 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 4, No.2, Nov 2006, pp. 69-72 Comparison of twin pregnancy outcome after assisted reproductive technology with and without embryo reduction Fatemeh Mostajeran1, M.D., Hosna Gharavi2, M.D., Seyed Mehdi Ahmadi3, M.D. 1,2 Department of Obstetric and Gynecology,
Isfahan University of Medical Sciences, Isfahan, Iran. Correspondence Author: Dr. Hosna Gharavi, Department of Obstetric and Gynecology, Al-Zahra Hospital. Isfahan University of Medical Sciences, Hezarjarib Ave., Isfahan, Iran. Received: 14, May, 2006; Code Number: rm06013 Abstract Background: Spontaneous occurrences of
multifetal pregnancies always have been a medical problem. The risks of
perinatal morbidity and mortality and maternal morbidity increase with
enhancement of the number of fetuses. Key words: Assisted reproductive technology, Multifetal pregnancy reduction, IVF, ICSI. Introduction
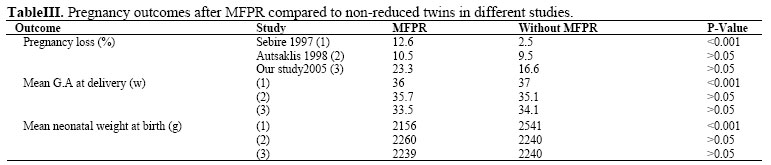
The incidence of multiple gestation (triplet or more) had been increased by epidemic proportions over the past three decades, primarily due to widespread use of ART. Multiple gestations are at higher risk of fetal, neonatal and maternal complications, as well as complete pregnancy loss, when compared to singleton pregnancies(1). Neonatal complications are primarily the result of preterm delivery. Problems related to prematurity include perinatal mortality, low birth weight, respiratory and gastrointestinal complications, and long-term neurological impairment, and finally higher maternal complications (1). Ideally, multifetal pregnancy would be prevented by better control of ovulation induction and embryo transfer (one or two) or follicular aspiration before hCG injection. Secondary prevention, is done by multi fetal pregnancy reduction (MFPR) (1,2). Dumez and Oury were the first to report the technique of embryo reduction in 1986 (3). The researchers estimated that by limiting multiple gestations to twin, mortality of about 58 % of triplets and 70% of quadruplets will decrease (2). Recent studies reported no difference in pregnancy outcome between reduced twins and non reduced twins (4,5), for example in Antsaklis et al study (5), pregnancy loss was 10.5 % in reduced twins compared to 9.5% in non-reduced twins or in Nevo and Avisar study mean gestational age at delivery was 2260 gr. in reduced twins compared to 2240 gr. in non-reduced twins (4), but some studies reported different outcomes, e.g. in Angel's study , reduced twins were hospitalized longer, delivered earlier, had a higher incidence of preterm labor, and a greater percentage of neonatal intensive care than non-reduced twins (6), or in Sebaire et al study, pregnancy loss rate was 12.6% in reduced twins compared to 2.5% in non-reduced twins and mean neonatal rate at birth was 2150 gr. in reduced twins compared to 2541 gr. in non-reduced twins (7) . The aim of this study was to compare the gestational age at delivery, birth weight, and other complications of surviving twins following MFPR to those in a control group of non-reduced twins. Materials and methods This study was an experimental prospective study on infertile couples referred to Isfahan Fertility–Infertility Center (IFIC) from January 2003 to January 2005. They were treated by ART (IVF or ICSI) and then 30 couples who have had twin (control group) and 35 couples with quadruplet or higher order pregnancies (experimental group) were selected. In experimental group MFPR was done after inform constant was given to the couples and they signed a letter of satisfaction. Enough knowledge was given to the patients about complications of multiple gestation and also MFPR, for example complete abortion, infection, premature labor, and limb abnormality. The patients who didn’t accept MFPR or after process had single or triplet gestation or didn’t follow up or had fetal loss within one week of process were excluded from the study. Two patients didn't accept the procedure, in two patients, pregnancy was terminated due to fever after the procedure and in one patient pregnancy continued with three fetuses and MFPR was failed. These patients were excluded from the study, thus the study was started and continued with 30 patients in each group. In all cases of experimental group reduction was performed within 10-13 weeks of gestation by injection of 0.1- 0.4 cc KCl (Produced by Iranian Pastor Institute) (concentration 2 mcg/cc) into the fetal thorax using a 22 gauge translucent needle under transvaginal or transabdominal ultrasound guidance. Asystol was usually seen within one minute of injection of KCl, and total procedural time was typically less than 5 minutes. The needle was left in place until asystol has been confirmed for at least 2 minutes or confirmed with colored doppler and was then withdrawn. Additional fetuses can be reduced with the same needle puncture. An ultrasound was usually performed one hour and again one week after the procedure to again confirm the asystol in the reduced fetus (es) and cardiac activity in the non- reduced fetus (es) once more (8,9). Twenty minutes before procedure, 2 grams ampicillin IV was injected prophylactically and progesterone was administered for ten days as tocholytic. The patients were advised to call the doctor if there were any symptoms of fever, vaginal bleeding, or infectious vaginal discharge. Transvaginal sonography was performed at 12-14 weeks of gestation due to assessment of cervical length and cerclage was done at cervical length below 3cm. Prenatal care for experimental and non experimental group was similar. Statistical analysis Data were compared with Chi-square test or exact Fisher test for pregnancy outcomes and independent t-test or Mann-Whitney for mean gestational age at delivery and mean neonatal weight at birth. Results Pregnancy outcomes of twins in reduced group were not related with starting number of fetuses (p- Value = 0.869). Pregnancy outcomes of two groups are listed in tables I,II. In total 66.7% of neonates in experimental group and 72% of them in non experimental group were viable with normal appearances, while 23.8% of neonates in experimental group and 20% of them in non experimental group were non-viable, but with normal appearances. Only one neonate in non experimental group had Down syndrome and died after 24h of delivery. In experimental group there was not any anomaly in fetuses or neonates. Discussion An increased number of multifetal pregnancies are an inevitable consequence of ovarian stimulation regimens. There is a tendency, nowadays, to transfer a smaller number of embryos (as maximum of two) in order to reduce the incidence of unwanted multifetal pregnancies (5,10). MFPR is a procedure to decrease the number of fetuses in multiple pregnancies to 2 or 3 for decreasing maternal risks and burden of raising many children. Fetuses are selected based on presence of any defect, smaller fetuse (10 days differentiation with other fetuses) or one lowest lying (3). The major risks of fetal reduction are loss of the pregnancy, premature birth and infection of the uterus. Average pregnancy loss rate are 6% for triplets, 11% for quadruplets, and 20% for quintuplets or more. Such losses, however, have to be compared with the back ground loss rate for twin pregnancies known in early stages of gestation, which is nearly 10%. Thus, most experts believe that the procedure related loss rate of fetal reduction ranges between 1% and 2% (10). In Sebire et al study, 127 multifetal pregnancies reduced to twins compared to 354 non-reduced twins as controls. The study showed that in experimental group, the percentage of miscarriage was higher, the mean gestation at delivery in the live births was lower, and the median birth weight deficit was higher than these rates in control group (7). In a retrospective study by Antsaklis et al, 158 patients who underwent embryonic reduction to twin were compared to 135 twin pregnancies conceived either naturally or after assisted reproduction. The miscarriage rate for both fetuses, mean gestational age at delivery, mean neonatal weight at birth and caesarean section rate was similar in cases and controls (5). Similarly, in our study, the miscarriage rate (23.3% vs 16.7%) (p= 0.926), mean gestational age at delivery (33.5 w vs. 34.1 w) (p=0.173) and mean neonatal weight at bright (2239 vs 2240 g) (p-=0.382) was similar in two groups. The results of these three studies are shown in table III. Collaborative data show that pregnancy outcomes improve in most cases when multiple pregnancies are reduced to twins. However, perinatal morbidity and mortality are related not only to the number of remaining fetuses, but also to the starting number, despite successfully performed procedures (10,11). In Antsaklis et al study, one question was that wether the premature delivery was related to the initial number of embryos implanting or the final number of fetuses growing in the uterus? They suggested that, prematurity is a consequence of the number of fetuses in the uterus and is not related to the amount of placental tissue left after the reduction (5). In present study, we considered that pregnancy outcome was not related to the initial numbers of embryos implanted into the uterus. Our limitation in the study was small volume of specimen, because all patients didn't accept MFPR and also some multiple gestations were triplet and were not accepted for MFPR medically. Because the previous studies in this field have been multicentral and it had been carried out on triplet or higher order pregnancies and our study has been unicentral and has taken quadruplet or higher order pregnancies into account, it is not possible to take advantage of former studies for determining sample size. Therefore the minimum number of sample has been used for the experimental study and also the maximum number of patients referring to IFIC was chosen for the research. Ethical consideration must be remembered in order to prevent abuse of this procedure (5). This method is legitimated in Shiite Islamic law (12). Multifetal pregnancy reduction to twins appears to bear no adverse effect on the intrauterine course of the remaining fetuses or their neonatal course and outcome when born after 28 weeks of gestation (4). Conclusion In conclusion, MFPR during early pregnancy is a safe, effective, simple operation for the purpose of reducing perinatal and maternal complications (13). There is no difference in outcome of twin pregnancies with or without MFPR. Acknowledgment We should thank IFIC personnel for collaborating in collecting our data. References
Editorial Comments
There are enough studies to support this that MFJPR reduction will improve the prenatal outcomes such as birth weight and mean pregnancy duration (1-4), while there are some studies which show that MFPR will not improve prenatal outcome comparing with this outcome in non redacted pregnancy (5) or even it cause losing the whole pregnancy. In addition, MFPR will cause emotional & ethical problems for patients and even can increase the risk of maternal infection. Do we have the right to choose which embryo should be destroyed while there is no proof for chromosomal abnormalities in these embryos? There is no answer to this question so far. There fore choosing MFPR should be individualized and its possible problems and complications should be clearly discussed with couples finally it is the patients who make the final decision. Prof. Abbas Aflatoonian Reference
© Copyright 2006 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm06013t1.jpg] [rm06013t3.jpg] [rm06013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}