 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 6, No. 2, Spring, 2008, pp. 105-107 Case report Spontaneous ovarian hyperstimulation syndrome in a patient presenting with missed abortion Bibi Shahnaz Aali1 M.D., Shahin Narooi2 M.D. 1Department of Obstetrics and Gynecology, Physiology Research Center, Kerman University of Medical Sciences, Kerman, Iran. Received: 21 January 2008; accepted: 20 May 2008 Code Number: rm08018 Abstract Background: Spontaneous
ovarian hyperstimulation syndrome rarely occurs during pregnancy and is usually
associated with high levels of human chorionic gonadotropin, in conditions such
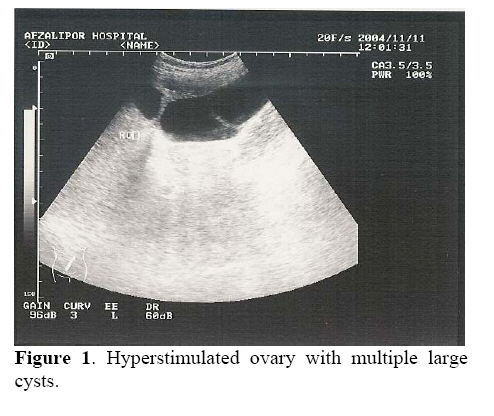
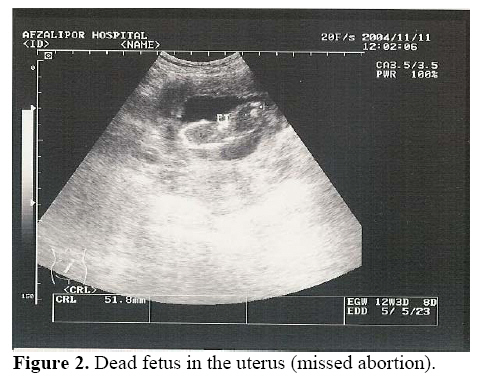
as molar or multifetal pregnancies. Key words: Ovarian hyperstimulation syndrome, Spontaneous pregnancy, Missed abortion. Introduction Ovarian hyperstimulation syndrome (OHSS) is a potentially life-threatening complication of pharmacological ovarian stimulation. The clinical manifestations vary from abdominal distention and discomfort to potentially life-threatening, massive ovarian enlargement and capillary leak with fluid sequestration in the third space. Spontaneous forms of OHSS are very rare and always reported during pregnancy (1). Human chorionic gonadotropin (hCG) is thought to play a crucial role in the development of the syndrome, because severe forms are indeed restricted to cycles with exogenous hCG (to induce ovulation or as luteal phase support) or with endogenous pregnancy-derived hCG (1,2). Several cases of spontaneous OHSS have been observed during multiple pregnancies (3) or hydatidiform mole (4, 5) which are known to be associated with abnormally high values of hCG. Cases of recurrent OHSS in spontaneous singleton pregnancies in individuals and families have been described and linked to germline mutation in the FSH receptor resulting in loss of ligand specificity that permits activation by hCG. The interaction between hCG and the FSH receptor could be an essential prerequisite in the development of spontaneous OHSS and couldexplain why symptoms in spontaneous cases of OHSS appear later than in iatrogenic OHSS in which follicular recruitment and enlargement occur during the ovarian stimulation with exogenous FSH. It is likely that the stimulation of the mutated FSH receptor occurs at a threshold level of hCG which could vary according to the type of mutation (6). Some researchers have presented a sporadic case of spontaneous OHSS and stated that elevated hCG cannot be responsible for spontaneous OHSS as a single factor and factors other than the hCG-FSH-receptor interaction are additionally involved in the pathogenesis of this syndrome (2). Here we present a case of spontaneous ovarian hyperstimulation in a patient with missed abortion and significantly low level of human chorionc gonadotropin hormone. Case report A 33-year-old, G6p3Ab2Lc3, woman attended the obstetrics clinic of Afzalipour Hospital in her 16th week of a spontaneously conceived pregnancy, seeking prenatal care. The uterine fundus was palpated above the umbilicus and at 24 cm from symphisis pubis. However, fetal heat sound was not detected on auscultation. Transabdominal ultrasonography revealed a 14 weeks dead embryo based on crown rump length, without heart activity (missed abortion). Also, both ovaries were enlarged, containing 7-8 cysts being 7-9 cm in diameter (Figure 1, 2). Small amount of free fluid was also visible in pelvis (mild ascitis). The patient's serum ß-human chorionic gonadotropin level was 400 mIU per milliliter (normal values for 12-14 weeks of gestation 50000- 100000 mIU per milliliter). No sign of acne and hair growth was observed. Her past history revealed that she had had 3 uneventful term pregnancies and 2 early abortions at 6-8 weeks. The thyrotropin level (TSH) was normal (0.5 µIU per milliliter) and hematocrit was 36%. The prothrombin time, partial-thromboplastin time, bleeding time, and platelet count were reported as normal. The dead fetus was removed by induction of labor and curettage and the pathology report confirmed missed abortion with no abnormality of the placental tissue. The patient was discharged from the hospital on the third day of curettage. At her follow up visit in the 4th week of curettage she had a ß hCG level of 230 and yet, enlarged multicystic ovaries, albeit smaller than her preoperative state. At week 8 of the operation, when ß human chorionic gonadotropin level was 12 mIu per milliliter, the ovaries almost returned to normal size, although there was still a 2×3 cm cyst visible in right side ovary. Discussion Spontaneous ovarian hyperstimulation is a rare complication of pregnancy usually occurring in conditions associated with high levels of hCG hormone like molar and multifetal pregnancy (3-5). Considering the dead fetus and stimulated ovaries the preliminary impression for the patient was incomplete molar pregnancy, which was ruled out thorough examination of placenta and pathologic report of it. Hypothyroidism was also ruled out due to the normal level of TSH in the patient. It has been stated that high TSH levels associated with severe hypothyroidism may account for the occurrence of the syndrome in the absence of high concentration of hCG (6, 7), because, TSH with three other glycoprotein hormones are derived from a common ancestor and can mimic hCG at high concentration. However, spontaneous cases of OHSS are probably not all related to high levels of hCG or TSH. Smits et al identified a mutation in the FSH receptor gene in a patient presenting with spontaneous OHSS during each of her four pregnancies (8). According to their hypothesis, in spontaneous cases, massive enlargement of multiple follicles would be induced through the hyperstimulation of the mutant follicle-stimulating hormone receptor by endogenous chorionic gonadotropin. Moreover, several mutations of the FSH receptor were recently described in patients presenting with spontaneous OHSS of the first trimester of pregnancy with normal levels of hCG (6). The development of spontaneous OHSS in the presented case presumably is not linked to such a mutant FSH receptor considering the lack of similar symptoms in her previous pregnancies. Whether the hyperstimulation occurred before or after fetal demise is not clear. The strong speculation is that, it has happened before fetal demise but ovarian cysts had not subsided because of their over responsiveness to the decreasing levels of hCG. This case presentation supports the idea that high level of human chorionic gonadotropin hormone is not the exclusive factor responsible for the development of spontaneous hyperstimulation syndrome. Besides, factors other than the hCG-FSH-receptor interaction should be involved in the pathogenesis of this syndrome and further investigations are required to elucidate this enigmatic syndrome. References
© Copyright 2008 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm08018f1.jpg] [rm08018f2.jpg] |
| |||||||||

{kind=link}
{kind=link}