 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
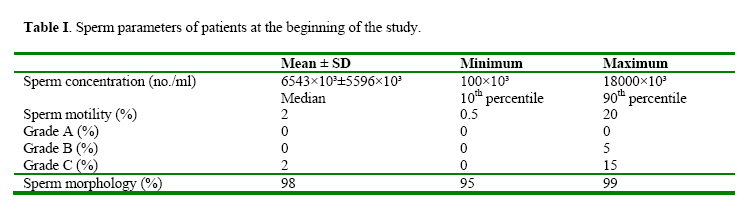
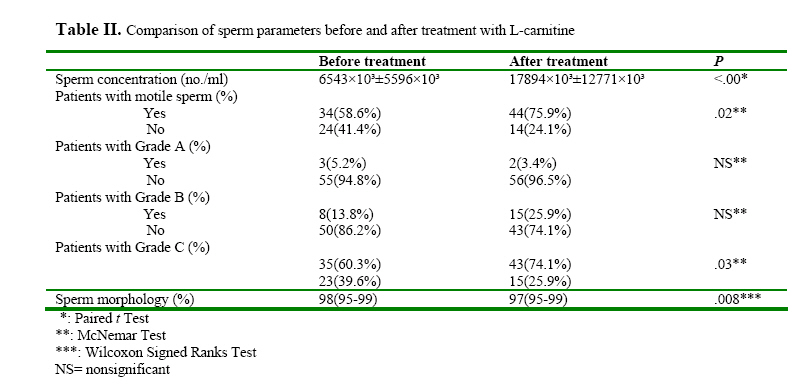
Iranian Journal of Reproductive Medicine, Vol. 2, No. 2, 2004, pp. 65-69 The effect of L-carnitine on sperm parameters in patients candidated for Intracytoplasmic Sperm Injection Afsaneh Khademi, M.D.1, Leili Safdarian, M.D. 1, Ashraf Alleyassin, M.D. 1, Marzieh Agha-Hosseini, M.D. 1, Ehsan Akbari Hamed, 2, Hojatollah Saeidi Saeidabadi, Ph.D.3, and Omid Pooyan, M.D.4 1Assistant Professor, Department of Obstetrics and Gynecology, Tehran University of Medical Sciences. Code Number: rm04013 Background: The etiologic cause in near one third of male factor infertility is unknown. The percentage of men with idiopathic infertility who have been successfully treated by the empirical therapeutic modalities is not high. Keywords: L-carnitine, Intracytoplasmic injection, Semen analysis, Asthenozoospermia Introduction Primary infertility is estimated to affect 15-20% of all couples. In around half of infertile couples, a male-related problem is the partial or sole cause of infertility (Rowe et al., 2000). The etiologic cause in near one third of male factor infertility is unknown (Schlegel and Pavlovich 1997). The treatment of idiopathic infertility was based on experimental pharmacological therapy, although most of this therapeutics may be effective for specific conditions. The percentage of men with idiopathic infertility who have been successfully treated by the empirical therapeutic modalities is not high (Greenberg et al., 1978; Shakkaebaek et al., 1994). So Assisted Reproductive Technology (ART) was introduced for idiopathic oligozoospermia. Quite early in the introduction of ART for idiopathic oligozoospermia and male factor subfertility, some of the leading andrologists in the field, realizing the potential offered, rejected medical treatment and became open supporters of the new techniques. However, some more sober views, advocating a combination of conventional treatments and ART, were also voiced (Comhaire et al., 1995). The introduction of new drugs in recent years has resulted in the new therapies in this field. At the beginning of the 1990s, a pilot multicenter uncontrolled study was begun to test the efficacy of L-carnitine in selected cases of idiopathic male infertility (Costa et al., 1994). Lcarnitine and acetylcarnitine are highly concentrated in the epididymis and play a crucial role in sperm metabolism and nutrition (Marquis and Fritz 1965; Carter et al., 1980). They are related to sperm motility. Indeed, the initiation of sperm motility occurs in parallel with the increase in concentration of free L-carnitine in the epididymal lumen (Juelin and Lewin 1996). A variety of studies support the conclusion that Lcarnitine and/or acetylcarnitine at daily amounts of 2-4gr/day can improve sperm concentration, total sperm counts and sperm motility among men with idiopathic oligo and/or asthenozoospermia, although none of samples in these studies includes severe oligoasthenoteratozoospermia. (Costa et al., 1994; Campaniello et al., 1989; Moncada et al., 1992; Vitali et al., 1995; Vicari and Calogero 2001; Lenzi et al., 2003). No study has been reported to use L-carnitine in ologozoospermic patients candidated for intracytoplasmic injection (ICSI). On the basis of reported experimental and clinical studies we investigated the effectiveness of L-carnitine administration in a group of patients with oligoasthenteratozoospermia of unknown origin who were candidates for Assisted Reproduction Technology. The aims of our study were therefore to assay the effect of L-carnitine on sperm parameters in patients who need intracytoplasmic sperm injection (ICSI) as a method for infertility treatment. Materials and Methods Between October 2003 and March 2004, a total of 385 male infertile patients referred for ICSI were visited in the outpatient clinic of IVF center at Shariati Hospital in Tehran. The study population consisted of 65 men (mean age± SD: 34.4 ± 6.07 and range: 25-53 years) presenting with primary infertility due to idiopathic oligoasthenoteratozoospermia (WHO 1999). The diagnosis was made after medical assessment which included: history; clinical examination especially for varicocelle detection and testicular volume evaluation; semen analysis; semen culture for Mycoplasma Ureoliticum and Chlamydia detection; FSH, LH, testosterone, E2, and prolactin assay, using commercial RIA kits; sonography of genitalia; and MAR test for anti-spermatozoa antibody (SperMAR test, Fertipro NV, Beernem, Belgium). Exclusion criteria were: history of smoking habit, alcohol consumption, and occupational chemical exposure; history of major renal and hepatic disorders and myopathy; treatment with other drugs within the 3 months before enrolment in this study; history or presence of primary testicular disease (cryptorchidism, orchitis, varicocelle) or testicular volume ≤ 12ml; infected semen; elevated (>10 mIU/ml) serum FSH concentrations or other abnormal hormonal assay; abnormal sonography ; and abnormal MAR test (Lenzi et al., 2003; WHO 1999; Balercia et al., 2004). Before and after the ending of the L-carnitine treatment, two semen analyses were performed. The mean was used for analyses. Semen was assessed after abstinence before ejaculation 2 to 7 days according to WHO criteria (WHO 1999). After liquefaction, semen samples were analyzed for sperm concentration (number/ml), percentile of total motile sperm, and percentile of abnormal shaped sperms due to strict criteria of Kruger (Kruger 1986). Motile sperms were divided to four groups based on World Health Organization references: A, B, C, and D (WHO 1999). L-carnitine ( Sigma tau; Italy) was prescribed, 1gram orally every 8 hours for 3 months (Marquis and Fritz 1965). Safety assessment included medical history, physical examination and monitoring of drug-related adverse events by indirect questioning. Of the 65 men enrolled to the study, 5(7%) were lost to follow-up. Two were excluded from study because of incompliance to the drug. The study was approved by Ethics Committee of Tehran University of Medical Sciences. Written informed consent was obtained from all subjects. Statistical analysis was performed by using the SPSS statistical software package (SPSS Inc., Chicago, IL). Paired t-test, McNemar test and Wilcoxon Signed Ranked test were used. The significant level was set at P<.05. Results Our analysis considered 58 patients whom we followed up after treatment with L-carnitine. The mean age was 34.4 ± 5.9 years. The mean duration of infertility was 8.97 ± 5.56 (1 to 21 years). All patients had primary infertility. Table I shows sperm parameters at the beginning of the study. The results were expressed as mean ± SD in variables with normal distribution and median, 10th percentile, and 90th percentile in variables without normal distribution. Table II reports values for semen parameters before and after L-carnitine therapy. After treatment, only in one patient with 5% sperm grade A, did the percentile rise to 10%. In another one, the percentile did not increase and in the third one it decreased to 0%. None of subjects without sperm grade A, showed formation of full motile sperms.Proportion of patients who had motile, and grade C sperms rose significantly after treatment. There were 13 patients (22.3%) in whom complete asthenozoospermia changes to relative asthenozoospermia. Motile sperms in 3 (5%) patients became immotile after treatment. Percentile of abnormal shaped sperms decreases significantly after treatment (Table II). Two of our patients discontinued the treatment because of the bad odour of their sweat. Discussion In 1992, the report on the first successful application of ICSI was published (Palermo et al., 1992). The injection of a spermatozoon which had not been selected in a natural way gave immediate rise to much concern regarding the safety of the technique. The selection of the spermatozoa for ICSI is indeed a matter of debate. This selection is made subjectively through the light microscope by picking out a “good-looking” motile spermatozoon (Tournaye 2003). Finding a way to increase these good-looking motile spermatozoa gives the chance to obtain normal sperms for ICSI. Treatment with carnitines improves sperm forward motility and viability (Costa et al., 1994; Campaniello et al., 1989; Moncada et al., 1992; Vitali et al., 1995; Vicari and Calogero 2001; Lenzi et al., 2003). These drugs are also confirmed to be effective in infertile patients with prostatevesiculo-epididymitis (Vicari and Calogero 2001). However, there is no study about the effect of carnitines on poor semen specimens. It is obvious that motile sperms are alive; however the reverse relationship is not true. Some of live sperms are immotile. Differentiation between dead and alive immotile sperms is possible by sperm viability techniques (WHO 1999). Since the exact proportion of the specimen utilized for sperm viability techniques cannot be used for ICSI, obtaining motile sperms for ICSI is the best policy. Attempts have been made in several laboratories to use ejaculated, immotile (frequently dead) human spermatozoa for ICSI for treatment of infertility due to severe astheno-or necrozoospermia (Dozortsev et al., 1995; Nagy et al., 1995).The results of ICSI with these spermatozoa were variable, ranging from total absence of oocyte activation (Dozortsev et al., 1995) to a fertilization rate comparable to the following injection of motile spermatozoa (Nijis 1996). It is, therefore, unclear whether human spermatozoa, which are dead at the moment of ejaculation or soon afterwards, have any oocyte activating capacity. So it is safer to utilize ICSI for patients with motile sperms. In our study, the percentile of patients who have motile sperms rose from 58.6 % to 75.9%. There were 13 patients (22.3%) in whom complete asthenozoospermia changes to relative atshenozoospermia. Appearing motile sperms will potentially improve the technique of performing the ICSI. We showed that the percentile of normalshaped sperms rises after carnitine therapy. In other studies there was no statistically significant increase in percentile of normal morphology. We estimated the morphology using the strict criteria of Kruger, although in other studies WHO criteria were used. The difference between tools which are used can be the reason. The magnitude of the elevation in normal morphology is not clinically obvious, but it seems that it can be important in obtaining normal-shaped sperms for intracytoplasmic injection. There is a significant increase in the obtaining normal-shaped sperms for intracytoplasmic injection. There is a significant increase in the concentration of sperms in this study, although this finding is not important in ICSI. A limitation of our study was the unavailability of the data about the level of L-carnitine in serum and/or semen. By measuring of L-carnitine level in serum/semen, the effect of the drug is better sensed. Designing a study on selected patients with complete asthenoozoospermia who do not have other abnormalities in semen parameters by determining the amount of the drug we can reveal the real effect of carnitine therapy in this category. References
© Copyright 2004 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm04013t2.jpg] [rm04013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}