 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 4, No.2, Nov 2006, pp. 51-56 Conscious sedation with and without paracervical block for transvaginal ultrasonically guided oocyte collection: A comparison of the pain and sedation levels, and postoperative side effects Simin Atashkhoii1M.D., Sedige Abdollahi2M.D., Aliye Ghasemzad Dejani3M.D., Laya Farzadi3M.D. 1 Department of
Anesthesiology, Tabriz University of Medical Sciences, Tabriz, Iran. Correspondence Author:Dr.Simin Atashkhoii. Department of Anesthesiology, Al-Zahra Hospital, South Artesh Ave, Tabriz, Iran. Received: 25, April, 2005;
Code Number: rm06010 Abstract Background: The quality
of intraoperative analgesia with paracervical block (PCB) during egg collection
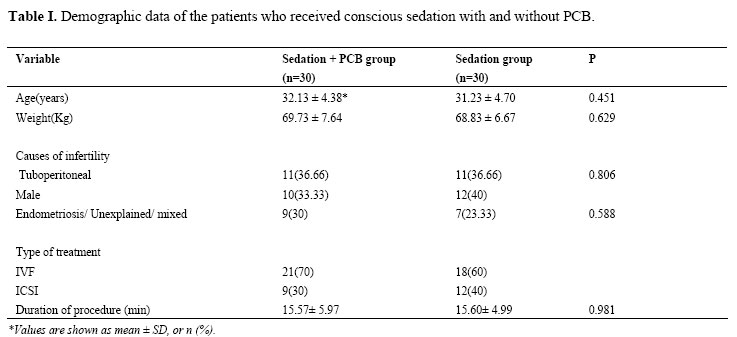
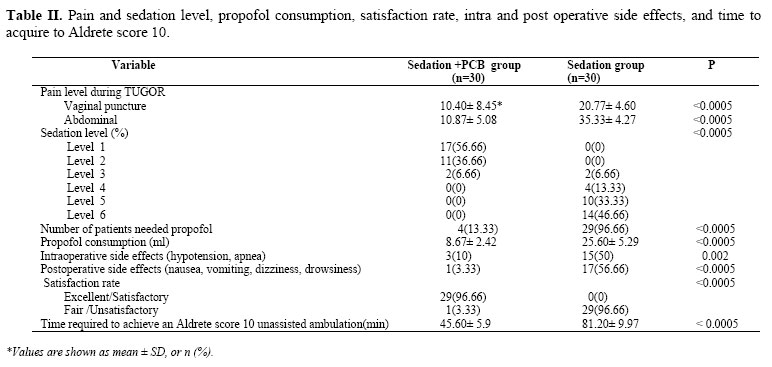
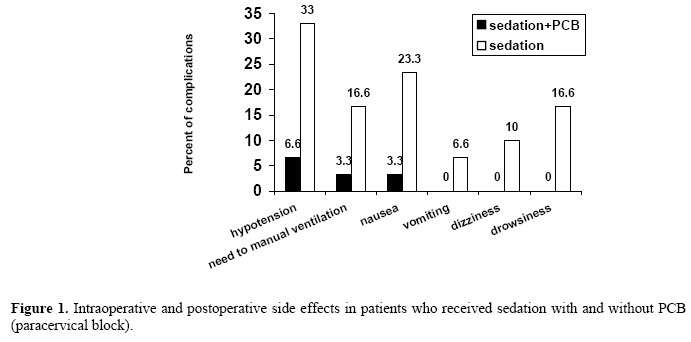
in in-vitro fertilization (IVF) is still unclear. Key words: Transvaginal egg collection, Conscious sedation, Paracervical block, Pain relief Introduction In-vitro fertilization (IVF) with embryo transfer is a well established treatment for various causes of infertility (1,2). It involves ovarian stimulation to induce development of multiple follicles, egg collection and embryo transfer after fertilization (2). Transvaginal follicle aspiration under ultrasonographic guidance has replaced earlier, more invasive recovery procedures (3). Thus, these methods of Oocyte recovery became increasingly simple, less traumatic to patients and simpler for their surgeon (4). Oocyte retrievals are relatively short procedures that are performed on an outpatient basis and are often done outside a standard operation room (4,5). Transvaginal ultrasound-guided Oocyte retrieval (TUGOR) may be the most painful part of procedures performed during in vitro fertilization/embryo transfer (IVF/ET) treatment (6). A variety of anesthetic techniques have been used to make transvaginal Oocyte retrieval safe and efficient. The optimal anesthetic technique should result in few side effects, a short recovery time, and be nontoxic to the Oocyte that are being recovered (4,7). Although general, regional, and local anesthetic methods have all been successfully employed during Oocyte aspiration, conscious sedation has emerged as the most widely used anesthetic technique for this procedure. Studies suggest higher pregnancy and delivery rates if conscious sedation or epidural anesthetic is used instead of general anesthesia (8-10). Howevere conscious sedation alone may be associated with higher postoperative side-effects (nausea, vomiting, dizziness and drowsiness) (6,11). Paracervical block (PCB) has been used in some IVF units, but its role in pain relief during TUGOR, is still not confirmed. Ng Yu et al reported that paracervical block in conjunction with conscious sedation during TUGOR was associated with lower levels of vaginal and abdominal pain as compared to those who received PCB or conscious sedation alone (2,6,12). The aims of this prospective, randomized, double-blind, and placebo-controlled clinical trial were to compare the pain levels during TUGOR and intra operative and postoperative side effects in patients who received conscious sedation with and without PCB. Materials and methods Sixty healthy, American Society of Anesthesiologists (ASA) physical status I patients undergoing ultrasound guided Oocyte retrieval for IVF procedures, were recruited for this study. Written informed consent was obtained from all of the patients prior to participating in the study. All of the patients had 22-39 years of age and 2-17 years of infertility. The inclusion criteria were: the first IVF cycle proceeding to TUGOR, and the presence of follicles in both ovaries. Only patients undergoing the first cycle were chosen because pain scores during egg collection may be influenced by previous experience. Exclusion criteria were: psycologic disorders, general anesthesia requested by patients, fewer than three dominant follicles present, and any history of drug sensivity to local anesthetic. Ovarian stimulation protocol (13) was done by using gonadotropin-releasing hormone agonist [GnRH-a or Suprefact (Buserelin acetate), Hoechst A.G, Germany] down regulation with human menopausal gonadotropin [HMG (Menogon); 75 I.U FSH, 75 I.U LH, Ferring, Germany] or follicle stimulating hormone [FSH (Gonal F) 75 I.U or 5.5 μg, Serono S.A., Switzerland]. At first ultrasound exam was done and oral contraceptive peal (OCP) was started on 5th day of menstruation. GnRH-a (Buserelin acetate) was administered at 21th day of menstruation, then on 3rd day of next menstruation, HMG (Menogon) or FSH (Gonal-F) was started until at least three follicles more than 18 mm was seen on ultrasound exam. Then 5000-10000 unit of human chorionic gonadotropin [(HCG), Holand] was administered 34-36 hours prior to oocyte retrieval. After TUGOR, gametes handling, conventional insemination, and intracytoplasmic sperm injection (ICSI) were performed as has been elsewhere. A maximum of three normally cleaved embryos were placed into the uterine cavity (1,6). All patients arrived in the IVF unit at 08:00 hours; then, after a 30 min period of rest, an intravenous catheter was inserted into the forearm and a standard i.v. infusion of lactate Ringer's solution was started (5 ml/kg/h). Standard monitoring was used throughout the procedure, including blood pressure, heart rate, electrocardiography, pulseoximetry and end-tidalco2. None of the patients received premedication. All patients were then given IV fentanyl (Fentanyl-Janssen, Janssen pharmaceutica N.V ) 1.5 μg/kg, midazolam (Midazolam 5-Exir-Iran) 0.03 mg/kg, and subanesthetic dose of propofol (Propofol-Lipuro 1%, B Braun Melsungen AG) 0.5-1.0 mg/kg, 5-10 minutes before the retrieval. Propofol 2-4 mg/kg/h were infused during TUGOR on patients request if they felt the procedure was too painful (2,5). Both the patient and physicians (anesthesiologist and gynecologist) carrying out the procedure were blind to the local solutions. Patients were randomized into two groups according to a computer-generated list of random numbers: study group; received paracervical block with 10 ml 1.5% lidocaine (Lignodic 2%, IPDIC, Rasht, Iran), and placebo group; received paracervical block with 10 ml normal saline. Ten ml of lidocaine or normal saline were injected through a 21 gauge needle at 1,4 and 8 O'clock positions into vaginal vault 2.5 cm beneath the mucosa in study or placebo groups respectively. The retrieval was performed 5 min later using a 16 gauge double-channel needle under ultrasound guidance with a 5 MHz vaginal probe lifted with a needle allowed aspiration and flushing of follicles. The number of vaginal puncture sites was kept to two, i.e. one for each side. Each follicle was flushed once with culture media and the fluid from aspiration and flushing was examined by an embryologist. TUGOR was timed from the first vaginal puncture to the removal of the needle after aspiration of all follicles>10 mm on both sides. The pain levels were assessed by means of a 100 mm linear visual analogue scale (VAS) (0=none to 100=intolerable pain). The maximum levels of vaginal and abdominal pain during TUGOR were rated by patients during TUGOR. Levels of sedation during the retrieval were accorded to the scale by Ramsay et al (2). Occurrence of any intraoperative and postoperative untoward events including: hemodynamic instability, need for manual ventilation, nausea, vomiting, drowsiness, and dizziness were recorded. The time required achieving an Aldrete score of 10 and unassisted ambulation (14) [time discharge from post anesthesia care unit (PACU)] was recorded. The patients were asked to rate their satisfaction with the retrieval by 4-point scale; excellent, satisfactory, fair, and unsatisfactory (6). After their vital signs were stable, the participants were discharged from the hospital 4 hours after TUGOR. Statistical analysis Statistical analysis was performed using the SPSS software package v13.0. Continuous variables were analyzed using the independent sample t-test, while changes over time were evaluated with repeated measures analysis of variance. Chi-Square test was used for side effects, and satisfaction rate. A value of p≤0.05 was considered significant. Results A total of 60 consecutive women were recruited between April 2005 and February 2006. No significant differences were found between two groups regarding the age and weight, the type and causes of infertility, the type of treatment received, and duration of TUGOR (Table I). The pain and sedation level, propofol consumption, satisfaction rate, intra and post operative side effects, and time to acquire to Aldrete score 10 in both groups are represented in table II. The mean pain levels during vaginal punctures were 10.40± 8.45 mm and 20.77± 4.60 mm and the corresponding mean abdominal pain levels were 10.80± 5.08 mm and 35.33± 4.27 mm. and in the study and placebo groups respectively. These pain levels were significantly higher in the placebo group than the study group (p< 0.0005). Twenty nine (96.66%) of the patients in the placebo group required higher propofol infusion rates during TUGOR, whereas only 4 (13.33%) women in the study group requested propofol infusion (p<0.0005). Propofol consumption in the women in study group was significantly lower than in the placebo women (p< 0.0005). Significantly more women in the study group were at level 1 or 2 of the sedation scale, whereas more women in the placebo group were at level of 5 or 6 of the sedation scale (p< 0.0005). The incidence of intraoperative and postoperative side effects in both groups is presented in figure1. There were significant differences regarding the hemodynamic effects and frequency of manual ventilation during procedure between two groups (p=0.002). There were significant differences between the two groups in the severity of nausea, vomiting, dizziness, and drowsiness after procedure (p<0.0005). The time required achieving an Aldrete score of 10 and unassisted ambulation in the placebo patients were significantly longer than this time in the study group (81.20±9.9 min vs. 45.60±5.09 min respectively; p< 0.0005). The satisfaction scales were comparable in the two groups and around 96.66 % of women in study group rated the excellent/satisfactory versus only 3.33 % of placebo patients (p<0.0005). TUGOR may be the most painful component of IVF treatment. The perception of pain and discomfort during TUGOR is an important issue as most of the couples undergoing IVF are already under great stress and anxiety. Because of the limited success rate, patients may need repeated attempts before pregnancy or live birth is achieved. Furthermore, patients may not remain stationary during TUGOR when they are in pain and this can lead to an increased risk of injuries or damage to the surrounding blood vessels and bowel. It may also explain poor recovery of Oocytes in some patients (1,2). This study investigated the effect of conscious sedation in conjunction with paracervical block on the pain levels during egg collection and the intra and postoperative side effects. In this study, the average score of abdominal pain during TUGOR was 35.33±4.27 mm when only i.v. sedation/analgesia was given. This finding is comparable to the results of other studies using only sedation/analgesia (2). Although conscious sedation is the most widely used method for the pain relief during TUGOR, most findings suggest that the use of only i.v. sedation/analgesia dose not provide adequate pain relief to patients during TUGOR (2-4). The use of propofol in conscious sedation also is limited, because of its tendency to induce substantial apnea, cardiovascular depression, and high expenses. On the other hand, general anesthetics transverse easily into the follicular fluid (FE) minutes after administration to the patient (3,5). Paracervical block has been used in some IVF units to reduce the pain levels during egg collection. However, still its value is not confirmed and there are few studies in the literature addressing this issue (5). Most investigators reported that patients receiving only PCB during egg collection experienced higher pain levels compared with those receiving both PCB and conscious sedation. Therefore it dose not seem advisable to recommend "only PCB" for all patients undergoing TUGOR (6-8). In the present study, there was less pain for vaginal puncture when lidocaine was used in PCB. The upper part of the vagina is remarkably insensitive to ordinary stimuli and the insensivity is explained by the fact that the upper part of the vagina is supplied by autonomic and not somatic nerves (2). This insensivity is also reflected by the finding that transvaginal single follicle aspiration during natural cycle IVF can be performed without analgesia. It is postulated from the results of most studies that lidocaine used in paracervical block anesthetized both the vaginal mucosa and the membrane over the pouch of Douglas or the uterosacral ligaments. This can reduce the levels of abdominal pain during TUGOR (2,6,7). Our results clearly showed that the pain levels during vaginal puncture were 2 times and the abdominal pain levels during the retrieval were 3.5 times higher in the placebo group than study group. One of the explanations for lower pain levels in the PCB group may be the amnesia and analgesia caused by the use of sedatives, and the pouch of Douglas or uterosacral ligaments anesthesia by the paracervical block (2,6,7). Significantly more patients (93.2 %) in the study group were found to be at level 1 or 2 in sedation scale (and 2 cases were at level 3 of sedation scale), whereas 93.2 % of placebo patients were at sedation level ≥4. TUGOR was performed with additional sedation (by propofol infusion) in the patients of placebo group. The need for face mask ventilation was required more frequently in placebo group, but it was transient, and resolving within minuets of reducing the infusion rate of propofol. Incidence of postoperative side effects was more frequently seen in placebo group. The use of propofol infusion in patients of placebo group may also account for some of the side effects noted in this study (6). In total, 96.6% of the patients in the study groups rated the procedure excellent or satisfactory, that it affected by the pain levels during TUGOR while this rate was only 3.33% in placebo group. Those patients in the fair/unsatisfactory grades had significantly higher vaginal and abdominal pain levels during TUGOR and higher postoperative side effects (2,6,7,9-11). The time required achieving an Aldrete score of 10 and unassisted ambulation was more prolonged in the placebo group. The use of lower propofol doses in study group is associated with a lower incidence of postoperative side effects and therefore shorter time of discharge from post ansethesia care unit (PACU) (2, 12,14,15). Conclusion In conclusion, this study showed that the use of i.v sedation/analgesia in conjunction with paracervical block during TUGOR is as affective, safe, and cost-effective as the sedation alone during TUGOR. Acknowledgments The author would like to thank the Research Center of Alzahra Hospital and Vice- Chancellor for research of Tabriz University of Medical Sciences. References
© Copyright 2006 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm06010t2.jpg] [rm06010t1.jpg] [rm06010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}