 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 6, No. 1, Winter, 2008, pp. 13-18 Correlation between sperm parameters and sperm DNA fragmentation in fertile and infertile men Nasrin Sheikh1 Ph.D., Iraj Amiri2,3 Ph.D., Marzieh Farimani3 M.D., Rezvan Najafi1 M.Sc., Jafar Hadeie2 B.Sc. 1 Department of Biochemistry and Nutrition, School of Medicine, Hamadan University of Medical Sciences and Health Services, Hamadan, Iran. Received: 15 December 2007; accepted: 19 April 2008 Code Number: rm08003 Abstract Background: It is established that sperm DNA integrity is essential
in fertilization and normal embryo and fetal development. Routine semen
analysis givesan approximate evaluation of the functional
competence of spermatozoa,but does not always reflect the quality
of sperm DNA. Therefore, the evaluation of sperm DNA integrity, in addition to
routine sperm parameters, could add further information on the quality of
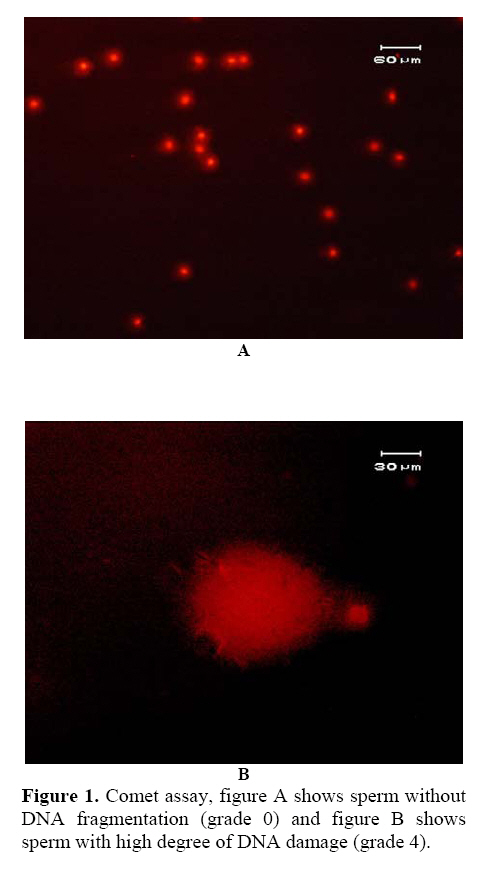
spermatozoa and reproductive potential of males. Key words: Sperm parameters, Male infertility, DNA integrity, Comet assay. Introduction It is established that sperm DNA quality is important in maintaining the reproductive potential of men (1). The fertilizing potential of sperm depends not only on the functional competence of spermatozoa but also on sperm DNA integrity(2-4) Classical semen analysis, which include sperm concentration, motility and morphology givesan approximate evaluation of the functional competence of spermatozoa,but does not always reflect the quality of sperm DNA. Men with normal spermograms may still be infertile; the cause could be related to abnormal sperm DNA (1, 5). Sperm DNA integrity has an important role not only for fertilization but also for normal embryo and fetal development (6). Sperm with compromised DNA integrity, regardless of the degree of DNA damage, appear to have the capacity to fertilize oocytes at the same rate as normal sperm (1). However, the embryos produced by fertilization of an oocyte with DNA damaged sperm can not develop normally. Therefore, the evaluation of sperm DNA integrity, in addition to routine sperm parameters, could add further information on the quality of spermatozoa and improved predictive values could be obtained from validatedsperm DNA fragmentation assays (7). A suitable sperm DNA integrityassay relies not only on its discriminative power to predictfertilization failure but also on its capacity to help cliniciansin the choice of therapeutic procedures (7). A number of studies have investigated the relationship between human sperm DNA damage and semen parameters, such as concentration, morphology, and motility (8-16). In several different study populations, using different assays to measure DNA damage, investigators found associations between some semen parameters and sperm DNA integrity whereas several others did not find associations (17, 18). The most commonly used techniques to assess sperm DNA integrity are the TUNEL,Comet and sperm chromatin structure (SCSA) assays. Comet assay which was first described by Singh et al (19) is a sensitive technique that detects the presence of DNA strand breaks and alkali labile damages in the individual cells. The DNA fragments migrate towards the anode pole at the rate inversely proportional to the size of the fragment during electrophoresis. Before incorporating these methods into the clinical setting, to determine whether sperm DNA integrity measures are predictive of fertility endpoints, several researches are needed to establish a discriminating threshold value for DNA fragmentation in semen samples of fertile and infertile population. Also, more researches are needed to determine the relationship between semen parameters and DNA integrity. The objectives of this study were: 1) to examine the levels of sperm DNA damage by single cell gel electrophoresis (comet assay) in fertile and infertile males and 2) to determine the correlation of sperm DNA damage with semen parameters in fertile and infertile males (in men with proven fertility and men from couplesconsulting for infertility). Materials and methods Study groups The study was done on 45 infertile men selected from couples attending the infertility clinic with a history of infertility of ≥1 years and 75 healthy volunteers of proven fertility (initiated a successful pregnancy) served as the control group. The study protocol was approved by the ethics committee of Hamadan University of Medical Sciences. Written informed consent was obtained from each participant. Standard semen analysis In all cases, after 2-6 days of sexual abstinence, semen samples were collected. All samples for evaluation, were allowed to liquefy for at least 30 minutes at 37°C and then evaluated for sperm concentration, motility, and morphology and leukocyte concentration according to the guidelines of the World Health Organization (WHO, 1999) guidelines (20). Morphology smears were scored using the Kruger's Strict Criteria (21). Sperm parameters were considered normal when sperm concentration was ≥20×106/ml, motility was ≥50% and normal sperm forms were ≥15%. The exclusion criteria were the presence of < 10 × 106 / mL total motile spermatozoa in the original (post–liquefaction) sample, azoospermia and severe oligospermia. No subjects in either group were smokers, on medication, had a history of exposure to chemotherapy or radiation, or a varicocele. Single cell gel electrophoresis (comet) assay In this study, the comet assay was performed using modification of Angelis method (22) in order to detect both single and double stranded breaks. Pre cleaned slide (ROTH, Germany) were dipped in a solution of 1.5 %( w/v) normal melting point agarose (NMPA) in PBS, a coverslip was then placed on top, and allow solidifying at room temperature over night. The next day, coverslip was removed and 100 micro litter suspensions of spermatozoa in 1% (w/v) low melting point agarose (LMPA), at a concentration of 1×104 cell/ mL, was pipetted on the slides and covered with a coverslip. The slides were allowed to solidify at 4°C for 5 min then the coverslip was gently removed, a 1% LMPA was used to form a third layer and slides were allowed to solidify at 4°C for at last 1 h. Then the slides with coverslip were removed and placed in cold lysis buffer (2.5 M NaCL, 100 mM EDTA, 10 mM Tris, 1% Triton X-100, 1% DMSO, and 10 mM Dithiothreitol [DDT] at a PH of 10) for 30 min at 4°C and protected from light. The slides were then incubated at 37°C in 10µg/ml of Proteinase K (Sigma) in lysis buffer for 2.5 h. Following cell lysis, all slides were washed through three changes of distilled water at 5 min intervals to remove salt and detergent from the microgels. The slides were placed in a horizontal electrophoresis tank filled with electrophoresis buffer (10 mM Tris containing 0.08 M boric acid and 0.5 M EDTA pH=8.2) and were kept for 20 min to allow the DNA to unwind. The electrophoresis buffer was adjusted at a level of ~0.25 cm above the slides surface. Electrophoresis was performed for 20 min at 25V adjusted to 300 mA by either raising or lowering the buffer level in the tank. When electrophoresis was completed, the slides were dried and flooded with three changes of neutralization buffer (0.4 mol/l Tris; PH 7.5) each for 5 min. After a neutralization step, the slides were stained with ethidium bromide (20µg/ml dissolved in distilled water) and mounted with a cover slip. Cells were visualized at 200× using a fluorescent microscope (Nikon). Each cell with fragmented DNA had the appearance of a comet with a brightly fluorescent head and a tail to one side formed by the DNA, which contained strand breaks that were drown away during electrophoresis. Measuring comet by visual scoring Analysis of comet cells was performed using the scoring method of Angelis (22). According to this method, the cells divided to 5 classes from 0 (no tail) to 4 (almost all DNA in tail) (Figure 1) according to comet appearance and each cell assigned a value of 0 to 4. At least 100 cells were randomly selected from one slide. Each cell, according to its appearance of a comet, scored between 0-4. The comet value for each slide was calculated between 0 and 400. Because two slides were prepared for each sample, the mean of comet value of two slides was calculated and considered for each case. Statistical analysis Data are reported as mean±SD. The comparisons between two groups were tested by student's t-test using SPSS13. Correlation between two continues outcomes were evaluated using Pearson correlation coefficients. p≤0.05 was considered as statistically significant. Results Semen quality The mean of participants' age, semen analysis parameters and comet value in two groups are summarized in Table I. As shown in the Table I, there are no significant differences in the mean of participants' age in two groups but the mean of sperm concentration and sperm motility of fertile males were significantly higher than that of infertile males (p<0.001). The means of sperm concentration in fertile males was significantly higher than infertile males (63.8±16.7 million vs. 39.7±26.30 million). Total sperm motility of fertile males also was significantly higher compared to infertile (53±5% vs. 29.8±13.7%). Normal sperm morphology of fertile males was also significantly higher compared to infertile (25±6% vs. 13.48±5.6%). The mean of comet value in the sperms of infertile males was significantly higher than that of fertile males (12.9±7.59 vs. 48.77±24.42, p< 0.001) (Table I). Table I.Characteristic of the study population, semen analysis parameters and Comet Value. There were no significant differences in the mean age of participants and morphology of sperms in two groups but the means sperm concentration, motility, Leukocyte concentration and Comet value in fertile males are significantly higher than infertile males (p<0.001).
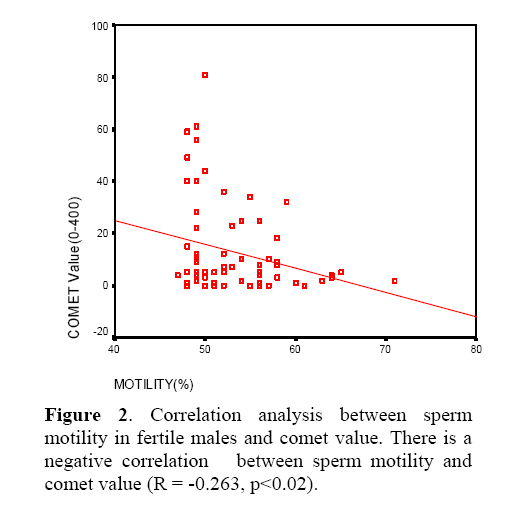
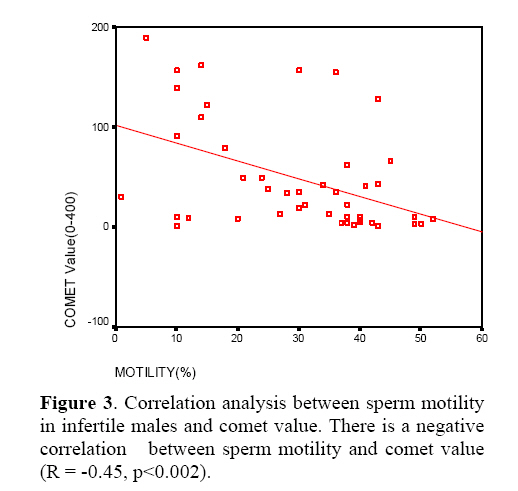
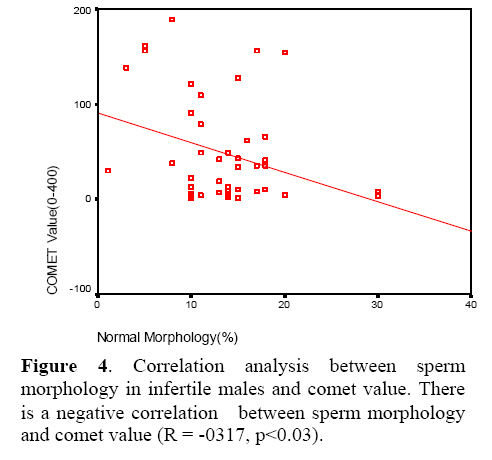
In fertile group there was not any correlation between sperm concentration and morphology with sperm DNA damage (Comet value), but a significant negative correlation was observed between sperm motility and DNA damage (Comet value) in this group (p<0.02, R= -0.263) (Figure 2). In infertile group, a significant negative correlation was observed between DNA damage and sperm motility (p<0.002, R= -0.45) (Figure 3). Also a significant negative correlation was observed between DNA damage and morphology (p<0.03, R= -0.317) (Figure 4). In addition, there was no significant correlation between sperm concentration and sperm DNA damage (Comet value) in infertile group. Discussion This study indicate that sperm DNA damages in infertile males is significantly higher than fertile males and sperms with abnormal morphology and low levels of motility has more abnormal DNA damages than motile and normal sperms. Our results have provided evidence of an important relationship between some of semen parameters and sperm DNA damage. Sperm DNA damage as assessed by Comet assay demonstrated a very clear negative relationship with sperm motility and morphology. Normozoospermics had a lower percentage of sperm with DNA damage compared with infertile group.Our finding of negative relationship between DNA damage and semen quality is supported by data from other laboratories. For example, Irvine et al. (16) evaluated the association between semen parameters and DNA integrity among a group of infertile patients and a group of normozoospermic donors. They showed that semen parameters, especially sperm concentration, were inversely correlated with the comet assay parameters. Sun and colleagues (3) have demonstrated a significant negative correlation between semen parameters and DNA damage in sperm. However, this relationship was not found by Hughes et al. (17) who examined DNA fragmentation rates in the spermatozoa of normozoospermic fertile donors and asthenozoospermic infertile patients with modified single-cell gel electrophoresis assay, possibly because of differences in composition of their study group. Although the extent of DNA damage is closely related to spermfunction and male infertility, the origin of such damage is still largely controversial. It is believed that despite of improper packaging and ligation duringsperm maturation and germ cell apoptosis, oxidative stressis an important factor in sperm DNA damage (4). This is important as mature spermatozoa with DNA damage mayexhibit lower functional potential and this may explain the patients’subfertility status. In summary, we have demonstrated that there was a negative correlation between sperm motility and morphology in infertile males and sperm DNA damage. Also there was negative correlation between sperm motility and DNA damage in infertile males. According to these results we can conclude that testing sperm DNA damage is helpful in selection of spermatozoa with the least amount of damage for use in assisted conception. In turn, this may alleviate the financial social and emotional problems associated with failed ART attempts. References
© Copyright 2008 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm08003f3.jpg] [rm08003f2.jpg] [rm08003f4.jpg] [rm08003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}