 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 105-112 ORIGINAL RESEARCH ARTICLE Experiences with Provision of Post-Abortion Care in a University Teaching Hospital in South-East Nigeria: A Five Year Review Expérience concernant la dispensation de soin de post-avortement dans un Centre Hospitalier Universitaire situé au sud-est du Nigéria : Révision des résultats couvrant une période de cinq ansCollins A Kalu1, OUJ Umeora2 and I Sunday-Adeoye3 Department of Obstetrics & Gynaecology, Ebonyi State University Teaching Hospital, Abakaliki. Ebonyi Code Number: rh12012 Abstract The objective of the study was to review the implementation of Post Abortion Care and effective linkage to other post abortion services in Ebonyi State University Teaching Hospital, Abakaliki, Nigeria. Data on PAC over a five year period (July, 2004 to June, 2009) were analyzed and a standardized questionnaire was administered to 45 direct PAC service providers. Abortion complications constituted 41.4% of all Gynaecological admissions. Maternal mortality from complications of abortion was 11.5% of all the maternal mortality at the centre. Women aged 19 years and less were 37(7.1%) and single women were 132, constituting 25.3% of all cases. About 31% of the PAC care providers had formal training for the implementation of the PAC services. Fifteen percent of the care givers were satisfied with the linkage between PAC and the Family Planning services. There is poor integration between emergency post abortion care and other reproductive health services in the centre (Afr J Reprod Health 2012; 16[1]:105-112). Résumé L’étude avait comme objectif de passer en revue la mise en œuvre de soin du post-avortement et le lien efficace aux autres services de post-avortement dans le Centre Hospitalier Universitaire de l’état d’Ebonyi à Abakaliki au Nigéria. Les données sur le SPA (soin de post-avortement) au cours d’une période de cinq ans (juillet 2004 au mois du juin 2009) ont été analysées et nous avons administré un questionnaire normalisé directement aux 45 dispensateurs de services de SPA. Les complications des avortements on t constitué 41,4% de toutes les admissions gynécologiques. La mortalité maternelle causée par les complications de l’avortement était de 11,5% de toute la mortalité dans le Centre. Les femmes âgées de 19 ans et de moins étaient 37 (7,1%) et les femmes célibataires étaient 132, ce qui constituait 25,3% de tous les cas. Environ 31% des dispensateurs des SPA avaient reçu une éducation formelle pour la mise en œuvre des services des SPA. Quinze pourcent des dispensateurs ont été satisfaits du lien entre SPA et les services de planification familiale. Il y a une faible intégration entre le soin de post-avortement d’urgence et les autres services de santé de la reproduction dans le Centre (Afr J Reprod Health 2012; 16[1]:105-112). Keywords: Abortion, complications, counselling, contraception, adolescent Introduction The United Nations has identified the unacceptably high maternal mortality ratio as a major challenge of the new millennium1 Unsafe abortions account for approximately 11% of all maternal deaths in Nigeria2,3 and similar figures abound in other sub-Saharan African countries with restrictive abortion laws4,5 Globally, an estimated 40-50 Million abortions occur annually and nearly half of these are unsafe.1 In Nigeria, of the yearly 6.8 Million pregnancies, 16% end in spontaneous miscarriage and 11% as induced abortion6. Where effective contraceptive methods are available and widely used, the total abortion rate declines sharply7. In Nigeria the contraceptive prevalence is 15% 2 and this contributes significantly to the high prevalence of abortion and its complications. Post-abortion care (PAC) was introduced in public health systems around the world since the 1994 International Conference on Population and Development (ICPD) and was programmed to meet the need of abortion complications and at the same time be cost effective. The PAC concept was developed as a way to reduce maternal mortality and morbidity in settings where abortion laws are restrictive.8 The PAC Consortium updated the definition of PAC to include five elements namely, prompt treatment of women with complications of unsafe abortion using manual vacuum aspiration (MVA); contraceptive counselling and methods to help women achieve their reproductive intentions and avoid repeat unwanted pregnancies and abortions; other reproductive health services offered onsite, or through referral, as needed by women; general counselling to respond to the full range of women’s emotional and physical needs; and community and service provider partnerships to help mobilize resources for PAC and prevention of unsafe abortion.8,10,11 The PAC model is a package of interventions that should be implemented as a whole.12 Studies and anecdotal evidence have exposed the poor quality of such care and this is related in large part, to abortion-related stigma. This is much more in low-resource countries like Nigeria where restrictive law on abortion still operates. Health care providers still display negative attitudes to women with abortion and abortion complications in most health settings.12,13 The PAC model calls for changes in provider attitudes and practices so that women receive timely and humane treatment. PAC can be offered as an ambulatory service at all levels of care and can be provided by a range of cadres of health workers.10 Systematic linking up of emergency services in post abortion care with contraceptive services, reproductive health counselling and community partnership with service providers are some of the areas of service delivery in the PAC model that have not been effectively implemented in most health facilities. In Enugu, south-east of Nigeria, it was reported in a study by Onah et al that 25% of the doctors working in private hospitals offered an all inclusive post abortion care, 46.9% of them had received formal training in the use of MVA in post abortion care and 33.3 % had actually used the instrument.14 This confirms the assertion by Ibekwe PC in his commentary on post abortion care, writing from Abakaliki in the same region of Nigeria that PAC is the least emphasized aspect of reproductive health in Nigeria.15 The Ebonyi State University Teaching Hospital Abakaliki has provided emergency care to women experiencing unsafe abortion complications from its inception. The Ipas in collaboration with the hospital management introduced PAC model in 2002 to the Department of Obstetrics and Gynaecology furnishing a manual vacuum aspiration room. This study attempts to analyze the implementation of the PAC model in the facility as well as to review the degree of systematic linkage of the five elements of the delivery of post abortion care services in women that have complications from induced or spontaneous abortion. Methods Study Background The Ebonyi State University Teaching Hospital is a tertiary health care facility accredited for both the undergraduate and postgraduate medical training. It serves as a prime referral centre to the State and her neighbours. The obstetrics and gynaecology department is fully staffed by all cadres of care providers. It has a 24-bed gynaecological ward, routine and emergency clinics and a manual vacuum aspiration (MVA) room and a theatre suite. Women presenting with post abortion complications are usually seen at the Emergency clinics where they are properly evaluated, undergoing in depth clinical history and vaginal examination. Where indicated appropriate resuscitative measures are instituted and laboratory investigations performed. Minor cases requiring evacuation of products of conception are handled in the MVA room immediately on admission. Both the MVA room and the Family planning unit are located within the Antenatal clinic complex. The patients are usually seen by the Senior house Officers and then subsequently reviewed by the registrar. More complicated cases are handled by the senior registrars and Consultants. All women that need evacuation of retained products of conception are treated with the MVA instrument. They were usually discharged within 24 to 36 hours and subsequently managed on outpatient basis with follow up in the clinics. Patients with more serious complications are admitted into the gynaecological wards and managed according to departmental protocol. Study design The preliminary part of this descriptive study was a review of restrospective data on women with post abortion complications who received post abortion care in the Department of Obstetrics and Gynaecology from 1st of July, 2004 through 30th of June, 2009. The PAC outpatient register and the gynaecological ward admission register were reviewed. To ensure the accuracy of the information obtained from the registers, the researchers went through the registers themselves and extracted all the information needed and recorded same in a preformed data proforma. The information was equally crosschecked with a similar record that is recorded for the purpose of submission to the IPAS consortium that comes to the unit monthly for monitoring and evaluation. The information obtained from the Registers and case notes included the demographic characteristics of the women (age, marital status, parity and level of education), type of post abortion complication, abortion related maternal mortality, knowledge and usage of contraceptives, type of post abortion care given, duration of hospital admission and the cadre of the most senior PAC provider that attended to them. Those women that were discharged within 24 hours from the PAC Room were considered as being managed as PAC outpatients. The various types of abortion were categorized as follows based on the clinical history;16
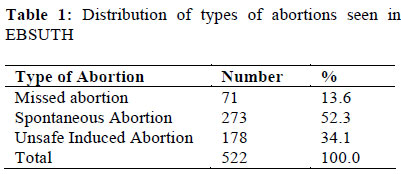
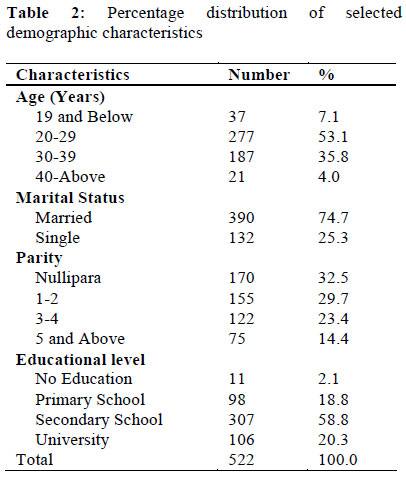
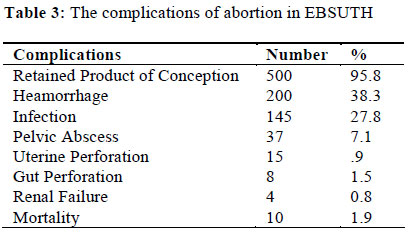
The final aspect of this study was the evaluation of a questionnaire-based data from the PAC service providers transcending all cadres of staff in the department. The items in the questionnaire related to their assessment of the effectiveness of the PAC model in Ebonyi State University Teaching Hospital and its degree of systematic integration of the emergency treatment of complications of abortion to the other packages of PAC. The various types of abortions were categorized into three major clinical types; missed abortion, spontaneous abortion and induced (septic) abortion and their percentages were calculated. The demographic characteristics of the women were equally reviewed and their frequencies and percentages were calculated and presented in a simple frequency table. The mean age and standard deviation was calculated using the Epi info statistical software. The type of abortion complication and the associated interventions were categorized and presented in a simple frequency tables. The questionnaire data which needed a yes or no answer from the service providers were similarly analysed. Results During the five year study period, one thousand, three hundred and forty four (1,344) gynaecological cases were admitted and of these, five hundred and fifty six (556) were abortion complications. This represented 41.4% of all gynaecological admissions. Five hundred twenty two (522) cases had complete data and were analyzed. Missed abortions were 71(13.6%), spontaneous abortions 273 (52.3%) and unsafe induced abortions complications accounted for 34.1% (178) (Table 1). The total number of maternal deaths related to complications of abortion were 10 and these represented 1.9% of all cases of abortion complications treated in the hospital during this period, and constituted 11.5% of all maternal deaths during this period. The age range of the patients was 15 to 48 years, with a mean of 26yrs. (SD +2). Those between the age of 20 and 29 years were 277, constituting 53.1% all cases while those 19 years and below were 37(7.1%). Married women were 390 (74.7%). The rest were unmarried. Thirty-two point five percent of the subjects were nulliparous women. Majority (58.8%) of the women with complications of abortion attained the secondary level of education. Eleven women (2.1%) women had no formal education. (Table 2). Among all the women that presented with complications of abortion none was using any method of contraception at the time of the index pregnancy, but 429 women (82.2%) were aware and never used any method of contraception in the past. Only 51(9.8%) women had used any modern method in the past while 42 (8.0%) women had no knowledge of contraception at all. The commonest complication of abortion observed in this study was retained product of conception (incomplete abortion) and this was seen in 500 women (95.8%), heamorrhage was seen in 200 women (38.3%), septic incomplete abortion were 145(27.8%), Pelvic abscess were 37(7.1%), Uterine perforation were 15(2.9%) and Gut perforation were 8(1.5%) (Table 3). Specialist Gynaecologists attended to 139(26.6%) women with complications of abortion. Senior Registrars attended to 92(17.6%), Registrars 224(42.9%) and Senior House Officers 67(12.9%) women. Of the 522 women, 289 patients (55.4%) were in -patients while 233(44.6%) were treated in the MVA room and discharged within 24hours. The commonest intervention offered the patients was Manual Vacuum Aspiration (MVA) and this was used to treat 500(95.8%) patients. All the patients received Antibiotics according to the departmental policy, 40 women (7.7%) had blood transfusion while 42(8.0%) women had laparatomy because of pelvic abscess gut perforation and uterine perforation. The duration of hospital stay of the in-patients ranged from 2 – 59 days, with a mean of 7.7 days (SD + 2.2 days). The total number of days spent by all the in -Patients was 2,247 days. Out of the 522 patients managed in this facility 219(42%) women were counselled on various modern methods of contraception and 84 (16%) were referred to the family planning clinic for uptake of their method of choice and other reproductive health needs. An appraisal of the PAC package in Ebonyi State University Teaching Hospital by the Doctors and Nurses who provided the post abortion care showed that 80%(32) were aware of a well defined programme on post abortion care while 20%(8) see it as just one of the routine care provided by the hospital. It was significant to note that only about 31% (12) of the PAC care providers had any form of formal training for the implementation of the total package of the PAC programme and these were mostly the Consultants and the senior registrars in the department of obstetrics and gynaecology. Of the PAC care givers 80% believed that the programme has reduced the maternal mortality in the hospital. Another significant finding of this study is that only 40% of the care providers integrate prompt treatment with the counselling for contraception and other reproductive health services. Only 15% (6) of the care givers are satisfied with the linkage between PAC and the Family Planning services in Ebonyi State University Teaching Hospital (Table 4). The study also showed that 62.5 %( 25) believed that PAC in the hospital is not adolescent and single women friendly, as evidenced by lower number of single women that utilize the facility. 82.5% (33) of the service providers are of the opinion that partnership between the PAC and the community is poor. Of the 40 service providers who assessed the PAC project in the hospital, 67.5 %( 23) said that the MVA room, MVA equipment and the ancillary facilities were inadequate. Only 47.7% (19) care providers think that the PAC programme as it is currently being implemented in Ebonyi State University Teaching Hospital is satisfactory. Discussion Complications of unsafe abortion account for 11% of maternal deaths in Nigeria.2 Other complications of abortion include pelvic sepsis, septicaemia, haemorrhage, renal failure, uterine perforation and other genital tract injuries, and gastro-intestinal tract injuries. These levels of mortality and other post abortion complications tend to occur together with restrictive abortion law.17 In this study there were 10 maternal deaths and these constituted 11.5% of all maternal death during this period and compared with the results of previous studies by Aboyeji who recorded 14.8%.17 and 13% at Ilorin Nigeria. This level of mortality from complication of abortion is unacceptable in a tertiary institution in the 21st century considering the publicity and global investment that has been put into reproductive health in the past two decades. It is worthy of note that, of the ten women that died six of them were single, seven died from severe sepsis and three died from acute renal failure. Sadly too all the mortality cases presented late to the hospital. I believe that the reasonable solution to these unnecessary deaths is primary prevention, using effective contraception. The bed occupancy rate for abortion related pathologies was high in this study as it accounted for 41.37% of all gynaecological admissions, higher than 20.2% recorded in a similar tertiary centre in Ibadan Nigeria18 and 25.1% in Abeokuta19 . It was however significantly lower than 60% of gynaecological admissions in Kenyatta National Hospital Nairobi Kenya and conversely; unsafe abortions have almost been eliminated in Great Britain.20 This study also highlighted the fact that significant number of man hour is lost daily in the hospital as a result of complication of abortion. The average number of days spent on admission by the Patients is 7.7 days and the total number of days for all the patients is 2247 days, these translate into a significant economic loss to the individual, family and society. Complications of abortion therefore, still remain a major reproductive health problem in the south-east of Nigeria and this is unacceptable. One of the significant findings in this study was that majority of the women that received PAC were married, constituting 74.7 %( 390) as against 25.3 %( 132) of single women that received care in the hospital. Also the study showed that only 7.1 %( 37) of all the cases were below the age of 20 years. This finding is much lower than the findings of Emuveyan in Lagos who recorded 33.4% teenage involvement21 and the study in UCH Ibadan by Konje and Obisesan where teenage girls constituted the single largest group of patients involved in abortion complications.18 Among the married women who had complications of abortion, the finding of Emuveyan in Lagos (61.1%)21 differed significantly with the findings in this study . But the study by Fawole in Sagamu is similar to our finding as it showed a greater prevalence of among married women (52.4%), while 42.9% were single women20 . These finding showed that PAC in Ebonyi State University Teaching Hospital seems to be missing some of the major target group for post abortion care, which is the unmarried teenage girls who are more prone to the complications of abortion from other studies, as this study equally showed that out of the 10 deaths from abortion six, were single women. The above finding was corroborated by 62.5 %( 25) of the service providers who believed that PAC in the hospital was not adolescent and single women friendly. However a survey on the perception of the adolescents of the post abortion services at the centre would be worthwhile. The above findings may have resulted from an unfriendly attitude of the care givers toward the single women or due to lack of awareness that the hospital offers such service to single teenage girls. Also the fact that the MVA room is located within the antenatal clinic complex might have been contributory. One of the ways of improving the quality of care given to women with complications of abortion is to have a regular auditing of the project implementation and updating the technology being used.1 Forty service providers who assessed the PAC project in the hospital, 67.5 %( 23) said that the MVA room, the MVA instrument and the other facilities were inadequate. This of course may have affected the quality of care delivered by the providers. Only 47.7% (19) care providers think that the PAC programme as it is currently being implemented in Ebonyi State University Teaching Hospital is satisfactory. The performance of the programme in the hospital may have been affected also by the fact that only 30.8% of the care providers had any formal training on the implementation of the integrated PAC model and these were the Consultants and the Senior Registrars. Most of the Registrars and Senior House Officers have not had any formal training. It is interesting to note that only one Nurse in the Gynaecological clinic and ward had any form of training. This lack of training and retraining of staff seem to be a major drawback in the implementation of the post abortion care in this hospital. This study has shown that the first element of the PAC model has fairly been implemented in Ebonyi State University Teaching Hospital as in most health facilities where it has been introduced, which is prompt treatment of the abortion complication. However, linking contraceptive and other reproductive health services as well as counseling on physical and emotional needs of the woman and community partnership with the service providers; with emergency services is advocated in order to meet women’s full range of health needs.8,22 has been grossly inadequate as shown by this study. Only 40% of all the PAC care givers said that they always give contraceptive advice and methods as well as other reproductive health counseling following treatment of abortion complications and 42% of the patients received contraceptive counseling in this facility. Sixteen percent of the patients were referred to the family planning unit following treatment and only 15% of all the service providers are satisfied with the integration between PAC and family planning services in Ebonyi State University Teaching Hospital. Another interesting finding is that 82.5% of the care givers believe that there is a very poor partnership between PAC and the community in terms of funding and general public awareness. These may be difficult in the Nigerian society where abortion is apparently clandestine and frowned by the public. The effective implementation and integration of these five components of PAC will ensure secondary prevention of maternal mortality, unwanted pregnancy and unsafe abortion, which are the cardinal focus of reproductive health.10 These all important links seem to be lacking in our PAC package due to poor conceptualization of the model in the institution, resulting from lack of training and retraining of the service providers. This study has identified two major challenges in the PAC implementation in Ebonyi State University Teaching Hospital, which are failure to impact maximally on the most vulnerable target group, which are the unmarried and the teenage girls and failure to integrate the emergency care with other PAC components, especially contraceptive services. It is therefore recommended that: PAC be made more adolescent and single women friendly by relocating the MVA suite from the antenatal clinic to the adolescent clinic or to the Accident and emergency department or even outside the hospital; vigorous health education in the schools on the need for early presentation to the hospital following complications of abortion be pursued; institutionalization of PAC in Ebonyi State University Teaching Hospital; which refers to the establishment of a sustainable integration of PAC into existing health systems as part of their regular service delivery be implemented; regular formal training of younger Doctors and Nurses and retraining of older PAC providers to ensure that skills and concept of the model is passed on from generation of care givers to the next; the administrative segmentation and bureaucratic differences between the Family Planning unit and the PAC unit be abolished; collaboration with the community should be strengthened through formal partnerships and strategic alliances between local NGOs, international NGOs and public health institutions to facilitate the efficient use of scarce human and financial resources. And where possible the PAC services should be made free or affordable to the poor and unemployed. Some of the limitations of this study include the inability of the research to cover the opinion of the post abortion patients and make assessment of their care in Ebonyi State University Teaching Hospital. Another important limitation on this study was that the various types of abortion were not separated and stratified before the analysis. Conclusion Post abortion care is one of the most important secondary preventive measures in Reproductive Health which if strategically implemented in an integrated form will impact on the health of women positively by significantly reducing the maternal mortality and morbidity due to abortion complications, reduce the incidence of repeat unwanted pregnancies and abortion, as well as enhance the use of desired contraceptive methods among women with complications of abortion. Regrettably, in this tertiary health care institution there is poor integration between emergency post abortion care and other reproductive health services in the centre. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12012t3.jpg] [rh12012t2.jpg] [rh12012t4.jpg] [rh12012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}