 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
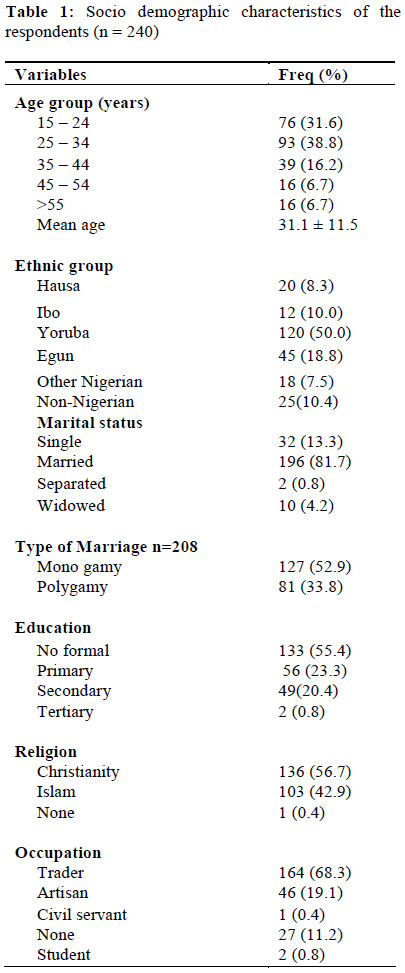
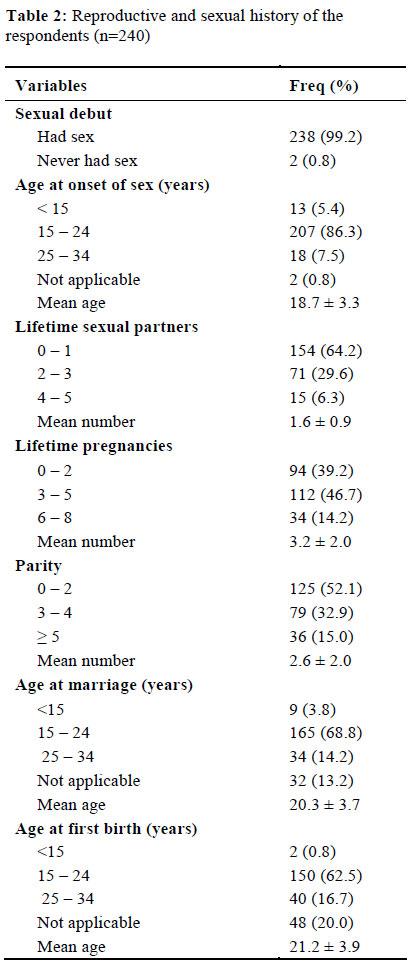
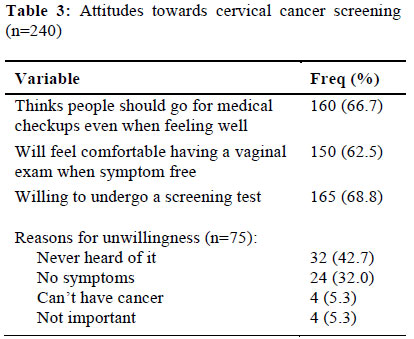
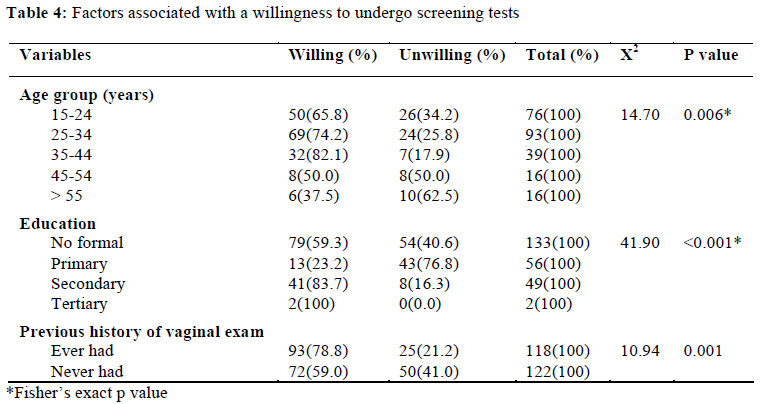
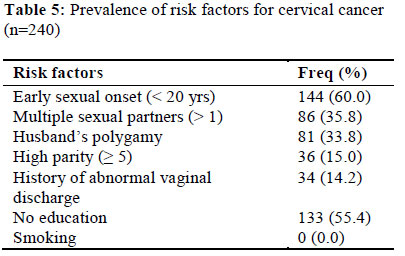
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 75-82 ORIGINAL RESEARCH ARTICLE Cervical Cancer Awareness and Preventive Practices: A Challenge for Female Urban Slum Dwellers in Lagos, Nigeria Prise de conscience du cancer du col de l’utérus et les pratiques de la prévention : Défi pour les habitantes des taudis urbains à Lagos, NigériaBalogun MR1, Odukoya OO1, Oyediran MA1 and Ujomu PI2 1Department of Community Health and Primary Care, College of Medicine of the University of Lagos; Code Number: rh12009 Abstract Cervical cancer is the commonest gynaecological cancer in Nigeria and women of low socio-economic status are at high risk of this condition. A study was conducted on the awareness of cervical cancer, attitude towards the disease and screening practice of women residing in two urban slums of Lagos, Nigeria. It also determined the prevalence of major risk factors for cervical cancer among the women. Multistage sampling was used to select 240 women who were interviewed with a structured questionnaire and data collected was analyzed with Epi-info version 3.5.1 statistical software. Only 10 (4.2%) women in this study were aware of cervical cancer and none of them believed they were at risk of developing the disease. Most (73.3%) were willing to undergo a cervical cancer screening test. Age, education and previous history of vaginal examination were positively associated with willingness to undergo screening (p < 0.05). The respondents had a high prevalence of major risk factors for cervical cancer such as early age at sexual debut, multiple sexual partners and male partner with other female partners. Efforts need to be intensified to increase awareness of this condition and to promote low-cost cervical cancer screening among this underserved population (Afr J Reprod Health 2012; 16[1]:75-82). Résumé Le cancer du col de l’utérus est le cancer gynécologue le plus commun au Nigéria et les femmes du milieu socio-économique inférieur sont à haut risque de cette condition. Une étude a été menée sur la prise de conscience du cancer du col de l’utérus, l’attitude envers la maladie et la pratique du dépistage chez les femmes qui habitent deux taudis urbains à Lagos, Nigeria. Elle a déterminé également la prévalence des facteurs de risque majeurs pour le cancer du col de l’utérus chez les femmes. On s’est servi d’un échantillon à étapes multiples pour sélectionner les 240 femmes qui ont été interviewées à l’aide d’un questionnaire structuré et des données collectées et analysées à travers la version Epi-info 3.5.1 logistiel de statistique. Seulement 10 femmes (4,2%) dans cette étude étaient au courant du cancer du col de l’utérus et personne d’entre elles ne croyait qu’elle courait de risque d’attraper la maladie. La grande majorité (73,3%) voulait bien subir un dépistage pour détecter le cancer du col de l’utérus. L’âge, l’éducation et une histoire précédente d’examen vaginal ont été positivement liés à la volonté de subir le dépistage (p<0,05). Les interviewées avaient une prévalence élevée de facteurs de risque majeur à l’égard du cancer du col de l’utérus tels l’âge lors du premier rapport sexuel, de multiples partenaires sexuels et un partenaire de sexe masculin avec d’autres partenaires de sexe féminin. Il faut intensifier des efforts pour augmenter la conscience à l’égard de cette condition et pour promouvoir des examens du dépistage du cancer du col de l’utérus qui ne coûte pas cher au sein de cette population dont on s’occupe mal (Afr J Reprod Health 2012; 16[1]:75-82). Keywords: Attitude, Cancer screening, Cervical cancer, Preventive practices, Nigeria Introduction Cervical cancer is the second most common cancer among women worldwide but the commonest in developing countries.1 It accounts for approximately 12% of all cancers in women worldwide1 and disproportionately affects women in developing countries where age-standardized incidence rates (ASRs) range between about 25 and 43 cases per 100,000 women, in contrast to that of North America which is 7.7 cases per 100,000 women. The ASR for Nigeria, where it is the commonest gynaecological cancer, is 28.5 per 100,000 women.2, 3 The disparity in prevalence between the developing and developed world can be attributed to lack of awareness of cervical cancer and the lack of effective cytological screening programs in developing countries.4 Other reasons include the constant focus on competing health priorities such as HIV/AIDS, tuberculosis and malaria.5 Cervical cancer is one of the most preventable human cancers because of its slow progression, cytologically identifiable precursors, and effective treatments if detected early. Papanicolaou (Pap) test also known as cervical cytology screening has helped to reduce cervical cancer rates dramatically through the detection of premalignant lesions.6, 7 Alternative screening approaches such as visual inspection with acetic acid (VIA), visual inspection with Lugol’s iodine (VILI), cervicography and speculoscopy have also been explored in the prevention of cervical cancer in resource-poor settings. They are simple, cost effective and promote a “screen and treat” mechanism that entails diagnosis and treatment at a single visit.1,3,4 However, most screening activities in developing countries do not reach the vulnerable women and consequently, a high proportion of cervical cancer cases are diagnosed at an advanced stage.8 The utilization of cervical screening services has been low due to absence of knowledge about the disease, lack of familiarity with the concept of preventive health care, poor quality of services, limited human resources and geographic and economic inaccessibility of services.9 Human papillomavirus (HPV), a sexually transmitted disease is the primary causal agent of cervical cancer. Prevalence of high-risk HPV types seems to be high among Nigerian women.1012 Previous studies have also shown a prevalence of major risk factors for cervical cancer among Nigerian women. These factors include low socioeconomic level, early age at first sexual intercourse, multiple sexual partners and previous history of sexually transmitted diseases.3, 13, 14 Although, a lot of research on cervical cancer has been carried out among various groups of Nigerian women cutting across different socioeconomic strata, there has been little focus on women living in urban slums. These slum dwellers are disadvantaged in terms of their socio-economic status. They often have limited income, restricted access to health care services, poor nutrition, and a low level of awareness about health issues and preventive behaviour.15 Even in more developed countries, coverage levels for cervical cancer screening were found to be low among women of low socioeconomic status.16-18 Similarly, place of residence is important in predicting health outcomes. For example, according to a study by Barry and Breen, lower class and extreme poverty areas in the United States were more likely to have later stage diagnosis of cervical cancer.19 This study assessed the awareness of cervical cancer, attitude towards the disease and screening practice of the respondents. The study also determined the prevalence of major risk factors for cervical cancer among the women. It forms the baseline findings of a larger intervention study that focused on the effect of a community-based screening program on the knowledge, attitudes and practices of women in urban slums regarding cervical cancer. Methods Study location This study was carried out in two urban slums in Lagos state, Nigeria. One of the slums, ‘Makoko waterside’ is located within Makoko community in Lagos Mainland local government area. The other slum is Abete community located within Ijora Badia ward in Apapa local government area. The houses and huts in both slums are numerous and scattered across a very large expanse of land (and water, in the case of Makoko) with no form of planning. They are typically made of wooden planks and dilapidated zinc. There is no government hospital or clinic within the community, no pipe-borne water or drainage system. Study population and design Study participants were women who were fifteen years of age and above. Selected households were visited and the oldest eligible female was recruited for this descriptive cross-sectional survey, which was carried out in January 2009. Sampling methodology A total of 240 women were selected using a multistage sampling technique. First, each community was divided into four clusters based on the arrangement of houses and thirty houses were selected within each cluster. The index house in each cluster was selected by spinning a bottle in the middle of the cluster and the bottle observed to see where its tip pointed; the house whose front door was closest to the tip was the index house. The next house was the one whose front door was closest to the index one and so on. Second, a household was randomly selected from each house by balloting and lastly, from each selected household, the oldest female from 15 years and above was selected for the questionnaire survey. In the event that there wasn’t any such female in the selected household, it was excluded and the next household was selected. Data collection and analysis The Research and Ethics Committee of the Lagos University Teaching Hospital (LUTH) approved the study proposal. The data collection tool was a pre-tested structured questionnaire which was administered by two trained female interviewers. The questionnaire contained questions on demographic details, reproductive and sexual history of respondents, awareness of and attitude towards cervical cancer and practice of cervical cancer screening. Verbal informed consent was sought from each respondent before administration of the questionnaire. Data collected were collated and analyzed using EPI-info Version 3.5.1 statistical software. Chi-squared test was used to determine statistical difference in bivariate analysis with level of significance pre-determined at p-value < 0.05. Results Two hundred and forty women were interviewed in the two slum communities. The ages of the respondents ranged from 15 to 65 years with a mean age of 31.1 ± 11.6 years. Most of the respondents (38.8%) were aged between 25 and 34 years. Half of the respondents were of Yoruba ethnicity. A little more than half of the respondents were Christian (56.7%) while 42.9% were Moslem. Most of the respondents (81.7%) were married with 52.9% being in a monogamous marriage. Most of the respondents (55.4%) had no formal education while a majority of them (68.3%) were traders (Table 1). The Majority (98.6%) of the respondents had commenced sexual activity as at the time of the study with 86.3% occurring between ages 15 and 24 years. Over a third of the women (35.9%) had had at least two lifetime sexual partners whilst 60.9% of the respondents had at least three lifetime pregnancies. Respondents’ mean age at marriage was 20.3 ± 3.7years and mean age at first birth was 21.2 ± 3.9 years (Table 2). Only ten respondents (4.2%) were aware of cervical cancer prior to the study and none of them believed they were at risk of developing the disease. Over two-thirds (66.7%) of the respondents were of the opinion that people should go for medical check-ups even when they are feeling well. Similarly, most of the respondents (62.5%) had a positive attitude towards having vaginal examinations performed on them even if they had no symptoms. Over a quarter of respondents (31.2%) were not willing to undergo a screening test for cervical cancer, the commonest reasons being lack of awareness and absence of symptoms (Table 3). There were statistically significant associations between age, education and previous history of vaginal examination and a willingness to undergo a screening test for cervical cancer. Higher proportions of respondents in the younger age groups (p=0.006) and higher proportions of respondents with at least a primary education were willing to undergo the screening test (p<0.001). Furthermore, respondents who had ever had a vaginal examination were more willing to undergo a screening test for cervical cancer (p = 0.001) (Table 4). Over half of the respondents (60.0%) had a sexual debut at an early age i.e <20 years. Over a third (35.8%) had had multiple sexual partners; 33.8% were from polygamous marriages. Up to 15.0% were of high parity (≥ 5 children) while 14.2% of them had a history of abnormal vaginal discharge. More than half of them (55.4%) had no formal education (Table 5). None of the women interviewed in either community was aware of a screening test for cervical cancer nor had any ever been screened for cervical cancer. Discussion Lack of awareness of cervical cancer has been identified as one of the factors contributing to the high prevalence of this condition in the developing world compared to the developed world.1, 4 In this study, awareness of cervical cancer was dismally low; the proportion (4.2%) was much lower than those found in other community-based African studies among women of low socioeconomic status.20 -22 This could be explained by the very low educational level of the women in this study compared to other Nigerian women widely studied in the 2008 Nigerian Demographic and Health Survey23 and also because they are an underserved population with limited access to health information and services. The awareness of a cervical cancer screening test was much lower as none of the women in this study was aware of such a test. Similarly low levels of awareness have been reported in other studies 21, 24 None of the women interviewed in this study had ever had a cervical cancer screening test. This is hardly surprising as there was no awareness of the test in the value population and little or no access to cervical cancer prevention services, a problem already identified in developing countries.5 Poor practices of cervical cancer screening were seen in other African studies, with prevalence rates less than 15% even among those awareness of the condition. 20,21, 25, 26 Only 0.3% of female professional heath workers surveyed in a similar study conducted in Ilorin had ever had a screening test. 25 The belief in personal susceptibility towards cervical cancer has been shown to be a determinant of future intentions to have a Pap smear.27 In this study, the belief in personal susceptibility to cervical cancer was very low as none of the women felt they were at risk of cervical cancer. This finding was also observed among health workers in Benin City in Nigeria where up to 89% of female health workers surveyed felt they were not at risk of developing cervical cancer. 28 In contrast, 58.9% of women interviewed in Singapore and 75.7% in Turkey felt they were susceptible. 27, 29 Lack of familiarity with the concept of preventive health care has been identified as a barrier to cervical cancer screening uptake.5 Most of the women in this study were of the opinion that people should go for medical check-ups even when they are feeling well. They also had a positive attitude towards having vaginal examinations performed on them even if they had no symptoms and most of them were willing to have a cervical cancer screening test. These findings may imply that improving access to preventive health care services may increase the uptake of cervical cancer screening among the women. Over a quarter of respondents (31.2%) were however not willing to undergo a screening test for cervical cancer. The commonest reasons for this were lack of awareness of the test and absence of symptoms. This is erroneous as the screening test is aimed at detecting precursor conditions before the onset of symptoms. Similarly, underserved women in studies in South Africa and in the US were more likely to ignore cervical cancer screening when no symptoms were present.30, 31 Even among the more educated women in Nigeria, lack of symptoms and low perception of risk has been shown to be major reasons for not having cervical cancer screening tests. 26,28 In this study, younger age, education and previous history of vaginal examination were positively associated with a willingness to undergo a screening test for cervical cancer. A few of the older women interviewed were not interested in the screening test because they felt they were too old; this is a misconception as older-aged women are at an increased risk of developing cervical cancer.2 Similar findings were reported in a study among Turkish women where age, education and attitude towards a vaginal examination were associated with an increased uptake of screening.32 Despite, the low awareness and knowledge of cervical cancer, the belief of not being susceptible to the disease and the poor attitude to screening among the respondents, there was a high prevalence of the major risk factors for cervical cancer amongst the respondents. This included initiation of coitus before 20 years, multiple sexual partners, male partner with other female partners, high parity, history of treatment for abnormal vaginal discharge (an indicator of vaginal or cervical infection)33 and no education (an indicator of low socioeconomic status). 33 Early age of sexual debut has been cited as a risk factor for cervical cancer as damage might be caused to the cervix at a time when it is still developing.34 Majority (86.3%) of the respondents in this study had their sexual debut between ages 15 and 24 years with 5.4% commencing sexual activity before the age of 15 years. The number of sexual partners also plays a role in cervical cancer risk as this increases the risk of infection with HPV. Over a third of the women surveyed (35.8%) had had at least two lifetime sexual partners. High parity may also serve as a risk factor for cervical cancer. Fifteen percent of respondents had at least five children at the time of the survey. In a similar study in Kenya, having multiple sexual partners, early age at first sexual intercourse, multiparity and low educational attainment were found to be associated with cervical cancer.35 Low education was also demonstrated to significantly increase the risk of invasive cervical cancer in a study conducted among Thai women.33 Other studies have also proposed that early age at sexual initiation, high parity and cigarette smoking may be relevant factors that modulate the oncogenic effect of HPV infection. 36, 37 The smoking rates of Nigerian women is however comparatively low23 and this may account for the fact that there was no current or previous smoker among the respondents Conclusion This study demonstrated a very low awareness of cervical cancer and absence of cervical cancer screening practice among the female urban slum dwellers. Efforts need to be intensified to increase awareness of this condition and promote low-cost cervical cancer screening among this underserved population at high-risk for cervical cancer. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12009t3.jpg] [rh12009t5.jpg] [rh12009t2.jpg] [rh12009t4.jpg] [rh12009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}