 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
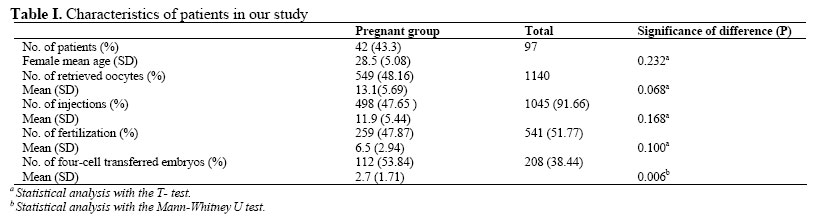
Iranian Journal of Reproductive Medicine, Vol. 5, No.1, Winter 2007, pp. 23-27 Role of embryo morphology in Intracytoplasmic Sperm Injection cycles for prediction of pregnancy Mir Mehrdad Farsi, Ph.D., Ali Jorsaraei, Ph.D., Mahmood Hajiahmadi, Ph.D., Sedigheh Esmaelzadeh, M.D. Babol University of Medical Sciences, Babol, Iran. Correspondence Author: Dr. Mir Mehrdad Farsi, Fatemeh Zahra Fertility and Infertility Centre, Babol, Iran. Received: 19 June 2006; Code Number: rm07005 Abstract Background:Multiple factors have been suggested for prediction of pregnancy in
Intracytoplasmic sperm injection (ICSI) cycles such as the number of injected
oocytes, fertilization rate, embryo morphology and quality of transferred
embryos. Predictive value of these factors is important in ICSI outcome.
Key words: Intracytoplasmic sperm injection, Pregnancy prediction,Zygote morphology, Four-cell transferred embryos Introduction The predictive value of factors involving in intracytoplasmic sperm injection (ICSI) outcome is important in assisted conception treatment. Sperm parameters (1-3), parental age (4), skill of embryologist (5), and morphology of embryos are indicated as important predictors in ICSI outcome (6-11). The selection of embryos at early stages of development are proposed based on pronuclear orientation, polar body placement (6), number and distribution of nucleolar precursor bodies in each pronucleus in zygote stage (8) and number, fragmentation and equal size of blastomers for embryos in day 2 or 3 (10). These data suggest that developmental fate of human embryos is predictable by using these criteria. Tesarik and Greco (1999) found a strong correlation between pronucleus scoring system and implantation rate in a retrospective analysis (8). There is also clear correlation between embryo morphology and implantation rate. Faster cleaving embryos implant at a higher rate. However, embryo morphology and cleavage rate alone do not always result high implantation of potential embryos (10). Furthermore, poor quality embryos may implant and result multiple pregnancy, whereas pregnancy might not occur despite the good quality transfer. The clinical validation of these criteria is still questionable and more studies are needed. This study was focused on the role of embryo morphology in ICSI cycles for prediction of pregnancy. The embryo morphology was recorded in pregnant and not pregnant groups and the differences were analysed statistically. The number of retrieved oocytes, number of injected oocytes, fertilization rate, and quality of embryo transfer, were also evaluated as predictors. Materials and methods Patients In total 97 couples, who were treated by ICSI procedure in Fatemeh Zahra Fertility and Infertility Centre from April 2004 to March 2005, were included in this study. The basal levels of FSH were ≤10 IU/L in all women. To exclude the influence of female age on analysis, women >38 years old were excluded. Oocyte stimulation: The standard long protocol of the pituitary suppression with gonadotropin releasing hormone (GnRH) was used in all patients. After 17 days of oral contraceptive, pre-treatment buserelin subcutaneous injection (Superfact; Hoechst, Frankfurt) was administrated at a daily dose of 0.5 cc until hMG ( Pergonal; Serono,S.p.A., Rome) initiation on the second or third day of next cycle. On the day of initiation of hMG, the dose of buserelin was modified to 0.25 cc until hCG injection. The hMG was administrated at a daily dose of 150-300 IU for 6-7 days. The dose was modified according to the response. Transvaginal ultrasound was performed every 2-3 days to evaluate follicular size, number and quality. When the largest measured follicle(s) reached a maximum mean diameter of 18-19 mm, 10000 IU hCG (Pregnyle, Organon, Darupakhsh)was administrated intramuscularly. Oocytes were retrieved 36-38 hours after hCG injection through a transvaginal route. Sperm preparation: All semen samples were collected by aid of female partner at the clinical andrology laboratory, after an abstinence period of 3-5 days, on the morning of ovum pick-up. In general, routine sperm analysis was performed to measure sperm concentration, as well as percentage of motility and normal morphology. Swim-up washing was completed for all specimens. Oocyte preparation, pre-embryo culture and transfer to uterine cavity Immediately after the collection, oocyte cumulus complexes were put in ham's F10 medium containing 0.1 mg/ml hyaluronidase (Sigma, Aldrich Co., Germany) for maximum of 30 seconds. With hand-drawn glass pipette, oocytes were denuded completely. ICSI was performed in all MΙΙ oocytes with normal appearance. Maximum of four injected oocytes were transferred to a drop of 20-30μl conventional GΙІΙ medium (Vitrolife, Sweden), and it was incubated at least 6 hours in 6% CO2 air under mineral oil (Nidoil, Nidacone, Sweden). Injected oocytes were evaluated under an inverted light microscope (TE 300, Nikon, Japan) at × 200 magnifications for presence of two pronuclei (PN) 16-20 hours later. Zygotes with 1, 3 PN or more and 2PN with significant difference in size and vacuolated zygotes were eliminated. Zygotes were evaluated as good; if two pronuclei were centralized, apposed, and polarized. Zygotes let further culture for 24-30 hours. Embryos were assessed based on number of blastomeres and percentage of cytoplasmic fragments. If there were four-cell embryos with <5% fragmentation, maximum of three embryos were transferred into the uterine cavity. Size of blastomeres and status of nucleus in blastomeres were not considered. Assisted hatching was performed mechanically in all pre-embryos, except for the cases that zona pellucida was hatched easily. Embryos were transferred in maximum of 30-40 μl media (GΙІΙ) by using ultrasound guided catheter (Frydman, CCD, France) and expelled at midpoint of uterine cavity. The quality of embryo transfer (bloody cervix only) was recorded in each case. Luteal supplementation The luteal phase was supplemented with a vaginal administration of 800 mg of natural progesterone (Cyclogest; Hoechst) daily beginning 24 hours after ovum pick-up, and continued until 8 weeks' gestation if pregnancy was occurred. Outcome measures Pregnancy test (β-hCG) was performed 15-16 days after hCG administration. A positive test of pregnancy was followed with an ultrasound to detect gestational sac at 5 weeks after menstrual age. Statistical analysis Statistical analysis including; T-test, Mann-Whitney U test and Fisher's Exact test were performed using SPSS (Version 10.05) software. Logistic regression was used to estimate the significance of variables in the prediction of pregnancy probability. p-value<0.05 was considered to be statistically significant. Results From the total of 97 couples treated by ICSI, 42 cases of pregnancy were detected (Pregnancy rate: 43.3%). In total 1140 Oocyte Cumulus Complex were collected, 91.66% of which were MΙΙ (table I). Overall 259 out of 541 fertilized oocytes were in pregnant group. Pregnancy occurred in 33 (58.9%) patients with at least one good quality zygote (table II). The number of four-cell transferred embryos that resulted in pregnancy was 112 (53.84%). The mean and standard deviation of female age were 28.5 and 5.08 respectively in pregnant group. The mean number of four-cell transferred embryos and the quality of zygotes had significant difference between pregnant and not pregnant groups (p=0.006 and p=0.000 respectively; table I,II). In logistic regression analysis, quality of zygotes (p=0.003) and number of four-cell transferred embryos (p=0.007) were significant predictors (table III). Nagelkerke R2 indicates that probability of analyzed factors for prediction of pregnancy was up to %32. The addition of female age, quality of embryo transfer and progressive motility of sperms as predictors to the L.R. model increased Nagelkerke R2 from 0.32 to 0.34 (data not shown). These factors were not significant predictors. Discussion Although ICSI is a well developed method in assisted conception treatment, the predictive value of the factors that affect its success rate is of great interest. Multiple factors have been suggested for prediction of pregnancy in ICSI cycles (4, 5, 7, 10). We focused on role of embryo morphology in ICSI cycles for prediction of pregnancy. We also analysed the number of retrieved oocytes, number of injected oocytes, fertilization rate, and quality of embryo transfer statistically. Our study differs from others because we used simple criteria in selection of zygotes based on their morphology and we analysed impact of four-cell transferred embryos (≤ % 15 fragmentations) in pregnancy without considering other criteria in embryo morphology 48 hours after injection. We also put variables in a logistic regression model to analyse their predictable value in pregnancy. In our study zygote with big difference in size of pronuclei and large cytoplasmic vacuolization were eliminated out of the culture because strong cytoplasmic vacuolization and unequal pronuclei have been indicated as negative factors on blastocyst development (12). It has been shown that the number of retrieved oocytes and the number of mature oocytes decline significantly with advancing maternal age (4).To exclude the influence of female age on analysis, we evaluated couples with a female partner aged <38 years. The number and distribution of nucleolar precursor bodies (NPB) in pronuclei has been noted by some authors (8, 13). According to Tesarik and Greco (1999) classification of pronucleus morphology, good morphology embryos were significantly more frequent for zygotes with <3 difference in the number of NPB as compared with other patients. The distribution of NPBs was either polarized or non-polarized in this group. Out of 44 embryo transfer with at least one mentioned zygote pattern, 22(50%) clinical pregnancy resulted. Balaban et al (2001) also indicated that pronuclear morphology based on Tesarik and Greco scoring system is significantly related to cleavage rate and quality of blastocyst. In a group that had at least one blastocyst derived from zero PN pattern, clinical pregnancy/embryo transfer was 50% (13). Although these studies emphasize the effect of NPB number and distribution in embryo quality, proposed categories seems to be complex and using these criteria by embryologist encounters some pitfall in routine practice. Pronuclei morphology criteria used in our study was more simple and practical than the mentioned studies (8,13). The present study shows that the probability of pregnancy elevates with the increasing of number of four-cell transferred embryos. This result is similar to Shen et al (2003) report. They analysed many factors in success of ICSI in a single population (5). In addition, transfer of embryos in four-cell stage 48 hours after injection emphasizes the importance of growth rate in pregnancy (14, 15). It is not unusual that high quality zygotes produce low quality embryos while low quality zygotes become top quality embryos, as indicated before (14). Placido et al (2002) indicated that selection of embryos based on morphology of zygote and embryo either independently or together has no predictive value (14). In spite of this study, our analysis shows that the presence of at least one high quality zygote, based on our criteria has predictive value in pregnancy. The probability of factors for prediction of pregnancy in our study was more than Shen et al (2003). Ngelkerke R2 was 0.32 versus 0.16 respectively (5). Conclusion In conclusion, the number of four-cell transferred embryos with ≤ 15% cytoplasmic fragmentation and zygotes with centralized, apposed and polarized pronuclei in women <38 years old have predictive value in pregnancy rate in ICSI cycles. The number of retrieved oocytes, number of injection, fertilization rate, rate of fragmentation (≤ 15%) and quality of embryo transfer (bloody cervix only) were not significant predictors of pregnancy. Acknowledgments We would like to thank our IVF lab technicians (F. Hashemi, F. N. Heidari and M. Fasihian ) and all staff in Fatemeh Zahra Fertility and Infertility centre. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07005t3.jpg] [rm07005t2.jpg] [rm07005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}