 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 7, No. 1, Winter, 2009, pp. 41-43 Case report A ruptured tubo-ovarian abscess after intrauterine insemination; a case report Sanam Moradan M.D. Department of Obstetrics and Gynecology, Amir
University Hospital, Semnan University of Medical Sciences, Semnan, Iran. Received: 16 September 2008; accepted: 11 March 2009 Code Number: rm09008 Abstract Background:Pelvic inflammatory disease
is one of the most serious infection and one of the important and life
threatening complications of it is tubo-ovarian abscess. This infection with
intrauterine insemination (IUI) is rare. We report a case of ruptured tubo-
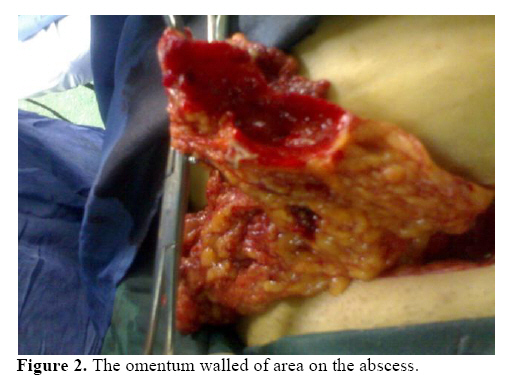
ovarian abscess after (IUI). Key words: Pelvic inflammatory disease, Tubo-ovarian abscess, Intrauterine insemination. Introduction Pelvic inflammatory disease is one of the most serious infections facing women. Untreated or unsuccessfully treated women may suffer from life – threatening consequences and even adequately treated women are at much higher risk for potentially serious sequel (1). It is a polymicrobial infection typically occurs in sexually active females and occurs in about 1% to 2% of young, sexually active women each year (1, 2). It occurs in women age 16 to 25 years and the resultant morbidity exceeds all other infections morbidity for this age group (1). Other risk factors are contraceptive methods such as IUD (3) sexual activity and previous episodes of PID (4). One of the important complications of PID is Tubo-ovarian abscess and it is represent a severe form of PID (5). A ruptured Tubo-ovarian abscess is a life threatening surgical emergency because gram negative endotoxic shock can develop rapidly. The treatment of unruptured tubo-ovarian abscesses is medical with appropriate intravenous antibiotics and close monitoring to detect leakage or impending rupture. A rupture tubo-ovarian abscess rapidly leads to diffuse peritonitis evidenced by tachycardia, rebound tenderness in all 4 quadrants of the abdomen and if progressive, hypotention and oliguria. Exploratory laparatomy with resection of infected tissue is mandatory (6). Before antibiotic therapy, the mortality rate associated with acute PID was 1% and most deaths resulted from ruptured tubo-ovarian abscesses. Today, death associated with PID is rare, but the mortality rate can still be as high as 5% to 10% for ruptured tubo-ovarian abscesses and mostly is the result of subsequent development of adult respiratory distress syndrome (ARDS), a condition is associated with serious infection (1). Pelvic inflammatory infection with IUI is rare, probably in the range of 1 in 500 inseminations but intratubal transfer of sperm could increase the risk of infection (7). In this report we had a case of ruptured tubo-ovarian abscess after IUI which is rare. Case report A 27 years old woman, Gravid 1, abortion 1, presented with chief complaint of acute abdominal pain and fever about one week after IUI. The patient was infertile and her marriage date was 6 years ago. The cause of infertility was male factor and the patient under went ovulation induction and IUI. Three days before IUI the patient was visited by gynecologist and there weren't any sign or symptoms of PID and pelvic examination was normal. So IUI was performed for the patient, 1 week later she was referred with chief complaint of acute abdominal pain and in physical examination the patient was febrile (tem: 38oC) and had tachycardia (PR: 105/min). In abdominal examination there was generalized tenderness with more dominant in left lower quadrant area. There was slightly rebound tenderness in all four quadrant of abdomen, in pelvic examination there was cervical motion and bilateral adenexal tenderness with severe cervical purulent discharge. In lab workup there was leukocytosis (WBC: 19.7X1000/cumm) and hypoalbuminemia (3.3g/dl). Abdominal sonography on the 1st day of admission was normal. So, the patient was a case of PID and intravenous antibiotic therapy with ceftriaxone 1 gram BD, metronidazole 500 mg TDS and gentanycin 80 mg BD was launched but even with treatment there wasn't clinical or para clinical improvement and in third day of admission the temp was 39.2 and there was more tenderness in abdominal exam. Therefore, laparatomy was performed. There were scattered pusy discharge in the entire abdominal cavity and left fallopian tube ruptured abscess was detected with momentum walled off on this tube. Therefore this was a case of PID and tubal abscess formation after IUI, so left salpingectomy and washing of abdominal cavity with 4 litter of fluid was performed. In post operation the same intravenous antibiotics therapy were continued and the patient was afebrile about 24 hours after surgery. The patient developed dyspnea and tachypnea in second day post operation and echocardiography with spiral CT scan was normal. Therefore a mild ARDS as a complication of tubal abscess was considered. But with continuing of IV antibiotic and oxygen therapy the patient was in a good condition 5 days after operation and was discharged from hospital in the same day. Discussion About 85% of PID cases are naturally occurring infections in sexually active female of reproductive age .The remaining 15% of infection occurs after procedures that break the cervical mucous barrier such as placement of an intrauterine device (1, 3, 8), endometrial biopsy, uterine curettage, hysteroscopy, and hysterosalpingography (1). Genital Chlamydial infections have been associated with problems in insemination and attempts at invitro fertilization (9). Infection with intrauterine insemination is rare, probably in the range of 1 in 500 inseminations (7). The squeals of PID are infertility, ectopic pregnancy, chronic pelvic pain, tubo-ovarian abscess or complex and mortality (1, 10, 11). Over 25% of women who develop acute PID suffer from these long term complications (12). Tubo-ovarian abscess are usually bilateral but unilateral abscess formation is not rare. The symptoms and sings are similar to those of acute salpingitis although pain and fever have been presents for longer than 1 week before presentation to the emergency room (12) and transvaginal ultrasonography could be a suitable diagnostic tool of tubo-ovarian abscess (13). In this case report we encountered with a ruptured tubal abscess formation after intrauterine insemination and it deserve to report. Because it is rare after IUI procedure and was unilateral abscess and the patient developed mild ARDS. References
© Copyright 2009 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm09008f2.jpg] [rm09008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}