 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 1, No. 1, 2003, pp. 33-36 The Chromosomal Abnormality of Failed Fertilized Human Oocytes in an In Vitro Fertilization Program Seyed M. Kalnatar Ph.D. 1 Ahmad Ebrahimi B.S., Mehrdad Solimani, Hossein Fazli Research & Clinical
Centre for Infertility, Medical Sciences University, Yazd Iran. Code Number: rm03008 Background: The high fertilization failure after IVF treatment
cycles could be related to chromosomal abnormalities. This study was carried
out to assess the frequency of chromosomal abnormality on human oocytes lacking
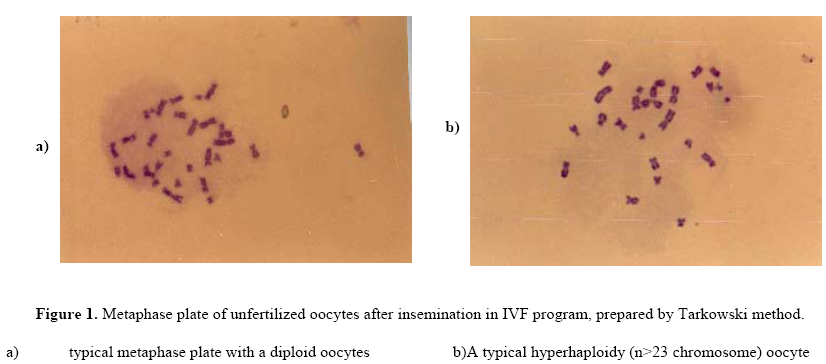
signs of fertilization 18-20 h after insemination . Key words: chromosome abnormality, cytogenetic, unfertilized oocytes, Total Fertilization Failure Introduction Assisted reproductive techniques (ART) have become an established treatment for certain types of human infertility, with high fertilization rate (Edirisinghe et al., 1997). With ARTs used for fertilization of human oocytes in vitro are extremely effective, the overall fertilization rates are now consistently about 60-80% in programs per inseminated egg (Bedford and Kim 1993). The fertilization failure may be occurred in some and/or occasionally all oocytes. In other words, in some women, it is common to find that some and occasionally all pre-ovulatory oocytes in a clutch are non-fertilized. TFF occurs in about 10-15% of patients (Barlow et al1990). Whereas, partial failure in a subset of visually TFF occurs in about 10-15% of patients (Barlow et al. 1990). Whereas, partial failure in a subset of visually normal and mature oocytes from a clutch despite the presence of competent spermatozoa, is more common. There are several reasons for a proportion of oocytes to remain unfertilized after insemination, such as abnormality of sperm DNA, sperm inability to undergo the acrosome reaction, immature oocyte either GV or MI stages and chromosomal abnormality as well (Kalantar et al., 1995; Plachot, 1995; Abruzzo & Hassold, 1995; Wall et al., 1996). Several researches have been attempted to analyze the chromosomal components reporting the incidence of chromosomal aberrations in the human oocyte to range from 11% to 49% (Bongso et al., 1988; Ma et al., 1989; Macas et al., 1990; Angell et al. 1991; Tarin et al., 1991; Kamiguchi et al., 1993; Almmedia & Bolton 1994; Sengoku, 1997). This study was carried out on 115 patients underwent IVF treatment cycles who referred to our center for their infertility problem. Cytogenetic analysis was performed on 513 oocytes, which did not present signs of development 18-20 hr after insemination or re-insemination In Vitro. Materials and Methods Patients who were underwent ART at Yazd Research & Clinical Center for Infertility gave written consent to donate their excess oocytes and unfertilized oocytes for Cytogenetic analysis. The induction procedure was done as previously described (Aflatoonian et al., 2000). Oocytes were aspirated transvaginally with ultrasound guidance 35 h after the hCG administration. Oocytes Table I: The overall results of failed fertilize oocytes from TFF and Pff cycles
* The numbers in parentheses are percantage Table II: Chromosomal Complement of Unfertilized oosytes
were cultured in Ham’s F10 medium supplemented with 10% FBS. Insemination was carried out 4-6 hr following oocyte recovery using 50,000-100,000 motile spermatozoa/ml which were separated from seminal plasma by Percoll preparation. On day one, 18-20 h after insemination (IVF), fertilization was confirmed when two pronuclei (normal IVF) or more pronuclei (poly pronucleus FR) were present. All embryos were graded on basis of 1-4 scales and transfered the best quality were selected and replacement to the uterus. Chromosomal analysis of unfertilized oocytes was carried out within 20-24 hr of collection. Cytogenetic methods Chromosomal preparation was carried out as described by Tarkowski’s techniques (Tarkowski, 1966). Briefly, all oocyte with no sign of pronuclei were collected from TFF PFF. Prior to fixation for chromosomal analysis the cumulus cells were removed from the pre-ovulatory oocyte using 0.1% hyaluronidase (Sigma, Chemical Co., St Louis). The zona pelucida removal was done by mouth pipetting in and out. All oocytes were then exposed to a 1% sodium citrate ashypotonic solution for 10 min. and fixed by a few drops of freshly prepared Carnoy’s solution (3 parts ethanol: 1 part acid acetic glacial, Merck). The slides were dried on a warming plate, and then stained in 10% Gimsa solution (Merck), the metaphase cell examined under an oil immersion objectives lens (Nikon, Co.). The results were analyzed by X2-test, using SPSS for windows. Results In total, 512 unfertilized oocytes from 220 cycles with mean age 30.6+5.1, ranged 23-41 were prepared for further Cytogenetic investigation. Chromosomal analysis was possible on 348 unfertilized oocytes (68%). The number of oocyte per cycle ranged from 1 to 12. All oocytes remained unfertilized from 26 TFF cycles, and in 194 cycles ranged from 1 to 5 as PFF. The Cytogenetic results of unfertilized oocytes are shown in Table I.A total of 232 unfertilized oocytes (66.3%) had a normal haploid karyotype. 6.4% of oocytes had hypo-haploid karyotype, forty-two oocytes (12.2%) were hyperhaploid , +1, to +3 (Figure 1) and 52 were diploid (2n) (Figure 2). Of those only 5 cycles had more than one oocyte with abnormal chromosome, and remaining had only one abnormal oocyte per cycle. The most frequent numerical aberration was observed in chromosome groups, G, D, C, A of the human karyotyped. In cycles with TFF, 33 out of 80 oocytes showed aneuploidy which was significantly higher than cycles with PFF, where aneuploidy was 83 out of 268 oocytes (p<0.01, X2). Discussion The occurrence of unfertilized oocytes considered common in ART treatment cycles. The failed fertilization is caused by abnormal gametes either oocyte or sperm (Bedford et al., 1993). Regarding to MII oocytes and associated with spontaneous miscarriage, may all contribute to the final chromosomal abnormalities in the human abnormal embryos (Plachot, 1995; Abruzzo & Hassold, 1995; Wall et al., 1996; Kamiguchi et al.,1993; Almmedia & Bolton 1994; Sengoku et al., 1997). The present data on cytogenetic analysis of unfertilized oocytes is compared with the average finding of the previous studies presented in Table 3 (32.75, ranged 18–73.8). The 33.3% total abnormality rate of oocytes failed to cleave 44-66 h after insemination, compared favorably with results from several studies (Bongso., 1988; Macas et al., 1990; Pellestor., 1991; Kamiguchi et al., 1993; Lim et al., 1995; Edirisinghe et al., 1997), but not with data from others (Ma et al., 1989; Delhanty & Penketh, 1990; Tarin et al., 1991; Almeida & Bolton, 1994; Nakaoka et al., 1998; Martini., et al., 1997). The difference of the romosomal aberration between different studies may be explained by several factors such as, cause of infertility, age of women, method of culturing of oocytes, stimulation protocol, also method of oocytes preparation for chromosomal analysis as well (Edirisinghe et al., 1992; Lim et al., 1995; Sengoku et al., 1997; Edirisighe et al., 1997; Nakaoka et al., 1998). It is reported that with the method described by Tarkowski an artificial loss of chromosome might occur while using the gradual fixation/air-drying method leads to poor spreading of chromosomes from oocytes that cause difficulty for analyzing in detail (Dyban et al., 1993; Nakaoka et al.,1998). In our study, the success rate of chromosome analysis was 68% which is in more than the gradual fixation/air-drying method used by others (Edrisinghe et al., 1997; Nakaoka et al., 1998). The incidence of chromosome aneuploidy in our study was not significantly different from previously reported as 29.65%, ranged 25%-37.3% (Pellestor et al., 1991; Tarin et al., 1991; Lim et al., 1995; Edrisinghe et al., 1997; Smith et al., 1998) which obtained using both methods As shown in Table2, aneuploidy in unfertilized oocytes was observed in all groups except B and F. the frequency of aneuploidy in group G (n=20, 32.2%) was higher than that in the other groups, which the results consistent with the data reported by Zenzens et al., 1992; Kamiguchi et al., 1993; Nakaoka et al., 1998, while we found only one oocytes with chromosomal anomaly in E group, and non in B and F, groups. We found hypohaploidy in 6.3% of the all analysed oocytes, which is similar to the value of 5.9% reported by Kamiguchi et al., 1993 while hyperhaploid was 12% which was much higher than their value of 4.3% but similar to others report by (Ma et al., 1989; Macas et al., 1990; Angell et al., 1991; Almeida & Bolton., 1994). In the recent study, the overall incidence of dipolidy was high (14.9%) which was similar of finding by Almeida & Bolton., 1994. Our results showed that the incidence of chromosome abnormality in unfertilized oocytes in TFF cycles was significantly higher than oocytes failed to fertilize in PFF. In the case of TFF cycles the semen parameters according to the WHO, 1998 were normal and did not impair the sperm quality. It is interesting to note that in nine cycles in a repeated IVF cycles, arrest of the oocytes was already observed and in one of those cycles sperm with abnormal DNA was found and no chromosomal abnormality in those cycles detected (Kalantar et al., 1998). To our knowledge, the present study represents the analysis of unfertilized oocytes obtained in TFF vs PFF. In conclusion, in a cytogentic study carried out in patents groups with similar stimulation regimens, culture condition, treatment cycle, oocytes preparation, we were able to show that total fertilization failure may be affected by chromosomal aneuploidy. Like all previous studies, there are limitations to the approach used in this study. For instance using FISH technique to analysis the chromosomal abnormality, which would helpful to identify anomalies in detail. Also, we did not performed sperm function tests to find any sperm abnormality especially in TFF cycles to look the possible reasons of sperm and egg dysfunction should be caused of fertilization failure. Since cytogentic analysis of failed fertilized oocytes and sperm function tests are very helpful for direct information on low success rate of fertilization, further studies analyzing on both gametes function in TFF cycles will be needed. Acknowledgment The authors wish to thank IVF team of the centre for providing unfertilized oocytes. References
© Copyright 2003 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm03008f1.jpg] [rm03008t1.jpg] [rm03008t2.jpg] |
| |||||||||

{kind=link}