 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 7, No. 1, Winter, 2009, pp. 1-5 The outcome of in vitro fertilization / intracytoplasmic sperm injection in endometriosis–associated and tubal factor infertility Ensieh Shahrokh Tehrani Nejad1,2,3M.D., Batool Hosein Rashidi2,3 M.D., Atefeh Larti3 M.D., Zahra Ezabadi1 M.Sc., NadiaJahangiri1 M.Sc., Elham Azimi Nekoo3 M.D. 1Department of Endocrinology and
Female Infertility, Reproductive Medicine Research Centre, Royan Institute,
ACECR, Tehran, Iran. Received: 11 September 2008; accepted: 22 February 2009 Code Number: rm09001 Abstract Background: Endometriosis is one of the most challenging diseases that constitute 20% - 40%
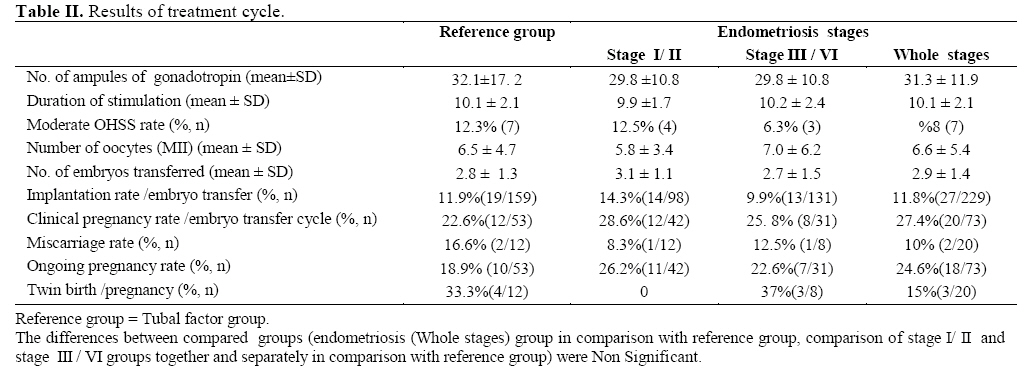
of women searching for their infertility diagnosis. Key words: Endometriosis, IVF / ICSI outcome, Tubal factor, Infertility. Introduction Endometriosis is a disease of reproductive-aged women that constitute 20% - 40% of women looking for their infertility diagnosis (1, 2). There are several theories in association with endometriosis, but the theory of retrograde remains dominant (3). The mechanism by which endometriosis cause infertility has not been completely determined (2), but the factors which have been suggested for infertility in women with endometriosis, include pelvic adhesions, ovulatory dysfunction, altered folliculogenesis, defective implantation and luteal phase defect (1, 4, 5). The effect of endometriosis on assisted reproductive outcomes are the issues continuously debated (2, 6, 7). In some studies a reduced response to gonadotropins, and a lower number of oocytes, has been described (5, 8). Several authors reported a significant lower implantation among patients with endometriosis compared with tubal- factor infertility (9, 10). In contrast, in another study, no differences in the number of oocytes, and implantation rates were observed (11). Matalliotakis et al(2007) found that patients with endometriosis had lower peak E2 levels, higher cancellation rate and lower oocyte reserve than tubal factor groups, but there were no differences in fertilization, implantation, pregnancy, miscarriage and delivery rates between two groups (7). Some early researchers indicated that pregnancy rates after IVF were significantly higher in women with minimal to mild endometriosis than in those with severe endometriosis (12, 13). Although IVF was initially used for treatment of tubal factor, patients with endometriosis may have anatomic dysfunction of the fallopian tube and ovary, which may need the use of IVF (7). Considering the presence of controversies in data on the effect of endometriosis on the results of IVF/ICSI treatment, we decided to perform this study. The main objective of this retrospective study was to compare the outcome of IVF/ICSI cycles in women with endometriosis and tubal factor infertility as control and the specific purpose was to explore if the stages of endometriosis influence the results of IVF/ ICSI. Materials and methods Between 2005 and 2006, all the cases of patients with infertility who underwent IVF or ICSI treatment at Royan Institute (Infertility and Reproductive Medicine Research Centre) were assessed and 137 infertile women were identified. The study group consisted of 80 women with endometriosis, while the control population comprised 57 patients with tubal infertility. Endometriosis was scored according to the American Fertility Society classification (1996). Diagnosis of the two groups had previously been confirmed by laparoscopy. Inclusion criteria for the women were age < 37 years, minimum 2 years of infertility, regular menstrual cycle, normal concentrations of prolactin, free thyroxin and thyroid–stimulating hormone (TSH). Patients with polycystic ovaries and women with other known infertility factors besides the endometriosis and tubal factor infertility were excluded. In addition, for the patients, no medical treatment for endometriosis-associated infertility had been performed during at least one year. All semen samples in both groups were normal (according to the World Health Organization criteria). A standard long protocol was used for COH. In summary, Buserelin acetate 500µg/day (Suprefact®, Hoechst, Frankfurt, Germany) was administered subcutaneously on the cycle day 21. After established ovarian suppression (by ultrasound or serum E2 level <50 pg/mL), the dose of GnRh agonist was reduced to 200μg/day, and daily injection of hMG (Menopur; Ferring, the Netherlands) commenced at doses of 225 IU/day and increased until 450 IU/day depending on the patient's age, body mass index and ovarian response. When there were at least two follicles with a diameter more than 18 mm, Human Chorionic Gonadotrophin (10,000 IU IM, Pregnyl®; Darou Pakhsh Pharmaceutical, Tehran, Iran) was administered. Oocyte retrieval by transvaginal guidance was performed 36 hours later. The luteal phase was supported by intramuscular progesterone 100 mg/day (Amp 50 mg; Aburaihan, Tehran, Iran) starting the day before embryo transfer for 2 weeks. In both groups, ICSI was performed for couples who previously had experienced at least one cycle of IVF failure in spite of normal parameters of semen according to WHO standard. The resulting embryo was transferred to the uterus 48-72 hours after oocyte retrieval using ultrasound–guided transvaginal approach. Pregnancy was confirmed by increasing level of concentration of serum βHCG which was assessed 14 days after embryo transfer. The embryos were graded according to their morphology, cleavage stage and fragmentation rate (14). Only the embryos with high quality were transferred. This study was approved by Royan ethics committee. Statistical analysis Data analysis was performed by means of SPSS version 13.0 software program. Appropriate statistical analysis was performed using χ2 and student t-tests. p-values of <0.05 were considered statistically significant. Results In this study, the characteristics and treatment cycle results of patients compared separately between; 1) Women with endometriosis (whole stages) and reference group (tubal infertility) 2) Women with minimal to mild endometriosis (Stage I/II endometriosis) and reference group 3) Women with moderate to severe endometriosis (Stage III/IV endometriosis) and reference group and 4 Women withstage I/II and stage III/IVendometriosis (Tables I and II show the overall results). In comparison of women with endometriosis and women with tubal infertility, no significant differences were seen in the age, body mass index and duration of infertility (Table I). The women in compared groups were comparable in mean number of ampules of hMG, length of stimulation phase, number of mature oocytes (MII) and number of embryos transferred. The rate of moderate ovarian hyperstimulation syndrome was also similar in compared groups (Table II). No significant differences were found between the compared groups with regard to the implantation, pregnancy, miscarriage, ongoing pregnancy and twin birth rates (Table II). Our results showed that the percentage of previous pregnancy was significantly lower in women with endometriosis than women with tubal infertility (6.3% versus 21.1%, p=0.01). According to the results, women with endometriosis also had no history of ectopic pregnancy, while 8 women (14%) in tubal infertility group had previous ectopic pregnancy (p=0.001). As indicated in table II, we detected no differences in IVF/ ICSI outcomes when separately compared women with stages I/II endometriosis and those with stages III/IV disease with patients with tubal infertility. In comparison of stage III/ IV endometriosis and reference group, the mean duration of infertility was significantly lower in women with moderate to severe endometriosis before referral to our assisted reproductive centre.In comparing data in endometriosis patients with stage I/II and stage III/IV disease, no significant differences were observed in results of IVF/ICSI (details are presented in table II). In following of pregnancies, overall number of preterm labour was two (one case in each group). First trimester vanishing twin was observed in one case in tubal factor group. In two cases of the twin pregnancies in endometriosis-associated group, one of the babies died after birth in the 24th days of life due to major malformation and the other died after birth in 28th of gestational weeks because of LBW (both women had healthy singletons). The analysis had performed between endometriosis (whole stages) group in comparison with reference group, and also stage I/ II and stage IIIIV / groups together and separately in comparison with reference group. The differences between compared groups (endometriosis (Whole stages) group in comparison with reference group, comparison of stage I/ II and stage IV / III groups together and separately in comparison with reference group) were Non Significant. Discussion Endometriosis is a known cause of subfertility characterized by the presence of ectopic endometrial glands and stroma and a significant number of child-bearing aged women are affected by endometriosis (2, 15, 16). Several investigators have found that the duration of hMG used, dosages of gonadotropins, number of oocytes in the endometriosis–associated group were similar to control group (1, 4, 11). But in the study of Matalliotakis and colleagues (2007), patients with endometriosis required higher dosages of gonadotropins and yielded lower number of oocytes (7). The present study indicated no such differences between the study groups and tubal factor infertility. Our observation demonstrated that implantation and pregnancy rates were similar in both groups. Some studies also corroborate our data (5-7, 17).Basically, it has been reported that produced cytokines by activated macrophages in peritoneal cavity might have an adverse effect on the follicle, the oocytes, sperm function and gamete interaction or contribute an unsuitable environment for fertilization, and "with IVF/ICSI, the oocyte is not in contact with the peritoneal fluid"(5). Speculating, the presence of endometriosis decreases pregnancy rates for couples who make an effort for conception without ART or with ovulation induction (2). Apparently, Diaz et al (2000) showed that women with advanced endometriosis, receiving oocytes from non-endometriotic ovaries, had an implantation and pregnancy rate similar to that of recipient without endometriosis. This suggests that endometrial receptivity is not impaired in women with endometriosis (18). While in a meta-analysis by Barnhart and associates as well as Surrey et al (2002) the negative effect of endometriosis on implantation and pregnancy rates compared with tubal factor infertility was observed (2, 19). In most studies, the abortion rate was not found to be affected in women with endometriosis when compared with the control group (1, 5, 7, 20). Our results also showed no significant difference in rate of pregnancy loss between two groups. The ongoing pregnancy and twin birth rates had no significant differences between women with endometriosis and tubal infertility, similar to some other studies (7, 11). Analysis of our data indicates that women with endometriosis had no history of ectopic pregnancy, while 14% of women with tubal infertility group had previous ectopic pregnancy. On the basis of studies, history of ectopic pregnancy suggests the possibility of tubal damage and dysfunction (21). Hajenius and associates (2000) reported that tubal patency rate among women with ectopic pregnancy, who desire future fertility, is 80-90% (22), and in another study the OR for tubal pathology after a previous ectopic pregnancy was reported 8.4% (95% CI 6.3 to 12)(23). According to the results of present study, the percentage of previous pregnancy was significantly lower in women with endometriosis than control group. However there was no significant difference in pregnancy result between two groups of endometriosis and tubal factor in patients with history of pregnancy (p=0.28) and patients with no previous pregnancy (p=0.82). We also compared the outcomes of women with stage I/II endometriosis and women with stage III/IV endometriosis with reference group separately.We detected that severity of disease doesn't have adverse effect on IVF/ICSI outcome. Some authors demonstrated the lower success of IVF with an increase in severity of the disease (1, 2, 12, 24). Conversely, there have been several studies with no differences in IVF pregnancy rates for women with moderate to severe endometriosis than control group (20, 25, 26). Matalliotakis and colleagues, reported higher gonadotropin requirements, lower oocyte yield in women with advanced stage endometriosis versus women with tubal infertility. However they didn’t find any differences in implantation, pregnancy, and delivery rates between the severe endometriosis and tubal factor (7). In the study of Aboulghar et al (2003) no significant differences in mean number of hMG ampules and number of stimulation days observed between patients with severe endometriosis and tubal disease, but the rates of implantation, clinical pregnancy and multiple pregnancy were significantly higher in tubal infertility group (4). We also performed analysis to compare IVF outcome of women with mild and severe endometriosis. Some investigators reported that women with severe endometriosis have a significantly lower implantation and pregnancy rate, versus women with mild endometriosis (2, 12, 13).These results differ from our study which showed no differences in IVF/ICSI outcome between stages of endometriosis. Similarly in the analysis of other studies, no difference observed in pregnancy rate between women with either stage I/II and stage III/IV disease (17, 20, 25- 27). As indicated, the results of current study showed that the duration of infertility was significantly lower in women with moderate to severe endometriosis than tubal infertility. The etiology is unknown, but an explanation for the present result, might be duo to the clear symptoms of endometriosis than tubal disease, as endometriosis is the most common known cause of pelvic pain. Furthermore dyspareunia, dyschezia, cyclical dysuria and extreme fatigue are all common in women with endometriosis (3, 28). Thus these patients might refer to doctor sooner for their treatment. Kuivasaari et al (2005) reported that the infertility history of women with moderate to severe endometriosis was a few months shorter than women with less severe disease (1). As over the past two decades, there has been a steady decrease in diagnosis of advanced endometriosis at first diagnosis (15). In conclusion, this study showed thatendometriosis does not seem to have adverse effect on ovarian response, quality of oocytes and pregnancy outcome as compared with tubal infertility. Acknowledgement The authors wish to thank the staff of Royan Institute and Tehran University of Medical Sciences especially Mrs. Nabavi for their cooperation. References
© Copyright 2009 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm09001t2.jpg] |
| |||||||||

{kind=link}