 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 5, No.2, Spring 2007, pp. 51-55 Reactive Oxygen Species (ROS) level in seminal plasma of infertile men and healthy donors Mohammad Reza Moein1,2 M.D., Vali Ollah Dehghani1,2 M.D., Nasim Tabibnejad2 M.D., Serajadin Vahidi1,2 M.D. 1 Department of Urology,
Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Received: 20 November 2006; accepted: 20 April 2007 Code Number: rm07011 Abstract Background:
Reactive Oxygen Species (ROS) are a group of free radicals that in excessive
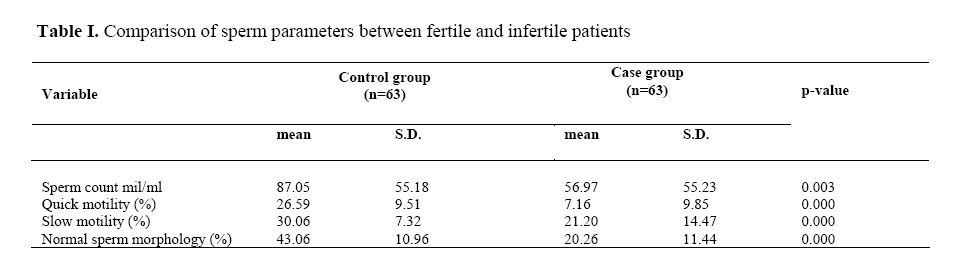
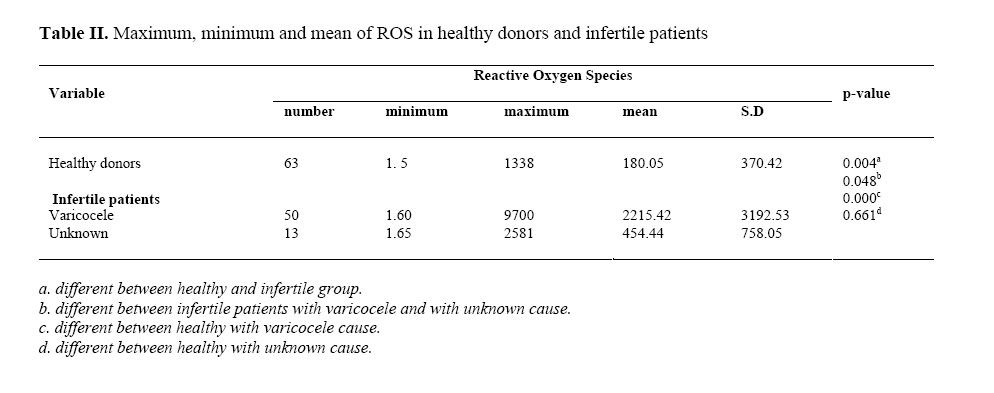
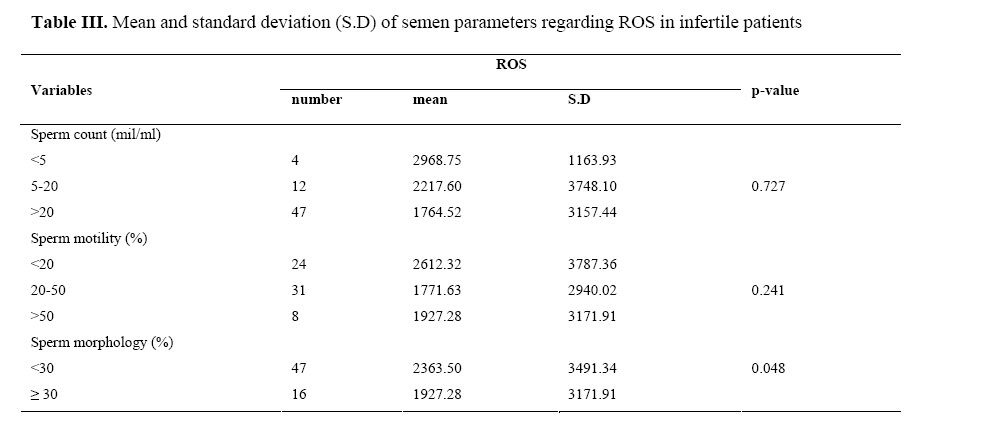
amounts have negative influence on sperm quality and function. Key words: Male infertility, Reactive Oxygen Species (ROS), Varicocele, Smoking. Introduction Reactive Oxygen Species (ROS) are a group of free radicals that are produced by spermatozoa, in male reproductive tract (1). Under physiological conditions, spermatozoa produce small amounts of ROS (2). In minimal amounts, ROS are needed for regulation of sperm function, sperm capacitation and Acrosome reaction; however at high concentration they are toxic to normal cells (3,4). Spermatozoal membrane is rich of polyunsaturated fatty acids and so is susceptible to lipid peroxidation when exposed to high amounts of ROS (1). Gomez et al (1998), demonstrated that the amounts of ROS produced by spermatozoa were negatively correlated with the quality of sperm in the original semen (2). High ROS levels can also affect sperm fertility potential by DNA damage and apoptosis (5). It was shown that the levels of antioxidants in seminal plasma of fertile men are significantly lower than its levels in infertile controls (6). In addition, it is reported that up to 40% of infertile men may have high seminal ROS level (7). Increased production of ROS can also cause a decrease in axonemal protein phosphorilation and reduce sperm motility (8). High levels of ROS have also been correlated with poor semen morphology (9). In this study, we investigated ROS levels in seminal plasma of infertile men and compared it with normal volunteers. We also evaluated the influence of ROS on sperm parameters. Materials and methods Clinical investigations The Institutional Review Board at Yazd Shahid Sadoughi University of Medical Science approved this study. We selected 95 infertile men who were referred to our infertility clinic. Patients who had no child after a period of unprotected intercourse for more than one year and had an abnormal semen analysis were considered infertile. All men were fully examined by a single andrologist. Other investigations like Doppler ultrasonography of scrotum, urine analysis, urine culture and hormone assay including Testosterone and Follicular stimulating hormone (FSH) was done for all, to disclose different possible causes of infertility. Patients were asked about their smoking habits and also the medications that they are probably taking. Finally 32 patients who had azoospermia or history of taking antioxidant medications within the past three months were excluded from the study. We also selected 63 healthy donors with proven fertility who were initiated a successful pregnancy within the last 12 months and had a normal spermogram at the time of study as controls. Semen samples were collected from both groups. All specimens were collected by masturbation at the andrology laboratory, after an abstinence period of 48-72 hours. After liquefaction, routine semen analysis was performed according to WHO to measure sperm concentration, motility and morphology (10). Azoospermic samples or samples with a sperm concentration < 1 x 106 ml were excluded from this study. Samples were also checked for peroxidase positive leukocytes by Endz test, and samples with more than one million WBC/ml were considered positive. Measurement of ROS Levels of ROS were measured by a chemiluminescence assay. Fresh semen specimens were centrifuged at 300×g for 7 minutes and seminal plasma was removed. The pallet was washed with phosphate buffer saline (PBS) and re-suspended in the same media. Ten milliliter of luminal (5-amino-2, 3 dihydro-1, 4 phtalazindione; Sigma chemical Co., USA) used as a probe and was added to the aliquot. A negative control was prepared by adding 10 microliter of PBS. The ROS levels were assessed by measuring chemiluminiscence activity with an Autolamat LB 935 Luminometer (Berthold technologies, Bad-wildbad, Germany) in the integrated mode for 15 minutes. The results were expressed as RLU (Relative light unit) per 20 million spermatozoa. Statistical analysis Data were expressed in mean±SD. Differences between control and patients groups were assessed using Mann-whitney U test. A p-value of ≤0.05 was considered statistically significant. SPSS software version 13 was used for statistical analyses. Results In total, semen specimens from 126 individuals, 63 infertile and 63 healthy donors, were studied. The mean age of normal subjects were 30.78±3.73 years ranging from 21 to 63 years. The mean age of patients in the study group, was 31.43±6.60 years ranging from 23 to 61 years, with no significant difference (p=0.571). Sperm parameters including sperm count, quick and total progressive motility and sperm morphology in both groups are listed in table I. All sperm parameters were significantly lower in infertile patients as compared to fertile men (p=0.000).The mean ROS level in normal men was 180.05 RLU, while in infertile patients this was 1852.04 RLU, which is significantly higher in case group (p=0.000). We divided infertile patients into two groups according to physical examination and the above mentioned workup. Fifty patients had varicocele and in the other 13 patients no apparent cause was found, therefore they labeled as unknown infertility. The mean ROS level in varicocele patients was 2215.42 RLU, and in unknown group were 454.44 RLU, which the difference is statistically significant (p=0.048) (table II). In addition, the mean of the other sperm parameters in varicocele group were lower than unknown group, that is significant for sperm motility (p=0.000) and morphology (p=0.001), but not for sperm count (p=0.1). All samples were checked for WBC by ENDZ test, but none of them showed more than one million WBC and all of the tests were negative. In case group, 19 patients were smoker and 44 were non-smokers. The mean ROS levels in the patients with the history of smoking were 2074.56 RLU, and in nonsmokers were 1336.74 RLU, which was not significantly different (p=0.366). A negative correlation was found between ROS production and sperm concentration and motility, but it was not statistically significant. However normal sperm morphology was significantly decreased with elevated ROS levels (p=0.048) (table III). Discussion Recently the over-production of ROS in the male reproductive tract has become a real concern. Although it has been shown that small amounts of ROS are essential for regulation of normal sperm functions like sperm capacitation, acrosome reaction and oocyte fusion (3), but at high levels they have potential toxic effects on sperm quality and function. Koksal et al (2000) study demonstrated that severe pathologic changes in the testicular tissue are associated with high level of lipid peroxidation and suggested that overproduction of ROS may play a role in the mechanism of testicular degeneration associated with infertility (11). Recent reports have indicated that high levels of ROS can be detected in semen samples of 25-40% of infertile men (12, 13). There are some well known potential sources of ROS production in semen such as: immature sperm and peroxidase positive leukocyte (14). In addition, several clinical entities have been implicated as a cause of oxidative stress in semen such as varicocele (13, 15), cigarette smoking (16) and spinal cord injury (17). Therefore, in this prospective, controlled study, we assessed the level of ROS production in infertile patients and compared it to normal fertile men. We also divided the infertile patients according to the cause of infertility, and measured the ROS level in each group. We also studied the additional effect of cigarette smoking on the level of ROS production in infertile patients. In this study most of our patients in case group have diagnosed to have varicocele and in the other ones, physical examination and laboratory findings showed no specific abnormality, therefore they were considered as idiopathic or unknown infertility. These findings were not unexpected, because most of patients with specific abnormality such as undescendent testis and genetical abnormalities had azoospermia or severe oligospermia, and were excluded from study. In addition, previous studies reported that the incidence of varicocele is about 40% in infertile men (15) which is lower than this percentage in the present study (79.3%), but if we take into consideration the high number of patients, which were excluded from our study, it actually is only slightly higher than the previous reports (52.6%). Our data, showed that infertile men have totally decreased semen quality relative to fertile men, and that all sperm parameter including: sperm count, progressive motility and sperm morphology are deteriorating in infertile patients. In addition, our study showed that the levels of ROS production in semen of infertile patients is significantly higher than this level in control groups (p=0.004). We also assessed the correlation between ROS levels and sperm parameters. Our study revealed an association between high ROS production and reduced sperm concentration and sperm motility in semen, but it was not statistically significant. These findings are contradictory with other reports demonstrating an association between high seminal ROS levels and reduced sperm count (4, 18) and motility (4, 18, 19). In addition, ROS produced by polymorphonuclear leukocytes have been shown to decrease sperm motility (4, 14). The present study also showed a significant negative correlation between sperm morphology and ROS production (p=0.05). This finding is in accordance with Aziz et al (2004) study, in which a significant negative correlation was observed between sperm ROS production and the proportion of sperm with normal morphology(9). As it was cited, the patients were divided according to the cause of infertility into two groups. The results showed that levels of ROS in seminal fluid is significantly higher in patients with varicocele than this level in patients with unknown cause (p=0.048). This is in accordance with previous studies that showed high production of ROS and low antioxidant capacity in infertile men with varicocele (17, 20). As our data showed all sperm parameters, except sperm count, were significantly lower in patients with varicocele than patients with unknown cause of infertility. It seems that this finding may be due to the higher level of ROS in these patients, which by itself has a negative effect on sperm parameters. Although it has shown that a major source of ROS in semen is the polymorphonuclear WBC in seminal plasma of infertile patients (4), but as it cited, none of the semen samples in our study showed abnormal WBC. Therefore, it doesn’t seem that the ROS level in our study group is affected by this parameter. It has been shown that cigarette smoking is one of the causes of increased ROS production in seminal fluid of infertile men (16). In this study we divided infertile patients according to their smoking habit. In total, 19 patients had the history of smoking and the other 44 were not smoker. The results showed that ROS levels are higher in infertile patients who are smokers than infertile men with no history of smoking (2074.56 vs. 1336.74 RLU). Therefore, the difference was not significant (p=0.366), but it shows additional effect of smoking on ROS production in seminal fluid which can be a cause of sperm dysfunction in these patients. Conclusion Our study, showed that level of ROS in seminal fluid of infertile men is significantly higher than fertile donors. It also showed that ROS level in infertile patients with varicocele is higher than patients with unknown cause. High level of ROS has a negative effect on sperm parameters which was significant for sperm morphology. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07012t3.jpg] [rm07012t1.jpg] [rm07012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}