 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 5, No.1, Winter 2007, pp. 35-38 Short communication The effect of opium on serum LH, FSH and testosterone concentration in addicted men Seyed Hassan Hejazian, M.Sc., Mohhamad Hossein Dashti, Ph.D., Ali Rafati, Ph.D. Department of physiology, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Correspondence Author: Seyed Hassan Hejazian. Department of physiology, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Received: 4 April 2006; Code Number: rm07007 Abstract Background: Fertility
is considered as a life conservative phenomenon among married couples which can
be obliterated by various conditions affecting both males and females. In the
other hand addiction is a problem which increasingly developed among the
various populations throughout the world, and there are evidences that
addiction may affect the hypothalamous-pituitary-gonadal axis and sexual
functions.The precise pharmacological effects of chronic use of opium on serum
level of gonadotropins and male sex hormones are not studied extensively. This
study was conducted to investigate the changes in these parameters in opium
addicted men.
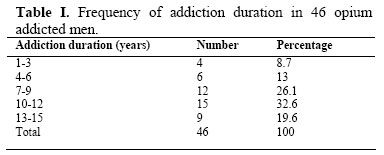
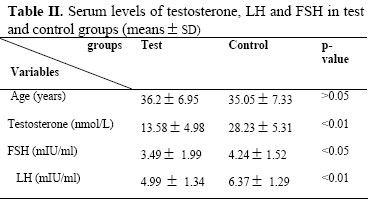
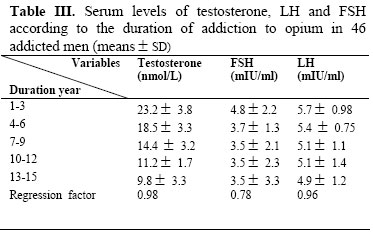
Key words: Opium, Addiction, LH, FSH, Testosterone Introduction Addiction is a problem which is increasingly developed among the various populations throughout the world (1,2). In western societies the major source of drug abuse is heroine (3,4). Therefore most of the research on addiction is focused on the effects of this agent on body systems (1,4) but in Iran opium is the most popular drug among addicted subjects (5-7). Various factors including social, economical and cultural factors are involved in addiction to opium and other morphine containing substances. In the case of gender D,souza et al (2002) tested the overall hypothesis that circulating gonadal steroids are responsible for the gender differences in morphine induced behavior (8). They reported that morphine causes a greater expression of C-fos in the striatum of males than that of females. They concluded that there is a significant sex differences in response to morphine. Also it has been mentioned that there is a relationship between the morphine consumption and steroid hormones. Yan and Hou (2004) found that chronic morphine administration resulted in a marked decrease in the brain concentration of steroids in Rat (9). In the other hand, Peters and Wood (2005) reported that the depressant effect of high dose of steroid hormones on autonomic nervous system is partly mediated by an opioidergic mechanism (10). This evidence suggested that there is a significant interaction between morphine and steroid hormones in those who are exposed to the opioid agents. This may be directly through its action on gonads or via hypothalamic-hypophysiol-gonadal axis. The gonadotropines (LH, FSH) are pulstily released from hypothalamus and acts via hypotalamo-hypophysio-gonadal axis which stimulate gonadal endocrine function and gametogenesis in males. This activity leads to proper spermatogenesis and male sexual responses (11). Suppression of this axis will lead to reduction of sperm count, semen quality, impairment of erection and finally infertility (12). Now a days opioids are increasingly consumed as drug of abuse (1,13,14). Despite many researches on the effects of morphine on different body systems, the effects of long term opium consumption on endocrine system especially on sex hormones are not well studied, therefore we studied the effects of opium addiction on testosterone and gonadotropines in addicted men. Material and methods In this study, 46 opioied addicted 23-48 years old men who had a history of 1-15 years of opium consumption, were randomly selected from Kerman Rehabilitation Center as the test group. At the same time 46 non addicted men with the same including and excluding criteria such as age range, cigarette smoking, social and cultural conditions were selected as the control group. Blood samples were collected from all subjects and serum specimens collected from these samples were frizzed at –20oC. After collection of all specimens, serum levels of free testosterone, LH and FSH were measured by radioimmunoassay (RIA) technique by a LKB gamma counter. Statistical Analysis Data were expressed as mean±SEM for serum levels of testosterone, LH and FSH. Data were statistically analyzed by using student’s t-test and ANOVA using SPSS software. P values less than 0.05 were considered to be significance. Results Considering the duration of addiction to opium indicates that the most frequent duration (32.6%) was 10-12 years among this population (table I). According to age, subjects in control group (35.05±7.33 years) were matched with test group (36.2±6.95 years). Mean values for serum levels of testosterone, LH and FSH from all subjects in control and test groups are shown in Table II. Our data indicate that testosterone, LH and FSH hormones were significantly declined in test group as compared with control group (p<0.01, p<0.01 and p<0.05 respectively). The minimum value for serum testosterone was measured in subjects who had a history of 13-15 years of addiction (9.8±3.3 mmol/L) which was significantly (p<0.01) less than subjects who had the least duration of addiction (23.2±3.8 mmol/L). Similarly, along with the increase in duration of addiction serum level of LH was significantly reduced (4.9 mIU/ml for 13-15 years addicted subjects vs. 5.9 mIU/ml for one year addicted subjects, p<0.01). Also the results obtained from the regression test indicate that there is a positive correlation between duration of addiction and the decline in the serum levels of testosterone and LH in test group but there was no correlation between the reduction in FSH level and the duration of addiction (3.5 mIU/ml for 13-15 years addicted subjects vs. 4.8 mIU/ml for one year addicted subjects (Table III). Discussion Changes in the sexual activity are commonly found in addicted subjects. The effects of drug abuse on sexual functions and sex hormones are one of the major scopes of investigations throughout the world. Since heroin and cocaine consumption is the most popular drug of abuse in western countries the majority of studies have focused on heroin and cocaine addicted subjects (3,4,15). In the case of cocaine many studies have mentioned a significant correlation between cocaine abuse and the reduction in hypothalamo-pituitary gonadal function (16,17). Festa et al (2003) reported that administration of cocaine in Fischer rats affects the endocrine response in both male and female rats and leads to a significant decrease in testosterone level (15). In Contrast, Mendelson (2003) found that despite a significant increase in LH release by intravenous administration of Cocaine there was no change in the testosterone level in men (17). Azizi et al (1973) in a clinical trial study found that there is a decreased in serum levels of testosterone in male heroin and methadone addicts (1). Also Finch et al (2000) suggested that intrathecal opioid therapy in both men and pre menopausal and postmenopausal women led to hypogonadism with low level of serum testosterone or estrogen coupled with low level of gonadotropines (18). Celani et al (1984) in a study on the effect of heroin addiction on the hypothalmo–pituitary gonadal function in men indicated that mean basal values of LH biological activity, and immunoreactive LH in heroein addicts were similar to those obtained in the control group but serum levels of free testosterone were significantly reduced in heroine addicts (4). Conclusion Our findings indicate that in the case of chronic opium consumption there is a significant decrease in serum levels of LH, FSH and testosterone and this reduction was positively co-related with the duration of opium consumption. These findings are in accordance with the Estienne et al (2002) findings (19).They suggest that opioid peptides suppress LH secretion and stimulate GH release in sexually mature Boars. Since Moshtaghi et al (2005) indicated that there is a positive co-relation between the dose of opium and the plasma prolactin level (as an inhibitor of GnRH) in opium dependents (20), thus the suppression of gonadotropine secretion by adenohypophysis may be due to suppression of GnRH release from the hypothalamus. However there are some reports suggesting the direct effects of opium on pituitary gonadotropine releasing cells via kappa (21) and mu (22) opioid receptors. Since there are some report’ suggesting that opium, heroin and methadone could not decreased testosterone level (1,23), the decrease in plasma testosterone level in the present study may be secondary to the suppression of LH and FSH release in opium addicted subjects. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07007t3.jpg] [rm07007t1.jpg] [rm07007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}