women may suffer the sequelae of unsafe and illegal abortions or face the difficult choice between abstinence and keeping an unwanted pregnancy.11 Considering the educational level of the lawyers, the 44.8% rate of ever used contraception is unacceptably low. Contraceptive pill was the commonest method used by the lawyers, while condom, with its attendant dual functions was practiced by only 17.1% of the contraceptive users (Table 2). Studies in Nigeria have shown that the potential to have consistent condom use in educated youth populations is hindered by several barriers. The major barriers are that condom does not give desired sexual satisfaction, makes intercourse to be boring, reduces enjoyment of sexual foreplay, produces health problems such as itching and reduces sexual urge.12, 13, 14 Probably some of these notions contributed to the low acceptance among the lawyers. Twenty four (24.2%) of the respondents gave preference to their culture or were undecided whenever there is clash of interest between culture and human rights. Again this could be a clear manifestation of dominance of personal/social rights over legal rights; which the lawyers are expected to safeguard. As regards their opinion on conditions where they think abortion should be legalized in Nigeria, only cases of intrauterine fetal death had an overwhelming support followed by rape cases. The former received the overwhelming support probably due to perceived danger to the health of the mother. Unfortunately only few lawyers (22.4%) supported safe abortion in cases of failed contraception, even when the couple had enough children and were financially poor to take care of those they already had (Table 3). That means many lawyers may perpetuate the existing reproductive health violations when given the opportunity. This study has found out that the knowledge of reproductive health and reproductive rights are poor among our lawyers; who are key stakeholders in the crusade towards achieving better reproductive health. Our socio-cultural influences on our lives are still strong among the lawyers; despite the level of their education. With current findings, lawyers might not be good ambassadors or advocates for reproductive health and reproductive rights. Therefore, international donor agencies, civil society organizations and other reproductive health advocates must target the lawyers with the view to inform, educate and communicate to the lawyers on reproductive health and reproductive rights. In many countries, including Nigeria, the laws addressing reproductive and sexual health are vague, insufficient, or in violation of international human rights standards. Federal government should affirm their commitment to these rights by domesticating and implementing the provisions of the Convention on the Elimination of All Forms of Discrimination against Women. Systematic review at the national level would help to identify areas of law and policy that need strengthening or revision. There is also the need for further research into how lawyers can play their roles better in reproductive health rights. Lawyers in Nigeria should be encouraged to specialize in the reproductive rights as is obtainable in other developed countries. Acknowledgement This is to express our gratitude to Ipas, especially the Country Director, Dr Ejike Oji, for not only permitting us to conduct the study during the Lawyers conference but also for the useful suggestions on the success of the study. Our unflinching gratitude and appreciations also go to the coordinator of the Bar, the Bench and the Police reproductive health project (Northeast chapter) Barrister Ibrahim Watila and other members of the Nigerian Bar Association; who contributed immensely in distributing and retrieving the questionnaires. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12008t3.jpg] [rh12008t2.jpg] [rh12008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}