 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
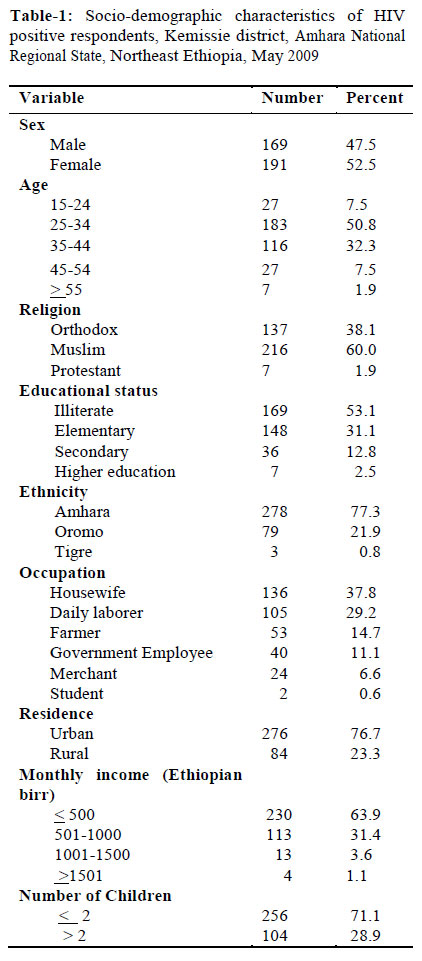
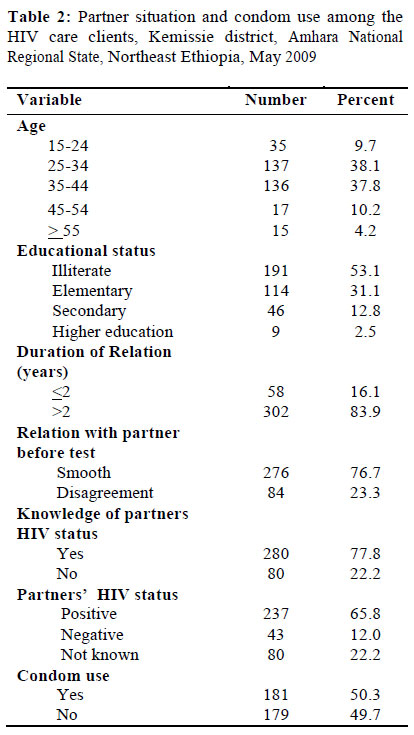
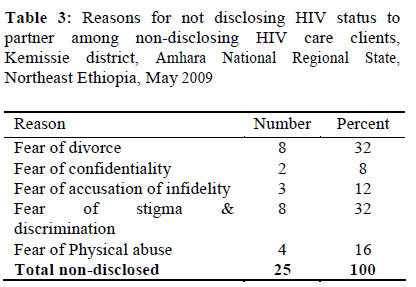
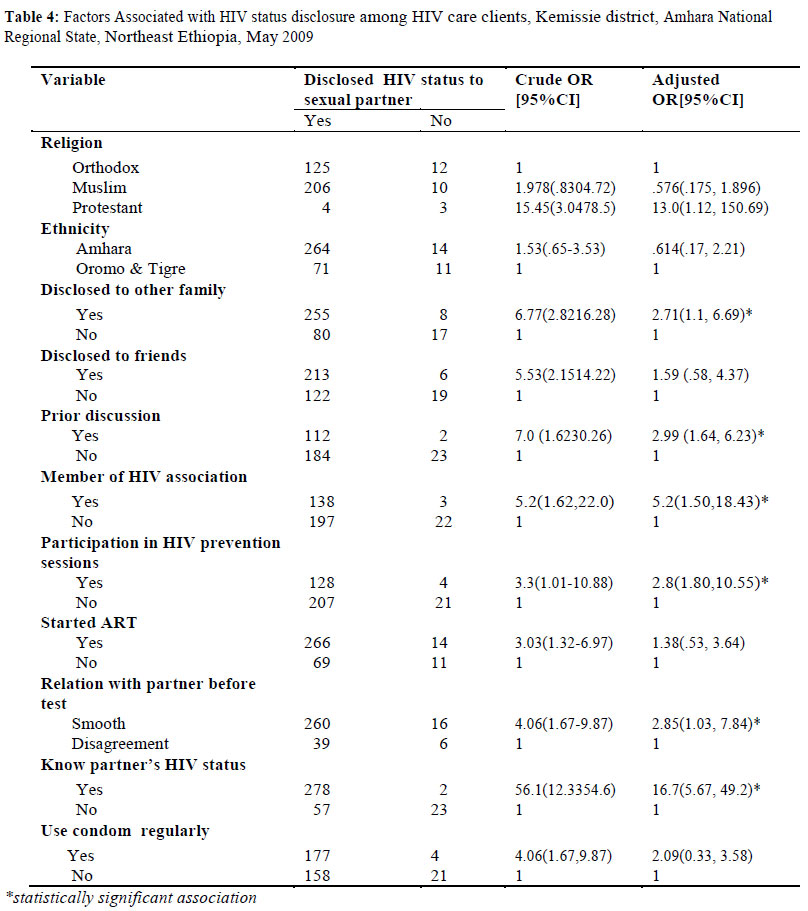
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 97-104 ORIGINAL RESEARCH ARTICLE Disclosure of HIV Positive Result to a Sexual Partner among Adult Clinical Service Users in Kemissie District, Northeast Ethiopia Révélation du résultat séropositif à un partenaire sexuel parmi les usagers adultes du service clinique dans le district de Kessimie au nord-est de l’Ethiopie Mohammed Seid1, Belaynew Wasie2* and Mengesha Admassu3 1Kemissie District Health Office, Kemissie, Ethiopia; Code Number: rh12011 Abstract HIV Status disclosure is vital for HIV prevention efforts and the couple’s health in the context of accelerated highly active antiretroviral therapy. This study aimed to identify factors associated with disclosure of HIV Status to a sexual partner and its outcomes. A facility based cross-sectional study was conducted at Kemissie Health center on 360 HIV positive individuals selected by systematic random sampling. Data were collected using a structured, interviewer administered questionnaire. The level of disclosure to a sexual partner was 93.1%. Among those who disclosed, 74.5 % were accepted, 10.8% minor challenges or suspicion of result and the last 7.8 % faced physical abuse and blame. The main reasons for not disclosing were fear of divorce [32%], fear of stigma and discrimination [32%] and fear of physical abuse [16%]. Prior discussion, disclosure to family, smooth relationship and knowing partner status were significantly associated with disclosure. HIV prevention programs and counseling efforts should focus on mutual disclosure of HIV test results, by encouraging discussion, reduction of stigma, for better disclosure and continuing care (Afr J Reprod Health 2012; 16[1]:97-104). Résumé La révélation d’état de santé par rapport au VIH est cruciale pour les efforts envers la prévention du VIH ainsi qu’à la santé du couple dans le contexte d’une thérapie antirétrovirale active et hautement accélérée. Cette étude avait comme objectif d’identifier les facteurs liés à la révélation d’état de santé par rapport au sida à un partenaire sexuel et ses conséquences. Une étude transversale qui est basée sur un établissement de santé a été menée au centre médicosocial de Kimissie auprès de 360 individus séropositifs qui ont été sélectionnés à travers un échantillon randomisé systématique. Nous avons collecté les données à l’aide d’un questionnaire structuré administré par l’enquêteur. Le niveau de révélation à un partenaire sexuel était de 93,1%. Parmi ceux qui ont révélé, 74,5% ont été acceptés, 10,8% ont fait preuve des défis mineurs ou des soupçons des résultats, alors que les derniers 7,8% ont vécu l’abus physique et la reproche. Les raisons principales qui font que les gens ne veulent pas révéler étaient la peur du divorce (32%) la peur de la stigmatisation et de la discrimination (32%) et la peur de l’abus physique (16%). Une discussion préalable, la révélation à la famille, une bonne relation et le fait de connaître l’état de santé du partenaire étaient liés de manière significative à la révélation. Les programmes destinés à la prévention du VIH et les efforts des conseils doivent viser la révélation mutuelle des résultats des examens de dépistage du VIH à travers l’encouragement des discussions, la réduction de la stigmatisation pour permettre une meilleure révélation ainsi que le soin continu (Afr J Reprod Health 2012; 16[1]:97104). Keywords: Disclosure, HIV status, sexual partner, associated factors, Ethiopia, sub-Saharan Africa Introduction An estimated 30.8 million people worldwide were living with HIV at the end of 2007(1) . The prevalence of HIV in Ethiopia in 2007 was estimated to be 2.1 %. An estimated 977,394 people live with the virus resulting in 71,902 HIV related deaths in 2007 (2).The prevalence of HIV among couples is 2.1%. The majority of couples (1.8 percent out of a total of 2.1 percent) were discordant. There is an unmet need for VCT services oriented towards couples, because most of these couples do not mutually know their HIV status(3) . Disclosure of HIV status to sexual partners is an important prevention goal given emphasis by many organizations in their protocols for HIV testing and counseling(4) . Disclosure offers a number of important benefits to the infected individual and to the general public. Disclosure of HIV test results to sexual partners leads to less anxiety and increased social support among many women(5) . Disclosure is also crucial to the individual’s health in today’s context of accelerated highly active anti retroviral treatment use, to gain social and emotional support, to ensure proper adherence to treatment and better therapeutic efficacy (6-8) . Level of Disclosure among studies ranges from about 46 % in HIV positive to 94%(9-11) . Disclosure for the HIV infected individual could result in negative outcomes, including anger, yelling, rejection , physical violence(9) , loss of economic support, blame, abandonment physical and emotional abuse, discrimination and disruption of family relationships (10). These risks may lead women to choose not to share their HIV test results with their friends, family and sexual partners. This in turn leads to lost opportunities for the prevention of new infections and for the ability of these women to access appropriate treatment, care and support services where they are available(12, 13) . As evidenced in many settings, in the majority of the cases support; acceptance and understanding are the outcomes of partners up on disclosure of HIV test results (9, 10, 12-15) . Level and outcomes of disclosure depend on multiple factors as ethnicity, the extent to which people told their family, friends and partners with HIV, support from the other partner, presence of other partner (16, 17) . Other studies also found out that male gender, age over 50 years at diagnosis, nationality, sexual transmission of the virus and hospitalization were associated with disclosure(18) . In a research done in Abidjan, 96.7% of the HIV negative woman and 46.2% of HIV positive women disclosed their HIV positive status to their sexual partners during a two year follow up. Those having co-spouse or living with family reduced the probability of disclosure; partners of HIV positive women informed about their wife’s HIV status were more likely to undertake HIV testing(19, 20) . In other studies in Africa and elsewhere, fear of accusations of infidelity, abandonment, discrimination, test result, violence, being married, prior discussion about testing, having a partner with tertiary education, better housing, less financial dependence on partners, and knowing someone with HIV were important predictors of disclosure of HIV status among women(21-23) . Disclosure related factors can be different among men and women. In men only, older age, literacy and having good communication with the treating doctor were significantly associated with disclosure. Among women, disclosure was associated with having children and high selfreported importance of religion(24) . Among ART clients in Jimma University Hospital, Ethiopia, living in the same house, prior discussion, knowledge of the HIV status of one’s partner, clinical stage of the disease and level of negative self image determined disclosure. In the same study, fear of separation or divorce, not to worry partner, fear of accusation of infidelity, fear of physical abuse, fearing that partner will be angry and fear of partner getting HIV from me were the main reasons for not disclosing HIV Status (11) . Therefore, studying the factors affecting disclosure of HIV serostatus to a sexual partner in an area where no assessment was done previously is very important for the better care of PLHIV. It will enable identify those barriers and design an appropriate intervention addressing those barriers, facilitate disclosure and improves continuity of chronic HIV care. This study therefore aimed to assess the rate of disclosure of HIV positive result to a sexual partner, outcomes of disclosure and associated factors among HIV positive adult clinical service users in Kemissie district, Northeast Ethiopia. Methods A facility based cross-sectional study was conducted from March to August 2009 to assess HIV Status disclosure to a sexual partner, outcomes and associated factors among HIV positive individuals. The Study was conducted in Kemissie Health Center, Kemissie district found in Amhara National Regional State 325 kms Northeast of Addis Ababa. Kemissie district has an estimated population of 22,980. The prevalence of HIV, according to the 2005 sentinel Surveillance was 5.6 %. The district has one big health center in town and three health posts around the peripheries. There are two NGO’s (World vision and Family Guidance Association), six private clinics, two drug stores, and four drug vendors(25) . The health center has one ART Clinic and an ART pharmacy providing chronic care. At the study time, there were 1150 HIV positive individuals getting care in the ART Clinic; 690 of them were already taking the treatment (25) . The study population was all HIV positive individuals 15 years or above and getting clinical service at ART clinic. HIV positive clients on pre ART or ART at Kemissie Health Center and age 15 years or above and have partners were included in the study. On the other hand, extremely sick, patients with mental illness and unable to communicate coherently were excluded. Taking the rate of disclosure 69% in Metu and Gore towns, the required sample size at 95% Confidence interval, a marginal error of 5% and 10% non response rate, was 360. To select the study participants, systematic random sampling with sampling interval of 3 was employed. The outcome variables of the study were disclosure of HIV status and outcome of disclosure. Explanatory variables included socio demographic (age, Sex, ethnicity, Religion, occupation, educational status, place of residence, monthly income, number of children), psychosocial factors (prior discussion about HIV, being a member of HIV associations, participating in volunteer groups, people lived with), medical factors (clinical stage, treatment status, duration of the HIV test result), and partner related factors (age, level of education, Number of partners, type of partner, duration of relation with partner, knowledge of partner’s HIV status, partner’s HIV status). Face to face interview using a pre-tested, structured questionnaire was used to collect the data. Four data collectors and two supervisors trained for 2 days on objectives of the study and techniques of the interview collected the data from March 28 to May13, 2009. At the end of each day, data were checked for completeness and accuracy by supervisors and investigators. Data quality was maintained through careful design of study tool, carefully selected and well trained data collectors and supervisors. Questionnaire was also translated and back translated from English to Amharic and pre-testing was done on 30 individuals not included in the study. Each variable was coded and data were entered in to SPSS version 13 statistical software for analysis. Frequencies, proportions were used to determine level and outcomes of disclosure. Odds ratios and 95% confidence intervals were used to determine the significance and degree of association between dependent and independent variables. Multiple logistic regression model was used to identify the factors related to disclosure and control confounding. Ethical considerations Ethical clearance was obtained from Ethical Review Board of the School of Public Health, University of Gondar. A written permission was received from Zonal Health Department and Kemissie district health office. Before conducting each interview, the objective of the study was introduced and verbal consent from each respondent was secured. Finally each respondent was given information on the benefit of the study and that she/he could participate voluntarily and had the right to withdraw at any time without any negative effect on service provided. Counseling was arranged with the health center for study participants who had problems. Results Socio-demographic Characteristics of Study Participants A total of 360 HIV positive individuals who have partners were interviewed and the response rate was 100%. When we see the socio demographic characteristics of the study population, 191(52.5%) were females and the rest 169(47.5%) were males. The mean (+SD) age of the study population was 33.4 (+7.76) years and 210 (85.3%) of them were between 15-34 years. One hundred sixty nine (46.9%) did not attend any formal education and 278 (77.2%) were Amhara ethnics. Two hundred seventy six (76.7%) lived in urban areas (Table 1). HIV status disclosure Three hundred thirty five (93.1%) had disclosed their results to their main current sexual partner. Concerning disclosure to families and friends, 263 (73.1%) had disclosed their results to at least one of their families and 219 (60.8%) had told their result to one or more of their friends. Table 2 summarizes the variables related to partner situation. Only 119 (31.7 %) had prior discussion about HIV and testing before whereas 207 (57.5%) had no any prior discussion. When we consider their duration of HIV testing 116 (46.1 %) had been tested within one year and 194 (53.9%) before one year of this study. The mean (+ SD) duration of HIV testing of the study population was 19.2 (+ 15.8) months from HIV testing until the time of the study. Three hundred and two (83.9%) participants had more than two years relationship with their partner with a mean (+ SD) duration of relation of 8.0 (+6.5) years. Regarding their knowledge of partner status, 280 (77.8%) of the participants knew their partner’s HIV status. Among these, 237(65.8%) said that their partners were HIV positive, and in 43 (11.9%) of them, results were negative (Table 2). For those who did not disclose their results to their main partner the main reasons were fear of divorce 8(32%), fear of stigma and discrimination 8 (32%), fear of confidentiality 2(8%) fear of accusation of infidelity 3(12%) and fear of physical abuse 4 (16%)(Table 3). Outcomes of disclosure Among those who disclosed their results to their partner 268 (74.5%) had received positive outcomes like acceptance and receiving kindness and 28 (7.8%) had faced negative out comes like blame, physical abuse. The rest 39 (10.8%) of the clients who disclosed their result to their partners had faced either suspicion, disbelief of the result or minor challenges of why tested alone and then accepted later. Factors associated with disclosure Those who disclosed to their families (like parents, brothers, sisters, etc) were 2.7 times more likely to (OR=2.7; 95% CI, 1.2 -6.7).Those who had prior discussion were 2.99 times more likely to disclose to their main sexual partners when compared to those who did not have prior discussion (OR =2.99; 95%CI, 1.6 -6.2). Those who knew their partner’s status were 16.7 times more likely to disclose compared to those who did not know their partner’s status (OR=16.7, 95%CI, 5.7-49.2). Participants with smooth relation with their partner before the test were 2.85 times more likely to disclose their result as compared to those who were in disagreement with their partner before the HIV testing (OR=2.85 95%CI, 1.034-7.84). Clients who disclosed were more likely to have used condom regularly when compared to those who did not disclose (OR= 5.9, 95% CI, 1.98-17.5) (Table 4). Discussion From the study subjects 53.1% were females. This may be because the number of females who were getting service was higher than males in the health center. Similar to other studies, most of the study subjects were in the younger age group which is due to the fact that HIV affects younger ages. The level of disclosure in this study was high (93.1%). This is in agreement with the study done in Jima university hospital which was 90.8%(11) . But it is higher than that reported in Mali and Burkina Faso (79.9%), Metu (69%), Malawi (67%)(22-24) .The main reason for these differences might be due to the difference in population characters as this study was conducted in clinical setting whereas some of the other studies were conducted in community setting and some on women only. This study showed that only 6.9% of individuals did not disclose to their partners. In contrary to the DHS study(3) , 65.8% of individuals in this study reported that they have HIV positive partners and 22.2 % of the study population did not know their partner’s status(3) . The silence of the partners could either be due to the reason that he/she is already infected or the result of the emotional rejection of the partner. This result is in agreement to the one which was found in Jima University (11) . The discrepancy between this study and in the DHS might be due to the difference in the study population because DHS was community based where many individuals may not know their result. In this study it was clinical set up where individuals had accepted their result and who are on ART and pre-ART care. In this analysis, it was observed that disclosure to family, prior discussion, knowing partner status and relation with partner before HIV testing were independently associated with disclosure of HIV status to the main sexual partner. This is in agreement with studies elsewhere (9, 11, 16, 18, 24) . Communicating one’s partner prior to HIV testing is a key point in that it might help individuals to anticipate a partner’s reaction and would give them an opportunity to raise the issue and disclose their result; in this case disclosure may be easily discussed between partners since it was already started before testing. Discussing things about HIV testing and HIV test result with family facilitated disclosure of HIV positive result to sexual partner (OR=2.71 95% CI 1.1-6.69). This might have helped individuals to be strong and disclose their result to their partner. This may be because sharing ideas with family members gave strength for individuals spiritually as well as mentally, so that they can anticipate and accept the outcomes following disclosure and disclose their HIV status. Knowing partner status was strongly associated with disclosure of HIV status which is in agreement with many studies (11, 24), OR= 16.7 95% CI 5.7-49.2). But the status of the partner was not associated with disclosure of HIV positive result. This indicates that the matter is not the HIV status but the knowledge of a partner about the status of his/her counterpart. Having smooth relations with partner was significantly associated with disclosure in this study unlike the others(9); this might be due to the smooth relations leading to discussions about HIV and HIV testing which may later ease disclosure. Even though the other variables were not significantly associated with disclosure some of them such as starting ART, HIV stage, participation in HIV related activities are useful for disclosing of one’s HIV status to a sexual partner. Because those who started ART, who are in stage III and IV, and those who participated disclosed more frequently. The reasons for not disclosing were found to be fear of divorce, fear of breach of confidentiality, fear of accusation of infidelity , fear of stigma and discrimination and fear of physical abuse. This is also in agreement with many other studies (9, 11, 24) . Disclosure in this study was followed by positive outcomes for most of the individuals like in other studies (9, 24). Supporting people to make effective decisions to disclose their HIV serostatus should be addressed in behavioral interventions like counseling on positive living and a multidisciplinary approach to develop behavioral change through follow up counseling. In conclusion serostatus disclosure was frequent among HAART-treated patients but efforts are still needed to improve disclosure rates and prevent hetero sexual transmission in this population. The most common barriers to disclosure are fear of divorce, fear of stigma & discrimination, fear of accusation of infidelity, fear of physical abuse and fear of breach of infidelity. HIV serostatus disclosure is also associated with improved condom use. So facilitating HIV status disclosure is a key point for reducing HIV transmission. Most of the study population experienced positive outcomes after disclosure. This shows that helping individuals to disclose will help them get important services to improve their quality of life in contrary to its negative outcomes. Interventions by NGOs and government institutions on HIV shall target improved communication between patients and their spouses, notably by counseling them how to bring up conversations around HIV with family members and among themselves which will help for disclosure later on. Strengthening and reviewing the existing VCT manuals on the part of disclosure should be emphasized according to the culture of the different populations. Although the majority of participants disclosed their test results, lack of disclosure by a minority resulted in a limited ability to engage in preventive behaviors and to access support. Thus, HIV care efforts should focus on mutual disclosure of HIV test results, by encouraging individuals to ask their partner's HIV status in addition to disclosing their own. Acknowledgement The researchers would like to express their thanks to Kemissie district administrators for their cooperation in providing the necessary materials and resources for the completion of this research. We would also want to forward our heartfelt gratitude to patients and care takers included in the study. We thank the school of Public Health, University of Gondar for facilitating the ethical review process. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12011t2.jpg] [rh12011t4.jpg] [rh12011t3.jpg] [rh12011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}