 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 5, No.2, Spring 2007, pp. 73-76 Case report t (3; 22)(q21;q12) in a pregnant woman with two abortions and postnatal death of one offspring Zia Eslami1 M.D., Mohammad Hasan Sheikhha2 Ph.D., Seyed Mehdi Kalantar2 Ph.D., Seyed Mohammad Seyedhasani2 M.D. 1 Department of Pediatric, Yazd Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Received: 8 October 2006; accepted: 3 April 2007 Code Number: rm07017 Abstract Background: Carriers of translocations may have an increased risk of an
unbalanced progeny due to imbalances and delays in meiosis. Key words: t(3;22), Karyotype, Miscarriage, Translocation. Introduction Recurrent spontaneous abortion, defined as three
consecutive abortions, occurs in approximately 1% to 2% of couples. Although
the cause is unknown in up to 50% of cases, about 5% of these couples are found
to be a balanced translocation carrier(1).A translocation carrier may have
an increased risk of unbalanced progeny. As a result, miscarriages frequently
occur. In fact, manycarriers of translocations have a risk of miscarriages
of about 5-10%. The risk will be higher in case of duplication/deletion of
larger regions (2). In addition, chromosome aberrations are found in 27% of
couples with fertility problems (3). In one study, Stephenson and Sierra (2006)
identified 51 carriers of a structural chromosome rearrangement in 1893 couples
(2.7%) with repeated pregnancy loss (RPL) (4).
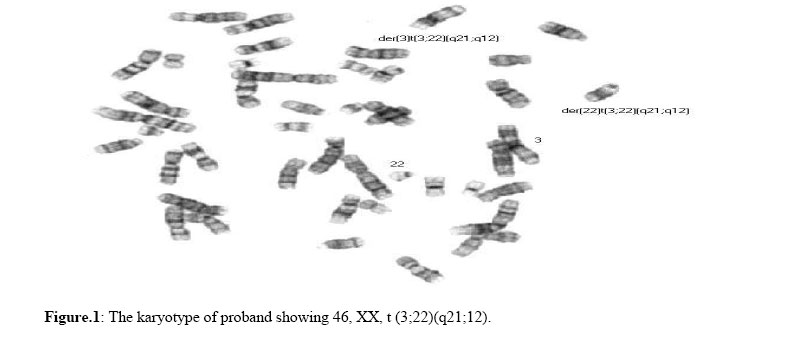
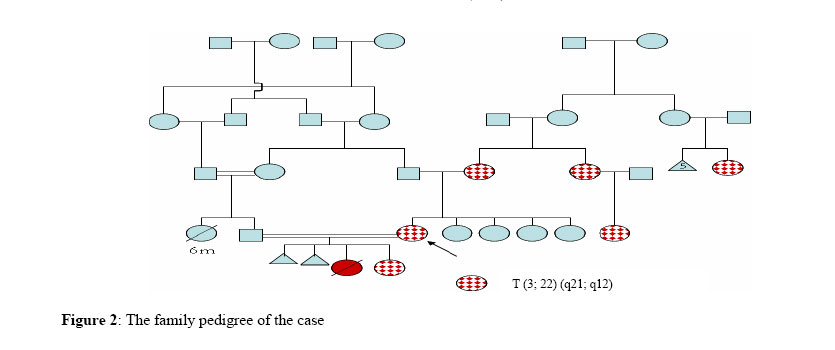
Case Report A pregnant woman was referred for genetic counselling, having had two first trimester abortions (after 6–8 weeks of pregnancy) and one postnatal death of her offspring. This offspring was a girl who had multiple abnormalities including cleft lip and cleft palate, glaucoma and blindness and died when she was 11 days old. Chromosomal analyses had not been done on any of the aborted foetuses or died offspring which had all occurred prior to the cytogenetic analysis of the mother. The infertility of the couple was previously regarded as idiopathic, as none of the common reasons of infertility was found. The husband was a healthy, 30 year old, phenotypically normal male. His semen analysis showed a normal sperm count. His only sister had died for unknown causes when she was 6 months old. His mother and his father were cousin. The proband had four normal and healthy sisters and no brother. Her mother was not related to her father and she had only one sisters. Her mother had a cousin with the history of five repeated pregnancy losses and one normal daughter. There had been no other history of repeated spontaneous abortions in the family. Karoytyping was done for the couple. Chromosomal analyses were done on preparations made from peripheral blood by use of standard methodologies. G banding (5) was done and 20 metaphases spreads were analysed from the couple. The cytogenetic examination was performed on cultured lymphocytes with a resolution of ~550. G banding of chromosomes derived from the woman’s lymphocyte cultures showed a balanced translocation of chromosomes 3 and 22, breakage and reunion have occurred at bands 3q21 and 22q12 and the segments distal to these bands have been exchanged, thus the karyotype was 46,XX,t(3;22)(q21;q12). (Figure 1) Her husband was found to have a normal male karyotype. Examination of peripheral blood lymphocytes obtained from the proband’s mother showed the same translocation in the mother as well. Her father showed a normal karyotype 46, XY. The translocation was found in some other family members as well (Figure 2). The translocation was first interpreted by conventional cytogenetic analysis as a t(3;22)(q21;q12) inherited from the mother. The risk of further miscarriages was high, and the proband was monitored closely during her pregnancy. After nine months of pregnancy, a normal baby girl weighted 3460 gr was delivered by Caesarean section. Three hours after birth, the baby suffered from jaundice and respiratory distress. The hyperbilirubinemia was investigated and it appeared to be a result of ABO incompatibility. It was treated by exchange transfusion and phototherapy. In addition, a systolic murmur (grade II/VI) was heard on chest auscultation and the echocardiography revealed right ventricular cardiomyopathy, which appeared to be secondary to haemolysis and anaemia, as after correction of anaemia the murmur was disappeared and repeated echocardiography became normal. The baby was discharged from the hospital after 15 days in a good condition. The baby’s karyotype showed the same translocation as her mother and grandmother. The family pedigree was prepared according to Rimoin et al. (6). The known karyotypes of the family members were: the proband 46,XX,t(3;22); proband’s husband 46,XY; proband’s mother 46,XX,t(3;22); proband’s father 46,XY; and the proband’s daughter 46,XX,t(3;22), proband's aunt and cousin 46,XX,t(3;22), and cousin of proband’s mother 46,XX,t(3;22) . Other family members either were not cooperated or were not available to participate in cytogenetic examinations (Figure 2). Discussion Carriers of balanced aberrations have an increased risk of an unbalanced progeny due to imbalances and delays in meiosis (2). There are only few publications presenting translocations involving 3q and 22q. While, there are reports of other translocation in RPL. Joseph and Thomas (1987) reported a balanced reciprocal translocation between chromosomes 1 and 7 in both the husband and his mother in a couple who referred for chromosomal analysis having had three first trimester abortions (7). In addition, defects in chromosomes 3 and 22 are reported to be related to other pathological conditions. Partial trisomies of 22q were reported in connection with congenital abnormalities (8-10). Monosomy 22q was also described resulting in serious dysmorphic features and psychomotor delays (11-12). Translocation t(3;22)(q27;q11) was reported to be related with diffuse non-Hodgkin's lymphoma (13). In addition, T-prolymphocytic leukemia, small cell variant, associated with complex cytogenetic findings including t(3;22)(q21;11.2) (14). To our knowledge, no translocation with such breakpoints t(3;22)(q21;q12) has been described previously in the women with RPL. The abnormal karyotype of the proband 46, XX, t (3; 22) (q21; q12) can be regarded as a reason of fertility problems in the investigated couple. The risk of further miscarriages is high due to large segments of duplication/deletion caused by unequal segregation. In the case that the couples seek more pregnancy, close monitoring is necessary. In addition more advanced techniques including prenatal diagnosis (PND) and preimplantation genetic diagnosis (PGD) are advisable. These techniques for people suffering recurrent miscarriages are increasingly being performed worldwide (15). In the cases that PND is performed, if the fetus suffers the same balanced translocation as his/her mother, the pregnancy should be continued, but in the cases of larger duplication/deletion, it must be terminated. Acknowledgements The authors wish to thanks Mr Fazli and Mr Khodaee for all their helps. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07017f1.jpg] [rm07017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}