 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
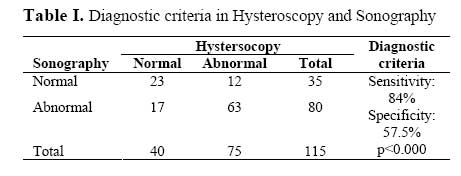
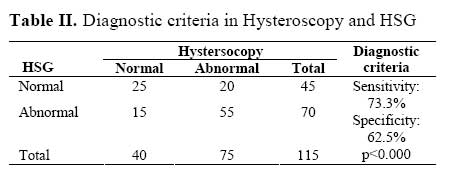
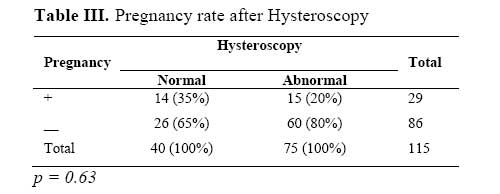
Iranian Journal of Reproductive Medicine Vol.5. No.3., Summer 2007, pp 99-102 Frequency distribution of pregnancy occurrence in infertile women after diagnostic-surgical hysteroscopyEnsieh Shahrokh Tehrani Nejad1 M.D., Tayebeh Naderi2 M.D., Shohreh Irani3 M.D.,Elham Azimi Nekoo1 M.D. 1Department of Obstetric and Gynecology, Tehran University of Medical Sciences and Royan Institute, Tehran, Iran. Correspondence Author: Dr Ensieh Shahrokh Tehrani Nejad, Tehran University of Medical Sciences and Royan Infertility Institute, Tehran, Iran. E-mail: Tehraninejad@royaninstitute.org Received: 11 December 2006; accepted: 23 July 2007 Code Number: rm07022 Abstract Background: Mullerian disorders are present in 5-25% of infertile women. Myoma, polyp and endometrial adhesions are among other involved factors in infertility. Key Words: Infertility, Hysteroscopy, Uterine cavity problem. Introduction Mullerian anomalies are present in 3-5% of the general population and in 5-25% of the women with recurrent abortion, late abortion and preterm labor. Uterine septum, the most common anomaly that is present in 2-3% of the general population is associated with unfavorable productivity prognosisincluding infertility and pregnancy complications (1). Liomyoma, the most common solid pelvic tumor in women, is seen in 20-25% of the women over 35 years and accounts for 10% of the pregnancy complications (1, 2). Endometrial polyps, endometrial adhesions following infections and tuberculosis and iatrogenic adhesions are some other disorders leading to infertility and abortion increase. In 1973, hysteroscope was used for the first time for intrauterine adhesions lysis and after that it has been used for various purposes including myomectomy. Hysteroscopy is indicated in selected infertile cases including those with abnormal hystrography, infertility with unknown cause and recurrent spontaneous abortion. Hysteroscopy can be used as a diagnostic and correction method in patients with anatomical anomalies that have been suspected or proved by hystrosalpingography (HSG) or sonography (2). Since 10-15% of the infertility causes are uterine factors (2), a main part of reproductive problems can be solved by using hysteroscopy. Improvement in productivity after polypectomy has been reported in several studies (3-12). The rate of pregnancy occurrence after hysteromyomectomy has been reported to be equal to that after laparatomy and transabdominal myomectomy, but it is less invasive with more end organ saving (13). Therefore, due to the complications of open surgeries, myomectomy with hysteroscope has been introduced as the selective therapeutic technique (11,14). It was shown that fertility rate was more in hysteroscopy myomectomy cases comparing to infertile patients with normal cavity (5,11). In one study carried on 21 infertile women undergoing hysteroscopy and myomectomy, pregnancy occurred in 11 cases in 2-6 months (15). According to some studies a higher rate of success has been reported in myomas≤ 30 mm comparing to larger myomas (16). According to Varasteh et al (1999) study hysteroscopic resection of a large myoma although may ablate a large surface area of the endometrial cavity, the reproductive benefit appears greater than the risk (11). In other studies in infertile women after septum resection, metroplasty and deliberation of intrauterine adhesions by hysteroscope because of infertility, recurrent abortion, ectopic pregnancy and preterm labor, an increased rate in pregnancy was observed in previously infertile patients, while a reduce rate in spontaneous abortion cases (1,17) The present study was aimed to evaluate frequency distribution of pregnancy occurrence after diagnostic-surgical hysteroscopy in patients referring to Royan Infertility Center (Tehran, Iran) because of reproductive problems. Materials and methodsThis study was designed as a descriptive-analytic study. From all patients referring to Royan Infertility Center (Tehran, Iran) during October 2004 to October 2005, 115 patients were scheduled for diagnostic and therapeutic hysteroscopy. Including criteria were having abnormal finding in the endometrial sonography (polyp, myoma, septation, anatomical abnormalities, adhesion) at cycle day 14, abnormal finding in uterine cavity (myoma, adhision, filling defect, anatomical abnormalities) in HSG, history of recurrent abortions and history of at least 4 unsuccessful IVF or ICSI cycle without any confirmed diagnosis of abnormalities in uterine cavity. After confirming general health, patients were treated with decapeptid for 12 months. Then they underwent diagnostic hysteroscopy under general anesthesia and in the case of observing septum, polyp, submocusal myoma or adhesion hysteroscopic operation was performed. The applied instruments were scissor, ring electrode, forceps and resectoscope. Postoperative sonography and HSG were repeated 2-3 months later and patients were followed for the occurrence of spontaneous pregnancy or IUI, IVF and ICSIinduced pregnancy for 12 months. The criteria for pregnancy occurrence were positive ß-HCG and observing gestational sac in the uterine cavity by sonography. Statistical analysisThe gathered data were analyzed by SPSS and after describing data, variables were compared in pregnant and non- pregnant groups by using Chisquare test. In data analysis p<0.05 was considered as statistically significant. ResultsMean age of participants was 32.65 ± 6.12 years and mean of infertility duration was 8.33 ± 5.25 years. According to the sonography performed before hysteroscopy, 69.6% had abnormal finding and 30.4% were normal. The results of HSG were abnormal in 41.8% and normal in 39% of the subjects. From all, 18.3% had no previous HSG. According to the results of hysteroscopy, 65.2% of the subjects were abnormal and 34.8% were normal. Among 80 cases with abnormal finding in sonography, in 63 cases the abnormality was confirmed by hysteroscopy while 17 cases were reported normal. Among 70 cases with abnormal finding in HSG, 55 cases were abnormal based on hysteroscopy while 15 cases were normal. From all patients who had been reported normal in sonography, 23 cases were normal based on hysteroscopy, while 12 cases had abnormal findings in hysteroscopy and finally among those with normal HSG, 20 cases had problem in hysteroscopy too, while 25 cases were reported normal. Sensitivity and specificity of sonography were respectively 84% and 57.5% and those of HSG were respectively 73.3% and 62.5% (Tables I and II), comparing to hysteroscopy as a gold standard method. Hysteroscopy findings were septum, polyp, myoma, adhesion, endometrial irregularity and bicornuate uterus and all cases with abnormality underwent hysteroscopic surgery. According to the postoperative sonography, 63.5% of the patients were normal and 24% were abnormal. From all patients, 27 cases became pregnant during the first 6 postoperative months and 2 cases during the second 6 postoperative months. Pregnancy occurred without any intervention in 3 cases, after IUI in 4 cases and after IVF or ICSI in 22 cases. From 40 cases with normal hysteroscopy reports, 14 cases (35%) and from 75 patients with problem in hysteroscopy, 15 cases (20%) became pregnant that shows no significant difference between these two groups regarding the pregnancy Tables III, IV, V DiscussionIn uterine disorders affecting productivity, hysteroscopy is the most accurate technique for diagnosis and treatment. By hysteroscopy, direct observation of the uterine cavity regarding its shape, size and location is possible (18). Operative hysteroscopy can be used for removal of uterine myoma and polyps or correction of uterine septum and adhesions. Hysteroscopy in comparison to abdominal metroplasty has improved fertility rate significantly and has lead to less complications. Suspected uterine polyps can be operated successfully by using hysteroscope (2). In infertile women, hysterosalpingography is the first and best imaging technique that can be followed by hysteroscopy in order to confirm the diagnosis. Due to the high prevalence of false negative results in radiographic images of women with uterine abnormalities (2) some suggest hysteroscopic investigation as an obligatory technique. According to Lee et al (1997) HSG is a specific but not sensitive predictor of uterine pathology in patients population. Tubal ostial polyps may occur in a significant proportion of infertile patients and can cause proximal tubal occlusion on HSG (12). The obtained sensitivity and specificity for HSG (73.3% and 62.5% respectively, K= 0.34) and transvaginal sonography (84% and 57.5% respectively, K= 0.42) in the present study, show the importance of hysteroscopy as a diagnostic technique. In several studies improvement in fertility rate following hysteroscopic operations has been observed. In Szymanski et al study (2000) 24% of patients became pregnant after myomectomy, septum resection and deliberation of intrauterine adhesions (17). Sanders (2006) in a literature review about reported case series, demonstrated a reduction in the spontaneous abortion rate from 91% to 17% on average after hysteroscopic metroplasty and 47% pregnancy rate in previous infertile patients and 78% pregnancy rate after hysteroscopy polypectomy compared to 42% in infertile patients with normal endometrial cavities (6). Shokeir et al (2004) suggested that diagnostic hysteroscopy should be used routinely in the workup of infertile women because presence of eumenorrhea persistent functional endometrial polyps, even if small, are likely to impair fertility. Removal of such lesions may improve subsequent reproductive performance (8). In two other studies by Perez-medina et al (2005) and Spiewankiewicz et al (2003) 65% and 80% of the patients undergoing surgery were conceived (7,9). Similarity, in the present study, 35% of the subjects with normal hysteroscopy findings and 20% of the subjects with abnormal finding in hysteroscopy who underwent hysteroscopic surgery became pregnant during one year without any intervention or by assisted reproductive techniques. Although the difference is not significant (p= 0.63), it shows that the infertility factor has not been limited to uterine cavity abnormalities and various factors may have been involved in the studied patients. Therefore longer follow up and were frequent ART cycles are needed. It is certain that abnormalities in uterine cavity should be treated and improvement and revision in techniques of hysteroscopic surgeries can definitely improve the results. These techniques include using more advanced instruments (laser instead of electric electrodes and preventing thermal damage), simultaneous laparoscopy and hysteroscopy in special cases and removal of remained lesions after hysteroscopy (such as interamular myomas) by second operation. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07022t3.jpg] [rm07022t4.jpg] [rm07022t1.jpg] [rm07022t5.jpg] [rm07022t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}