 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 5, No. 4, Autumn, 2007, pp. 165-170 Evaluation of epididymal necrospermia following experimental chronic spinal cord injury in rat Ali Reza Talebi Ph.D., Mohammad Ali Khalili Ph.D., Hossein Nahangi Ph.D., Abulghasem Abbasi M.Sc., Morteza Anvari Ph.D. Research
and Clinical Center for Infertility, and Department of Anatomy, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Received: 4 October 2007; accepted: 27 December 2007 Code Number: rm07033 Abstract Background: Spinal
cord injury (SCI) occurs most often to young men at the peak of their
reproductive health. Only 10% of SCI men can father children without medical
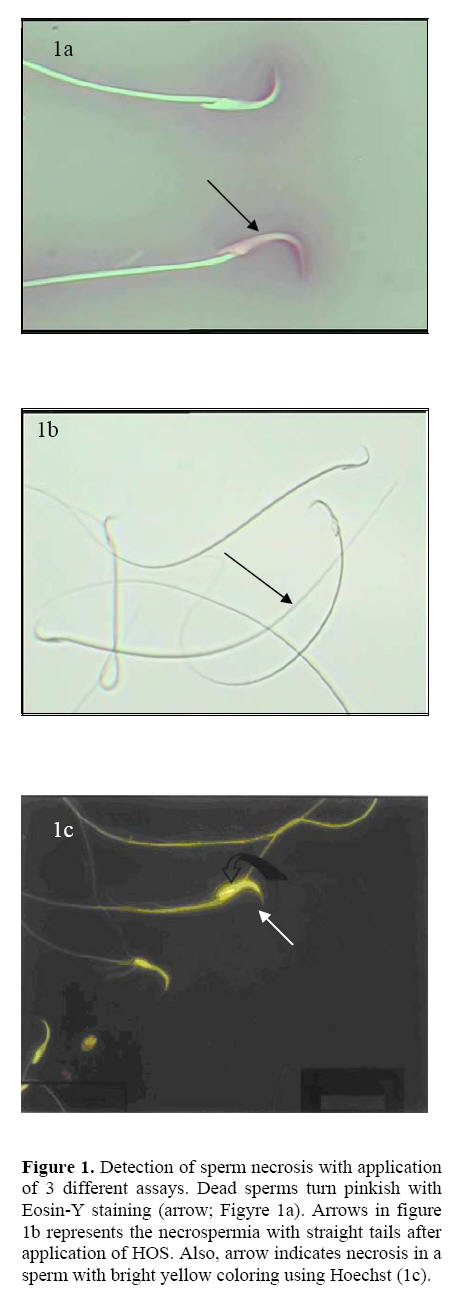
assistance due to potential impairments in ejaculation and sperm quality. Key words: Spinal cord injury, Spermatozoa, Necrospermia, Rat. Introduction Millions of individuals are affected with spinal cord injury (SCI) worldwide. It occurs most often to young men at the peak of their reproductive years (16-45 years) (1). Infertility, due to SCI results from a combination of ejaculatory dysfunction and multiple defects in spermatozoa (1,2). One phenomenon, occasionally associated with SCI is necrsopermia, which is defined as the rates of dead spermatozoa assessed by standard assays (3). In their clinical study on 141 cases of SCI, Brackett et al (3) observed that the ratio of dead to live sperm in SCI men was double than this ratio in the normal men (3). WHO recommended that vitality tests should be applied for all sperm samples with >50% immotility to detect the rates of live from dead sperms (4). Necrospermic samples are unsuccessfull in fertilizing the mature oocytes, even with application of sophisticated assisted reproduction techniques (5). Although, it is a common finding among men with prolonged SCI, necrospermia is very rare in infertile men without SCI, affecting only 0.5% of them (6). Following SCI, which may alter the epididymal autonomic innervation, the sperms accumulate in the cauda epididymis for a long period of time. This in turn causes the aging of spermatozoa, which could disturb normal sperm functioning (7). The damaged spermatozoa are capable of generating high concentration of reactive oxygen species (ROS). Oxidative stress has been associated with a reduction in sperm motility, elevation of DNA fragmentation and denaturation, high rates of necrospermia, and in fertilization process (8). Several assays are currently employed for evaluating the rate of necrospermia in clinical laboratories. The mechanisms of these assays are different from each other, but the rationale is to differentiate live from necrospermic cells within a short period of time. These include: 1- Eosin-Y staining, which selectively red stains necrospermic samples, whereas living cells, regardless of their motility stage, will be unstained (4). This assay reflects sperm membrane integrity, specially the head region that takes up the red stain immediately. 2- HOS (Hyposmotic swelling test) is a non-toxic assay which uses hypo-osmotic solution composed of fructose and sodium citrate. The ability of the live sperm tail to swell and/or coil in the presence of the above solution indicates that the influx of water across the membrane occurs normally (4,9). 3- Hoechst is non-toxic supravital fluorescent dye that binds to adenine and thymedine of double stranded DNA. The necrospermic samples will take up the stain and turn into bright green when viewed under fluorescent microscope (10). In addition, transmission electron microscopy has been used to study the ultrastructure of necrospermia. It was shown that the plasma membrane and acrosome were lost; also, microtubules and mitochondrial membrane were damaged (11, 12). The main objective of the current investigation was to evaluate the effect of experimental SCI on epididymal necrospermia of rats after chronic SCI (one spermatogenesis cycle is about 45 days in rat) with application of three different standard assays. Eosin-Y and HOS assays examine the sperm plasma membrane integrity through different approaches; while, Hoechst assay examines the sperm vitality through nuclear DNA only. To our knowledge, necrospermia following experimental SCI have not been reported by other investigators yet. Materials and methods Animals A total of 45 male Wistar rats (275-300g) were assigned to one of the groups of control, sham, and SCI. Animals were caged in light controlled room, and were fed rat chow with access to water ad libidum. The experimental proposal was approved by our university ethics committee. Control group Rats (n=15) were randomly assigned to non-surgical, non-injected controls. Sham group Rats (n=15) were laminectomized as described by Hirsch et al (7). Briefly, animals were anesthetized with ketamine (80 mg/kg; i.m) and xylazine (10 mg/kg) before a laminectomy was performed at the 10th thoracic vertebrae (T10), leaving the dura mater intact. The exposed vertebral column was stabilized by clamping the T9 and T11 vertebral bodies with surgical forceps. After surgery, the muscles and skin were immediately sutured together in layers. Each rat then received injections of 10 cc sterile saline (s.c.) and 33.3 mg/kg cefazoline antibiotic (s.c.) before being placed on a heating pad during recovery. The rats were housed in individual cages, and their daily activities were monitored by a technician. Spinal cord injury group A total of 15 rats were first laminectomized as described for the aforementioned group. Immediately after laminectomy, a contusion injury was performed with a 10 g brass rod with a tip diameter of 2.5 mm dropped from a height of 5 cm onto the exposed, intact dura overlying the dorsal spinal cord as described by Hirsch et al (7). The impact rod was immediately removed, the wound irrigated with saline, and observed under dissecting microscope for the presence of bruised cord. Then, the muscles and skin were sutured together in layers. Following surgery, each rat was cared as described above. The postoperative care included the sterilizing of wound, and manual expression of bladder twice daily until bladder function returned. Antibiotics (cefazoline) were administered twice a day for one week. Epididymal sperm preparation Animals surviving for 50 days (one cycle of spermatogenesis in rat is approximately 45 days) were anesthetized, as described above. A small piece of cauda epididymis was dissected and placed in 500 µl of PBS. Gentle agitation along with tearing of the tissue was applied to make spermatozoa to swim out into the medium placed in Falcon culture dish (13). Evaluation of necrospermia For evaluation of necrospermia, three different assays were applied under blind condition. Eosin-Y staining The eosin-Y staining (0.5% wt/ vol; Merk Chemical Co., Germany) was done by mixing 10 µl of sperm sample with 10 µl of stain on a microscope slide and covered with coverslip. A total of 100 sperms were counted within 2 min after the addition of the stain (4, 9). Evaluation of live (unstained) and necrospermic (red stained) sperms were done with light microscopy (Olympus, Tokyo, Japan). HOS test The HOS test wasdoneby mixing10 µl of sperm sample and 100 µl of warm hypoosmotic solution. The solution was prepared by dissolving 7.35 g of sodium citrate hydrate and 1.351g fructose in 100ml distilled water , and frozen in 1 ml aliquots for use as required (4, 9). The mixture was incubated (Behdad Co., Iran) for 45 min at 37ºC before it was examined with microscope at x400 magnification (Nikon Co., Japan). 100 spermatozoa were evaluated, and the percentage of live sperms (coiled tail) was calculated accordingly. Hoechst flourescent staining The numbers of live and dead sperms were evaluated according to the methods described by Cross et al (11). The sperm sample was first mixed with PBS (PH 7.2) , and then centrifuged for 5 min at 300 g. Then, 500 µl of Hoechst 33258 ( 100 µg/ml, Sigma Chemical Co., USA ) was added to the pellet for 30 min at 37ºC. The samples were washed free of unbound stain by centrifugations twice at 800g for 5 min. Finally, the supernatant was removed carefully, and the formed pellet was mixed with 500 µl of PBS. The spermatozoa were mounted as smears on glass slides and air dried at room temperature. The slides were evaluated on the same day using fluorescent microscope (Zeiss Axiplae, Germany) with 460 nm filter. The percentage of 100 pale green (live) and bright green (dead) fluorescence sperms per sample was calculated. Statistical analysis Data are presented as mean ± standard deviation. Statistical significance was set at P<0.05. Two-way ANOVA was considered for comparison of the results. Results The results showed that approximately 20% of spermatozoa retrieved from caudal epididymis of control group were necrospermia. This rate was slightly increased in sham-operated rats (Table I). However, fifty days after the weight-drop contusion, the total necrospermia was significantly increased to 46.11% after application of Eosin-Y staining (<0.05). This rate was increased to 45.88% and 42.76% with HOS and Hoechest 33258 assays, respectively. Figure 1 represents the detection of necrospermia with Eosin-Y (arrow); while, HOS assay shows dead sperms with straight tails (arrows). Also, fluorescent staining, Hoechest 33258, detected necrospermia as shown with arrow (Figure 1c). The results also showed that none of the sperm samples were noticed with total necrospermia. All of the assays were successful in detection of necrospermia from all epididymal sperm samples. Table I. The percentage of necrospermia with application of 3 different assays of Eosin-Y, HOS, and Hoechst from epididymis of 3 groups of control, sham operated, and SCI rats.
SCI= spinal cord injury. *control versus SCI Discussion In both rats and human, spermatozoa are capable of fertilizing an oocyte by the time they reach the cauda epididymis. The biochemical changes that sperms undergo during their slow transit to the cauda epididymis will increase the motion characteristics of sperm and their ability to fertilize oocytes (13, 14). Following SCI, however, the epididymal innervations are altered, which would decrease contractility of the duct, cause epididymal dysfunction, delay in sperm transition, and aging of spermatozoa (13). Huang and Li (15) and Linsenmeyer et al (16) induced SCI in rats to study its effect on sperm parameters. They observed a correlation between the severity of cord injury and alteration in sperm motility. All of these obstacles will lead to poor sperm quality and elevation of necrospermia (2, 3). Our previous study showed that sperm progressive motility as well as sperm normal morphology were significantly altered after induction of chronic cord injury in rats (17). In addition, chronic SCI in rats disturbed nuclear maturity and DNA integrity of spermatozoa. All of these alterations could reduce the fertility potential of male gamete in SCI animals. The present study showed that necrospermia is a common phenomenon in samples following chronic SCI in rodents. However, none of the epididymal samples were presented with total necrospermia. Therefore, the rates of necrospermia should be evaluated first with one of the viability assays, so appropriate assisted reproduction technique can be planned in clinical setting. Our results also showed comparable results from 3 different assays that were used for necrospermia evaluation. Both Eosin-Y and HOS tests are simple, inexpensive and quick, with easy application. However, the Hoechst assay is more efficient, with no detectable toxicity (10). Therefore, it is recommended that assays that accurately examine the DNA integrity (e.g. Hoechst 33258) of spermatozoa should be in practice in andrology laboratories. Although, electron microscopy is able to reveal the fine ultrastructure of spermatozoa in cases with necrospermia, but its application in clinical settings is very limited. It may be used for research purposes only (18). On their clinical study on 24 young men with SCI, Padron and associates (1997) found that the levels of ROS were much higher in semen from SCI men than in control subjects. They also observed that the level of ROS was correlated negatively with sperm motion characteristic. They recommended that use of antioxidant therapy may be beneficial in maximizing the sperm quality after traumatic cord injury (19). Also, Brackett et al (3) studied the necrospermia in patients with SCI. Their results showed that the rate of necrospermia was significantly higher (double) in men with SCI than able-bodied individuals. The level of cord injury was not correlated with percentage of dead sperms. They speculated that the higher level of necrospermia indicates a pathological mechanism for sperm cell death (3). One of the main considerations is the management of the SCI patients with poor sperm quality/ high number of necrospermia. In this regards, Wilton et al (6) and Mallidis et al (5) reported that necrospermia will be improved with frequent ejaculation/ 2 ejaculates per day for several days. With daily ejaculation, sperm parameters improved, but did not return to normal value (5, 6). Our experimental findings are in agreement with the aforementioned clinical investigations that have shown epididymal sperm viability was severely damaged after chronic injury to the spinal cord. Therefore, necrospermia is a common phenomenon, which is observed in mammals after chronic SCI. This knowledge can be used to optimize the clinical management of fertility in men with SCI (20). Where possible, semen should be collected and cryopreserved in the first two weeks after SCI. This should enable pregnancies to be produced by intrauterine insemination (IUI) and avoid the need for more expensive interventions, such as intracytopaslmic sperm injection (ICSI) (21). Conclusion This study provides evidence that sperm viability is compromised in animals with chronic SCI. Since, necrospermia is significantly elevated after SCI, it is recommended that following ejaculate collection, precise laboratory technique should be applied to separate live from dead spermatozoa for further infertility treatment. Acknowledgement The authors would like to especially thank the following individuals: Mehrdad Solaimani (B.Sc.), Nasrin Shekariz (B.Sc.) and maryam nayeri(B,Sc) for their superb assistance during the course of this study. This study was supported by grant from the Research Deputy, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07033f1.jpg] |
| |||||||||

{kind=link}