 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 6, No. 3, Spring, Summer, pp. 167-169 Case report Long term management of preterm labor with MgSO4 in myomatous uterus Ataollah Ghahiri1 M.D., Reihane Sabahi2 M.D., Mojdeh Ghasemi3 B.S. 1Associate professor of Obstetrics and Gynecology,
Isfahan University of Medical Sciences. Received: 26 April 2008; accepted: 4 September 2008 Code Number: rm08026 Abstract Background:According to the text book of obstetrics and Gynecology, prematurity is the
first cause of perinatal mortality. Therefore postponing delivery will become
mandatory to prevent complications of prematurity. Parental MgSO4 is one of the
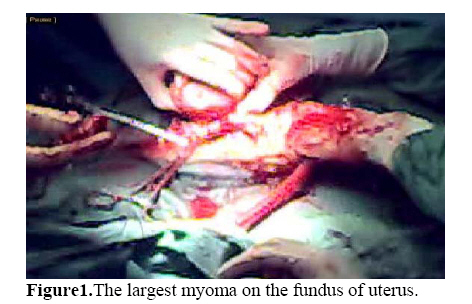
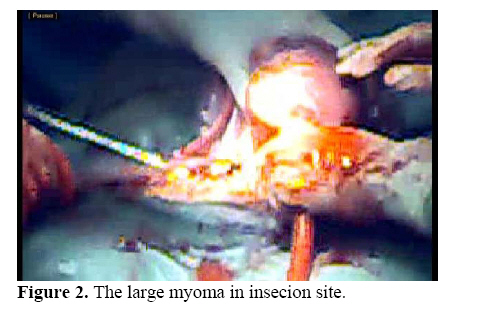
most common and the safest medications for this purpose. Key words: Premature labor, Lyomyoma, MgSO4 . Introduction Prematurity is the second cause of perinatal mortality after congenital anomalies in US and is accounted to be at least 12.5% of the whole deliveries in which 2% are less than 32 weeks of gestation. MgSO4 have been used for reducing uterine contractions, successfully in most hospitals. It is clear that neonatal morbidity and mortality will be decreased as the gestational age progress. Case presentation A 32 years old primigravida patient was referred to Alzahra Hospital with abdominal (uterine) pain, at her 25th weeks of gestation proved by ultrasonography and her LMP. She was found to have multiple uterine intramural myomas and with different sizes, before her pregnancy and also during it (figure 1, 2, 3). These myomas were reported sonographicaly to have different sizes of 2.3, 4, 5, 5.4, 7and 8 cm in length. At 17th week of her gestation, the obstetrician reported a 12.5 cm myoma as the largest on the uterine fundus and a 10.5 cm around the lower segment of the uterus by sonography. There was no clear congenital anomaly of the fetus in this sonography report. At her post history, she had a hyperthyroidism which was stable before getting pregnant and she was not getting any special medication for that. She had also the history of same episodes of uterine contractions from beginning of the second trimester of her gestation that get better with β receptor agonist and bed rest. She was admitted to the hospital at her 25th week of her gestation, complaining painful uterine contractions lasting about 30 seconds with the intervals of 2-3 in each 20 minutes. In vaginal exam, she had partial effacement with a dilatation of 2-3 cm, the amniotic sac was bulged through the cervix, the FHR was normal and the height of uterine fundus was 32 cm. At first the plan of treatment and probable risks of long term treatment by MgSO4 were described to the patient and her satisfaction letter was attached to her file. The patient was hospitalized at labor room with the order of complete bed rest in trendelenburg position. MgSO4 was started intravenously at the dose of 2-3gr/h intermittently which stopped the uterine contraction. The patient's lab tests were mostly normal except for GTT, leading us to start 10 units of NPH insulin daily before her breakfast. During her stay, the follow-up sonography showed a cervical dilatation of about 5 cm. Because of restarting the uterine contractions in spite of 3gr/h of MgSO4 , Nifidipin (Adalat) was added to her regime at the dose of 10mg q8h orally. For the prevention of thromboembolic phenomena during her complete bed rest, low molecular heparin (fragmin) was also started: 5000 IU daily SC. The serum Mg of the patients was checked not to exceed its therapeutic dose. The patient fetal well being was monitored by NST and BPP according to its conditions every day or every other day. At her 52nd day of admission she got tachycardia at a rate of 120-130 b/min with no dyspnea or tachypnea. Her ABG and ECG showed normal values as well as echocardiography. No thrombosis was reported at color Doppler of her lower exterimities, therefore Nifidipin was discontinued and Enoxaparine was started at a dose of 40 mg twice daily according to the medical consulting. Finally at the day of 58 of her hospitalization because of a decrease in fetal movements and Breech presentation, cesarean section by Mis Gavladach technique was performed at the gestational age of 34 weeks. The baby was a girl with APGAR score of 5/10 and 7/10 at 1 and 5 minutes respectively. The uterus had multiple intramural myoma with different sizes, the largest measuring 10 x 5 cm at the fundus and 8 x 6 cm at the lower segment. The uterine incision was down transversely at low segment under the lower myoma and was repaired successfully by No1 vicryle. The baby’s weight was 2300 gr. The patient tolerated the operation well with no uterine atonia and the Estimated Blood Loss was about 600 mls. The day after operation, she found dyspnea besides her tachycardia and because of the hypoxia seen at the ABG, Enoxaparine was exceeded to 60 mg BID and warfarin started. The perfusion scan of the patient's lungs reported large segment defect highly suggestive of PE. Ten days later the patient was discharged from the hospital in good condition. The baby showed mild RDS and was discharged after the management as well. Discussion Prematurity is the second cause of perinatal mortality after congenital anomalies in US and is accounted to be at least 12.5% of the whole deliveries in which 2% are less than 32 weeks of gestation. MgSO4 have been used for reducing uterine contractions, successfully in most hospitals. It is clear that neonatal morbidity and mortality will be decreased as the gestational age progress. Wedig et al reported an 8 weeks (22-30wk) therapy with intravenous MgSO4 for prevention of premature delivery in a triplet pregnancy (1). In Nayashi and Matsuda et al study they continued MgSO4 for 5 weeks for a patient with a twin pregnancy in combination with Ritodrin (2). In another study by Levar et al, writers postponed the delivery of a triplet pregnancy for 65 days (3). In literature review of long time therapy of MgSO4 , we can see symptomatic hypocalemia which is dose dependent (4) and maternal osteoporosis, after 65 days of MgSO4 infusion in combination with heparin (3). With prolonged bed rest for the management of premature labor, thromboembolic phenomenon increases significantly (5). Carr et al reported a rate of 15.6% of thromboembolic phenomenon in 1000 pregnant patients following complete bed rest from 7 to 49 days (6), comparing to its rate of 0.5-3 per 1000 during normal pregnancy (7) . The signs and symptoms of PE are completely different and non specific including dyspnea (73%), pleuretic pain (66%), Tachypnea (70%) and Tacycardia (30%). The non invasive diagnostic method is spiral CT (lung) and also perfusion scan, although their accuracy for diagnosis is not so enough (15-86%). Pregnancy with uterine leiomyomas can increase the C/S rate, breech presentation, premature labor, placenta previa, and post partum hemorrhage, is major complication especially if the size of myoma is more than 10 cm (8). It seems that the mentioned complications of pregnancy will be increased mostly by submucosal and retroplacental myomas. IUGR and premature delivery have been also reported with uterine myomas during pregnancy (9). Myomectomy during pregnancy has been completely limited to degenerated, pendanculated subserosal myomas and those sever sign and symptoms do not respond to usual managements (9). Myomectomy during C/S is contraindicated and is associated with massive hemorrhage. Boser et al reported that the rate of myoma with pregnancy is increased in nulliparous and the age of above 30. They also proved in their study that the most growth rate of the myoma is in the second trimester of pregnancy (10). References
© Copyright 2008 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm08026f3.jpg] [rm08026f2.jpg] [rm08026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}