 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
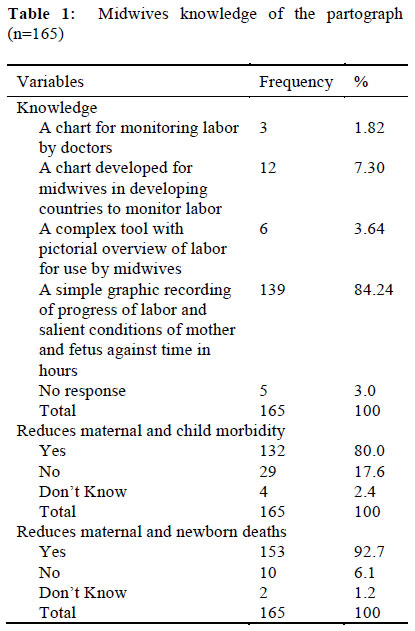
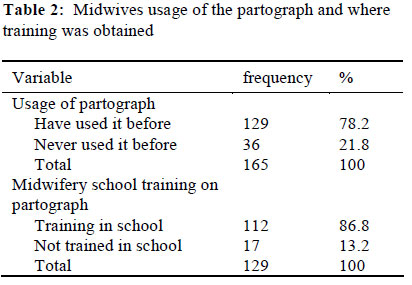
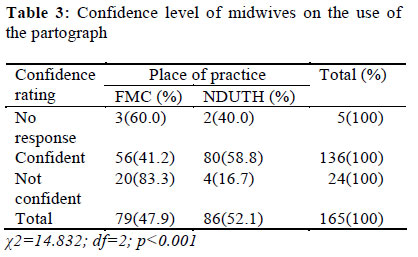
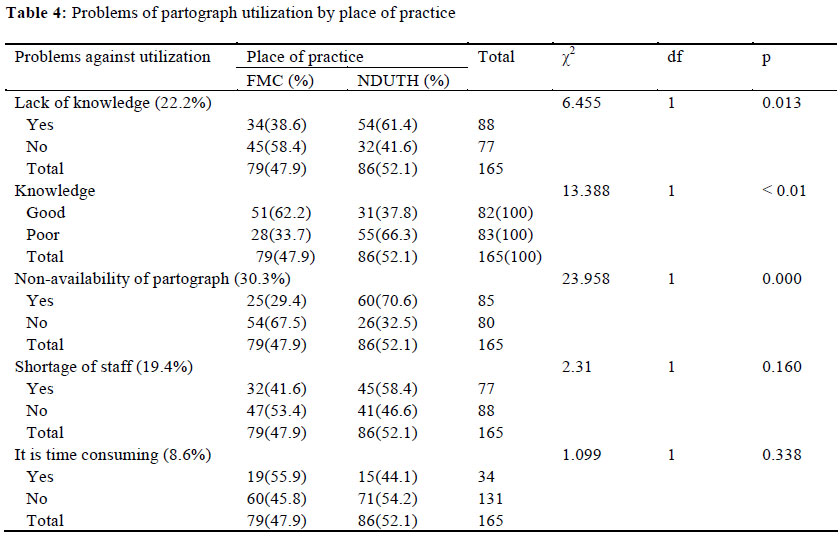
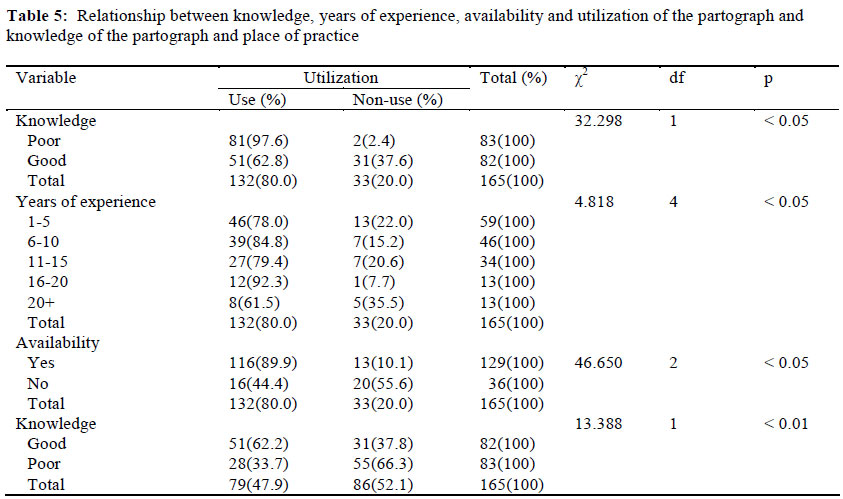
African Journal of Reproductive Health, Vol. 16, No. 1, Mar, 2012, pp. 125-132 ORIGINAL RESEARCH ARTICLE Knowledge and Utilization of the Partograph among Midwives in the Niger Delta Region of Nigeria Connaissance et utilisation de la partographie chez les sages-femmes dans la région de Niger Delta du NigériaMargaret M Opiah1*, Abosede Bola Ofi2, Ekere James Essien3 and Emmanuel Monjok3 1Department of Maternal and Child Health, Faculty of Nursing, Niger Delta University, Bayelsa State, Nigeria; Code Number: rh12014 Abstract This cross-sectional study assessed knowledge and utilization of the partograph among midwives in two tertiary health facilities in the Niger Delta Region of Nigeria. A descriptive survey design was utilized, using a structured questionnaire administered to 165 midwives purposively selected from the Federal Medical Center (FMC) (79) and Niger Delta University Teaching Hospital (NDUTH) (86). Results revealed that 84% of midwives knew what the partograph was and 92.7% indicated that the use of the partograph reduces maternal and child mortality. About 50.6% midwives in FMC and 98.8% in NDUTH indicated that it was routinely utilized in their centers. Assessment of utilized partograph charts revealed that only 18_ (37.5%) out of 48 in FMC and 17_ (32.6%) out of 52 in NDUTH were properly filled. Factors in the utilization of the partograph were:-non-availability of the partograph (30.3%), shortage of staff (19.4%), little or no knowledge in the use of the partograph (22.2%), and 8.6 percent indicated it was time consuming. A significant relationship existed between knowledge of the partograph and its utilization (χ 2 = 32.298. Df = 1; P <0.05) and between midwives years of experience and its utilization (χ 2=4.818, Df = 4; P <0.05). However, this study also showed that despite midwives good knowledge of the partograph, there was poor utilization in labor monitoring in both centers. Training of midwives on the use of the partograph with periodic workshops and seminars and a mandatory hospital policy are recommended and vital to the safety of women in labor in the Niger Delta region of Nigeria (Afr J Reprod Health 2012; 16[1]:125-132). Résumé Cette étude transversale a évalué la connaissance et l’utilisation de la partographie chez les sages-femmes dans deux établissements de santé tertiaires dans la région de Niger Delta du Nigéria. Nous nous sommes servis du modèle de l’enquête descriptive à l’aide d’un questionnaire administré auprès de 165 sages-femmes délibérément sélectionnées à Federal Medical Centre (FMC) et au Centre Hospitalier Universitaire de l’Université de Niger Delta (NDUTH) (86). Les résultats ont révélé que 84% des sages-femmes connaissent la pantographie et 92,7% ont déclaré que l’utilisation de la partographie réduit la mortalité maternelle et infantile. Environ 50,6% sages-femmes dans le FMC et 98,8% dans NDUTH ont dit qu’elle est utilisé de routine dans leurs centres. L’évaluation des chartes de la partographie ont révélé que seulement 18 (37,5%) sur 48 dans le FMC et 17 (32,6%) sur 52 dans la NDUTH étaient bien remplies. Les facteurs dans l’utilisation de la partographie étaient la non-disponibilité de la partographie (30,3%), le maque de personnel (19,4%) peu ou pas de connaissance du tout à l’égard de l’utilisation de la partographie (22,2%) et 8,6 pourcent ont déclaré que cela prend beaucoup de temps. Il existait un rapport significatif entre la connaissance et son utilisation (x2 =32, 298. Df =1 ; P <0,05) et entre les années d’expérience des sages-femmes et ses utilisations (x2 = 4,818, Df = 4 ; < 0,05). Néanmoins, cette étude a également montré que malgré la bonne connaissance qu’ont les sages-femmes de la partographie, il y avait une faible surveillance du travail dans les deux Centres. Nous recommandons que les sages-femmes apprennent à utiliser la partographie à travers des ateliers périodiques et des séminaires et à travers une politique hospitalière obligatoire, ce que nous considérons comme étant essentiel pour la sécurité des femmes pendant le travail dans la région du Niger Delta du Nigéria (Afr J Reprod Health 2012; 16[1]:125-132). Keywords: Knowledge, utilization, partograph, midwives, labor monitoring, Niger Delta, Nigeria Introduction Each year 210 million women become pregnant of which 20 million experience pregnancy related illnesses. Also, approximately, over half a million women lose their lives every year because of complications of pregnancy and childbirth. In developing countries, poor outcomes during labor account for 99% of maternal deaths and for every 100,000 live births an average of 450 women die. 1 Despite the continued focus on the reduction of maternal mortality by stakeholders and the development partners, it still remains a major public health problem in sub-Saharan Africa, particularly in Nigeria.2 In Nigeria, figures on maternal mortality rate (MMR) are mostly institutional. They vary from one geographical zone to another and are worse in the rural, when compared to the urban areas.2 Available data show that MMR, in the early 1990s, was 1400 – 1500/100,000 live births. This however dropped to 1000/100,000 live births in the late 1990 and dropped further to 704/100,000 live births in 1999 and 800/100,000 in 2002. There was an increase in 2005 to 1100/ 100,000 live births, 3 but the current estimates (2011) by the WHO is 840/100,000 live births. 4 There are regional variations in maternal deaths in Nigeria with the highest prevalence in the North East (1716/100,000) and Northwest (1210/100,000) compared to the South East (497/100,000) and South West (339/100,000). There is also more maternal death in the rural areas (1500/100,000) than in the urban areas.2 Agboola 5 observed that despite the safe motherhood campaign, the maternal mortality ratios for most developing countries including Nigeria, Cameroun and Sierra Leone are still on the increase. In Bayelsa state in the Niger Delta region of Nigeria, available statistics show that approximately 350 – 360/100,000 of women die from labor related complication at the Federal Medical Centre (FMC) and Niger Delta University Teaching Hospital (NDUTH), both in Yenegoa, the capital city of Bayelsa State.6 Also, some 60 – 65% of pregnant women were at risk of dying during childbirth mainly from preventable and avoidable conditions and complications. 6 Majority of these deaths could have been prevented by early detection of abnormal progress of labor with the use of the partograph which is a cost-effective and affordable health intervention.7-9 In addition; the early detection of obstructed labor with the use of the partograph prevents maternal morbidity and improves neonatal outcomes. 7-9 The use of the partograph for labor monitoring was adopted at the FMC and the NDUTH in 2002, but available data from the Ministry of Health, Bayelsa shows that there was no significant reduction in maternal mortality ratio after the adoption as revealed by the post-evaluation survey conducted in 2006. The observation of clinical midwifery practice within the maternity unit of the FMC and NDUTH by one of the researchers (MMO) revealed a haphazard utilization of the partograph in labor monitoring, a driving force for this study. Most studies on the partograph in Nigeria have been reported from the South West and South East zones. 10-14 Both zones are more endowed with health manpower and have lower MMR than the Niger Delta zone, the North East and North West zones.2 This is the first study on knowledge and utilization of the partograph among midwives in the Niger Delta region of Nigeria to the best of our knowledge. The partograph is a graphic recording of progress of labor and salient conditions of the mother and fetus plotted against time in hours. 7-9 When used effectively, the partograph will prevent prolonged or obstructed labor, which accounts for about 8-10 % of maternal deaths.8,9 It was originally produced by Philpott and Castle in 1972, and later modified and adopted by the WHO in 1988 7 and recommended for worldwide use in all healthcare settings. It is more commonly used in tertiary than in primary and secondary health care centers in Nigeria and in other developing countries. Several factors affecting the utilization of the partograph include poor knowledge, 5, 10-12 non-availability of the partograph charts in the labor wards, 11, 12 lack of adequate number of health care personnel, 11 an additional timeconsuming task for the inadequate staff 15, lack of understanding of the relevance of the partograpgh in preventing obstructed labor. 12 Other factors include lack of standard institutional guidelines on the use of the partograph in labor, 11 lack of support from management in terms of providing essential supplies, 16, 17 leading to lack of motivation of the health workers. 15 The aim of this study was therefore; to determine midwives’ knowledge about the use of the partograph during labor, compare the extent of use of the partograph among midwives in the two hospitals, identify level of utilization in each centre, identify factors that hinder it use, find out the relationship between the years of experience and knowledge of the use of the partograph in the two hospitals. Methods The study was conducted among midwives in the FMC and NDUTH, both tertiary hospitals in Bayelsa State in the Niger Delta Region of Nigeria. An exploratory and descriptive survey was used to study the knowledge and utilization of the partograph in labor monitoring in the labor wards of the two tertiary hospitals. The Federal Medical Centre is a 100-bed hospital with current staff strength of 772 which includes 138 registered nurses/midwifes (RN/RM). This Federal Government institution serves as a referral center providing specialized medical services for the entire State. The NDUTH is also a tertiary hospital and academic medical center of the Niger Delta University owned and funded by the Bayelsa State government. It is a 110-bed hospital with staff strength of 982 including 137 RN/RM. Both hospitals are situated in Yenogoa, the capital city of Bayelsa State. The target population was all practicing midwives (total 275) working in the gynecology/obstetrics units and labor wards in the two tertiary hospitals. Only 165 midwives (60%) in the two hospital settings were available for the study. The inclusion criteria was registered midwives of the rank of Nursing Officer level II (Staff Nurse/Midwives) and above with at least one year of experience in the obstetric and gynecological wards/units. Out of the 165 midwives, 86 were selected from the NDUTH while 79 were from the FMC. Purposive sampling technique was used. A structured questionnaire divided into four sections with open and close-ended questions was used for this study. Section 1: included questions that elicited information on the socio-demographic characteristics of the respondents. Section 2: included questions on the knowledge level of the respondents on the use of the partograph in labor monitoring. Section 3: contained items that elicited information on respondent’s willingness to use the partograph in their management of women in labor and in section 4, questions were designed to identify factors affecting the use of the partograph in the two hospitals. Test-re-test reliability test was carried out to ensure that the questionnaire will consistently measure what it intends to measure. This was done by using the instrument in a pilot study with ten midwives at the Federal Medical Centre, Asaba, Delta State (a neighboring state in the Niger Delta Region). The instrument was re-administered on the same set of midwives one week after the first administration. The analysis of the two set of questionnaires revealed a reliability coefficient of 0.89 at an alpha level of 0.05. In order to produce a more objective assessment of knowledge of the partograph and its level of utilization, a scoring method was devised and a knowledge score for each of the respondents was obtained by adding up the scores for correct answers given to questions under Section 2 of the questionnaire. A score of less than 50 indicates poor knowledge, while a score above 50 indicates good knowledge. Fifty (50) properly filled partograph charts were used for this analysis. Ethical approval for the study was given by the ethical committees of the FMC and NDUTH. A written informed consent was also obtained from each participant. The data entry and analysis were performed using SPSS version 14. Descriptive statistics such as frequencies, percentage, means and charts were used. Chi-square and student ttest statistical methods were used as appropriate. All results were confirmed at 0.05 level of significance. Results One hundred (100) partograph charts were retrieved from the two hospital records. Fifty charts (26 from NDUTH and 24 from FMC) were properly filled by the attending midwife. Therefore, only 50 properly filled partograph charts were analysed. The result showed that 84.2% of midwives studied were aware of the partograph and 153 (92.7%) of the midwives agreed that the use of the partograph would increase efficiency of labor monitoring (Table 1). Also, 84.8% of respondents agreed, that the use of the partograph is necessary to improve the quality of care, 17 (10.3%) disagreed while 8 (4.8%) did not know. Also, out of 165 respondents, 78(47.3%) knew the exact function of the partograph compared to 21(12.7%) who said it allows time for the woman to be adequately assessed for appropriate intervention and 39 (23.6) who reported that it was for continuous observation till delivery. About 55% of respondents agreed that action line of partograph plot falls on the left of alert line, 51 (30.9%) disagreed while 22 (13.3%) do not know. The result further indicate that out of 165 respondents, 80 (48.5%) agreed that it would fall on the alert line, 38.8% disagreed while 12.7% did not know. Moreover, 35.8% agree with the view that graph would plot on the right of alert line, 52.1% disagreed while 12.1% did not know (not shown). The majority 129 i.e 78.2% actually reported having used a partograph before while 36 (21.8%) indicated never used it before. One hundred and twelve (112) of them (86.2%) had partograph training while in school of midwifery, 13% said they were not trained in the midwifery school (Table 2). Seventy four (44.5%) reported being very confident in the use of partograph, 62 (57.6%) were fairly confident while 24 (14.5%) were not confident (Table 3). Eighty (58.8%) midwives who had confidence in the use of the graph were from NDUTH and 56 (41.2%) were from FMC. Only 20(83.3%) from FMC and 4(16.7%) from NDUTH, indicated not confident in the use of the partograph(Table 3). In addition, 129(78.2%) agreed that partograph was available in their labor ward, 26(15.8%) disagreed while 10(6.0%) did not even know. (not shown). One hundred and twenty three (74.5%) agree with the view that partograph is used to monitor women during labor, 32(19.4%) indicated that it is not utilized in labor monitoring while 10(6.1%) made no response.(not shown). Forty (50.6%) in FMC, 85(98.8%) in NDUTH indicated that partograph is used routinely to monitor patients during labor, 5(6.3%) in FMC and none in NDUTH maintained that it is used occasionally while 6(7.6%) in FMC, none in NDUTH noted that it is rarely used. Of those who said it was routinely used 96% said that partograph was used routinely to monitor every woman in labor, 27(16.4%) disagreed while 18(10.9%) did not know (not shown). Only 18(37.5%) out of 48 partograph charts in FMC and 17 (32.6%) out of 52 in NDUTH were properly filled while 30(62.5%) in FMC and 35(67.3%) in NDUTH were poorly filled. One hundred and two (61.8%) said it is used hourly while 40 (24.2%) had no response on how often partograph is used, while 23 (13.9%) said 4 hourly (not shown). The analysis also indicates that out of 165 respondents, 148 (89.7%) agreed that partograph is useful in obstetric review, 11(6.7%) disagreed while 6(3.6%) did not know. Findings also indicate that out of 165 respondents, 117 (70.9%) agreed that it is a managerial policy, that all women in labor should be monitored, 30 (18.2%) disagreed while 18 (10.9%) did not know. The identified factors hindering utilization of the partograph were non-availability of the partograph (30.2%), lack of knowledge of the partograph (22.2%), shortage of staff (19.4%), and the reason that it is time consuming (8.6%)(Table 4). Lack of knowledge (χ2 =6.455, Df=1, p <0.01) and nonavailability (χ2 =23.958, Df=1, p=0.000) of partograph had a significant relationship with the place of practice. (Table 4). It was noted that of the 88 respondents who reported that lack of knowledge was a problem facing the utilization of the partograph , 61.4% were from the NDUTH while only 38.6% from the FMC. Similarly, 67.5% of the 85 who saw non-availability of the partograph as a problem in its utilization were from the FMC while 32.5% came from NDUTH. Shortage of staff, FMC (41.6%), NDUTH (58.4%) while 55.9% in FMC and 44.1% in NDUTH says it is time consuming (Table 4). There was a significant relationship between the years of experience of midwives (χ2=4.818, df=4, p<0.05), knowledge of the use of the partograph by midwives in the two hospitals (χ2=32.298, df=2, p<0.05), availability of the partograph (χ2=46.650, df=2, p<0.05) and utilization of the partograph (Table 5). Majority of the midwives were in the group of those who had practiced between one to ten years and were less experienced. A total of 15.8% had spent from 16 years and above in clinical practice. It is interesting that a huge percentage (89.7%) consider the partograph useful in obstetric and gynecological reviews. Discussion This study was focused on midwives at the tertiary level of health care in Bayelsa State to gain an insight into their management of labor since this is crucial to safe motherhood in Nigeria especially with the high levels of maternal mortality. Midwives form the bulk of the skilled birth attendant in all levels of health care; therefore their knowledge on partographic labor monitoring is a significant factor for prevention of obstructed labor. This study shows that midwives’ knowledge about the partograph is a significant factor in its utilization in monitoring labor. Despite the good knowledge of the partograph, there was poor utilization in labor monitoring. Several and similar studies in Nigeria confirmed the low utilization of the partogram.5, 10, 11,13 Inadequate knowledge and utilization of this simple tool could be part of the reason for the high MMR in Nigeria and other developing countries. There was a significant relationship between the years of experience of midwives and their use of the partograph. The introduction of the partograph and its use should be an organizational (hospital) policy that has to be carried out regardless of midwife years of experience. This finding is similar to other studies which found support for the relationship between knowledge and the utilization of any relatively new policy.18 Watson 18 indicated that unless a midwife learns from experience, the learning would not be adequate. He asserts that experience is usually measured quantitatively in terms of time, whereas it would be better to look at experience qualitatively in terms of the quality of experience and the amount of learning that took place. In this regard, it may take time for midwives to gain experience on the use of the partograph even after it is a newly introduced hospital policy. The utilization of the partograph is significantly related to staff strength as shown in this study. It is probably as a result of staff shortages that some midwives consider the use of the partograph as a waste of valuable time. Sara and Alice 15 showed that some midwives often think that completing the partograph is an additional time-consuming task and as such have no understanding of how it can save a woman’s life. So, the more midwives there are per shift, the more likely that they will complete the graph during labor, Moreover, MacArthur et al,19 found that though midwives find the partograph to be of practical use and advantageous, its status within some obstetric units is restricted in terms of utilization. Some researchers have also identified shortage of staff as one of the biggest constraints in most health institutions.11, 15 The few midwives on duty are faced with so much responsibilities on a shift that some important aspects of midwifery care are haphazardly done or not done at all. This could be one of the reasons why a large number of utilized partograph charts assessed in the study settings were poorly filled. This analysis showed that there is indeed a significant relationship between the availability and utilization of the partograph. Dujardin et al 17 had found that lack of support from management in terms of providing the essential supplies and equipments including the provision of partograph charts for use by midwives are profound problems in the adoption and utilization of the partograph. It is possible that the respondents actually experienced the same limited resource situations in both hospitals and that the availability of partograph in the labor wards did play a significant role in determining its utilization in the monitoring of labor. Umezulike et al 12 in their study in Enugu reports that, a proportion of respondents who despite acknowledging it usefulness, revealed nonavailability of the partograph in their maternity unit. In this study, 67.5% in FMC and 32.5% in NDUTH acknowledged the problem of nonavailability of the partograph in their labor room. Despite the various factors affecting utilization, there is evidence to show that the partograph can be effectively used in developing countries. An audit of partograph use in a Nigerian tertiary hospital revealed universal application for all parturient women, satisfactory recording of information and its significant influence on decision making.13 The sad outcome is that this tool is not uniformly utilized in setting where it is most needed at the peripheral health and maternity centers, secondary health hospitals and private health institutions, where most skilled birth attendant are lacking or poorly trained.11, 16 Maternal mortality is a serious public health problem in Nigeria. The Federal Government has responded by scaling up midwives and recertification of retired midwives as a way of alleviating this serious crisis. It is therefore imperative that greater attention should be given to the use of this simple tool in labor monitoring according to WHO recommendation.7 so that the majority of complications and deaths that occur during childbirth in Nigeria would be reduced leading to improvement in maternal and child morbidity and mortality situation in the country. This should be a national emergency and policy makers should make sure all health centers adopt the partograph as an institution policy. The limitation of this study is the small sample size of midwives and the fact that the selected health facilities were both tertiary level hospitals. Both factors may introduce some bias in the findings. A more comprehensive study should include midwives working in primary health care maternity units, secondary health care general or community/cottage hospitals and private health institutions. Despite the limitations, the findings may be useful to health care professionals, program managers and policy makers. The following recommendations are therefore made; the training of midwives in partographic labor monitoring should be mandatory in all schools of nursing and midwifery. Periodic workshops and seminars should be organized for midwives and other healthcare providers on the use of partograph in assessment and monitoring of labor and all registered midwives must always renew their knowledge through continuous education. The hospital management should put in place a hospital practice guideline on the use of partograph and also make sure the charts are provided in all labor and maternity units. In summary, a significant percentage of midwives in the two tertiary hospitals have adequate knowledge of the partograph and why it is necessary to use it in the management of labor. However, despite adequate knowledge by midwives in this study a large percentage of the chart assessed were poorly filled. Midwives’ years of professional experience was significantly related to their adoption and utilization of the partograph. Availability or non-availability of guidelines for the use of the partograph did not show any significant influence on midwives’ utilization of the method in managing labor, a significant percentage thought that using the partograph would significantly improve the maternal and child mortality/morbidity situation in the country. It was also found that larger staff strength made it easier to utilize the graph when it was made available in the obstetric units/wards. The findings in this study could be useful in designing professional continuing education programs for midwives as well as formulating policies that will reflect on the delivery of professional midwifery in Nigeria. Acknowledgement The authors are grateful to the management of the NDUTH and FMC and to all the midwives who participated in this study. We are also thankful to Dr. A.O. Fawole, Consultant Obstetrician and Gynecologist and Professor A.A. Ojo, Professor of Nursing, both of the University of Ibadan College of Medicine at the University College Hospital, Ibadan for their specialist and technical advice through-out the study period. References
Copyright 2012 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh12014t2.jpg] [rh12014t3.jpg] [rh12014t5.jpg] [rh12014t1.jpg] [rh12014t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}